Objective: There are many models to predict extracapsular extension (ECE) in patients with prostate cancer. We aimed to externally validate several models in a Japanese cohort.
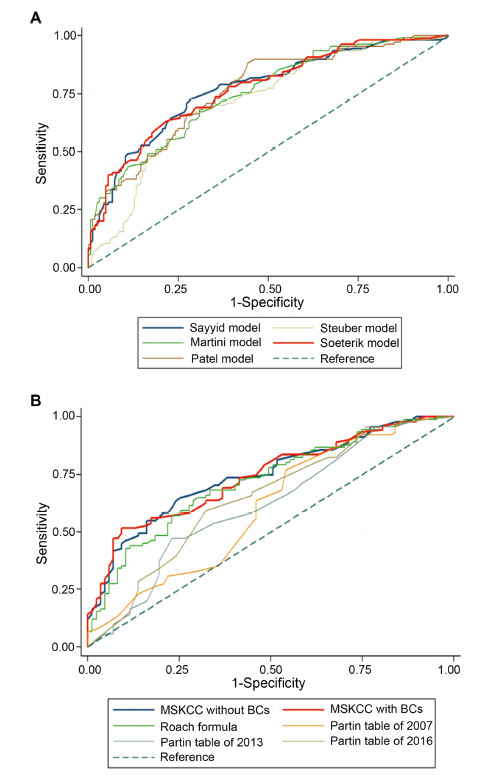
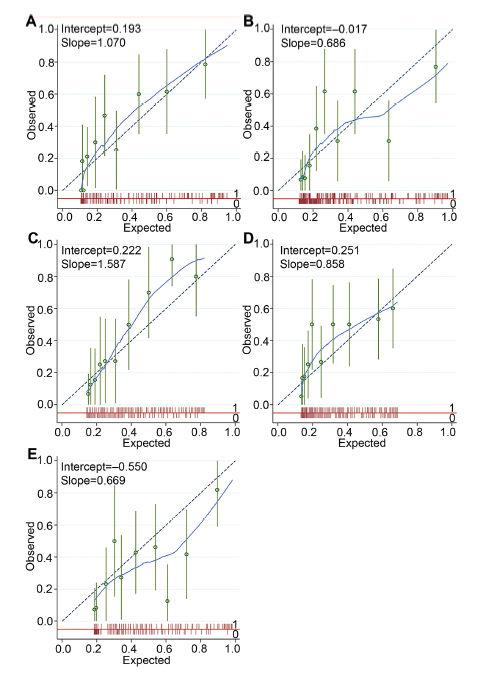
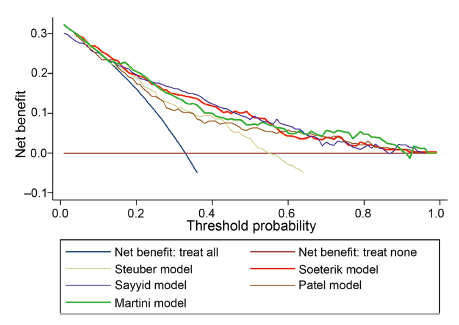
Methods: We included patients treated with robotic-assisted radical prostatectomy for prostate cancer. The risk of ECE was calculated for each patient in several models (prostate side-specific and non-side-specific). Model performance was assessed by calculating the receiver operating curve and the area under the curve (AUC), calibration plots, and decision curve analyses.
Results: We identified ECE in 117 (32.9%) of the 356 prostate lobes included. Patients with ECE had a statistically significant higher prostate-specific antigen level, percentage of positive digital rectal examination, percentage of hypoechoic nodes, percentage of magnetic resonance imaging nodes or ECE suggestion, percentage of biopsy positive cores, International Society of Urological Pathology grade group, and percentage of core involvement. Among the side-specific models, the Soeterik, Patel, Sayyid, Martini, and Steuber models presented AUC of 0.81, 0.78, 0.77, 0.75, and 0.73, respectively. Among the non-side-specific models, the memorial Sloan Kettering Cancer Center web calculator, the Roach formula, the Partin tables of 2016, 2013, and 2007 presented AUC of 0.74, 0.72, 0.64, 0.61, and 0.60, respectively. However, the 95% confidence interval for most of these models overlapped. The side-specific models presented adequate calibration. In the decision curve analyses, most models showed net benefit, but it overlapped among them.
Conclusion: Models predicting ECE were externally validated in Japanese men. The side-specific models predicted better than the non-side-specific models. The Soeterik and Patel models were the most accurate performing models.
- PSA, clinical T-stage, total Gleason score, percentage of positive BCs, percentage of cancer in biopsy specimen
0.73 (0.68-0.78)
Sayyid
- Age, PSA, clinical T-stage, total Gleason score, maximum percentage of core involvement, percentage of positive BCs, hypoechoic nodule
0.77 (0.71-0.82)
Martini
- PSA, total Gleason score, maximum percentage of core involvement, ECE in MRI
0.75 (0.70-0.81)
Patel
- Age, PSA, total Gleason score in positive core, clinical T-stage, percentage of in tumor positive
0.78 (0.73-0.83)
Non-side-specific model
Roach formula
- PSA, total Gleason score
0.72 (0.64-0.79)
Partin tables
Makarov
- PSA, clinical T-stage, total Gleason score
0.60 (0.51-0.68)
Eifel
- PSA, clinical T-stage, total Gleason score
0.61 (0.53-0.70)
Tosoian
- PSA, clinical T-stage, total Gleason score
0.64 (0.56-0.73)
MSKCC
Web calculator (incl. BCs)
- Age, PSA, clinical T-stage, primary and secondary Gleason, percentage of BCs
0.74 (0.67-0.81)
Web calculator (excl. BCs)
- Age, PSA, clinical T-stage, primary and secondary Gleason
0.74 (0.67-0.81)
[1]
Patel VR, Sivaraman A, Coelho RF, Chauhan S, Palmer KJ, Orvieto MA, et al. Pentafecta: a new concept for reporting outcomes of robot-assisted laparoscopic radical prostatec-tomy. Eur Urol 2011; 59:702e7.
doi: 10.1016/j.eururo.2011.01.032
[2]
Reeves F, Preece P, Kapoor J, Everaerts W, Murphy DG, Corcoran NM, et al. Preservation of the neurovascular bundles is associated with improved time to continence after radical prostatectomy but not long-term continence rates: results of a systematic review and meta-analysis. Eur Urol 2015; 68: 692e704.
doi: 10.1016/j.eururo.2014.10.020
pmid: 25454614
[3]
Druskin SC, Liu JJ, Young A, Feng Z, Dianat SS, Ludwig WW, et al. Prostate MRI prior to radical prostatectomy: effects on nerve sparing and pathological margin status. Res Rep Urol 2017; 9:55e63.
doi: 10.2147/RRU.S128499
pmid: 28459044
[4]
Martini A, Marqueen KE, Falagario UG, Waingankar N, Wajswol E, Khan F, et al. Estimated costs associated with radiation therapy for positive surgical margins during radical prostatectomy. JAMA Netw Open 2020; 3:e201913. https://doi.org/10.1001/jamanetworkopen.2020.1913.
doi: 10.1001/jamanetworkopen.2020.1913
[5]
Magi-Galluzzi C, Evans AJ, Delahunt B, Epstein JI, Grif?ths DF, van der Kwast TH, et al. International Society of Urological Pathology (ISUP) consensus conference on handling and stag-ing of radical prostatectomy specimens. Working group 3: extraprostatic extension, lymphovascular invasion and locally advanced disease. Mod Pathol 2011; 24:26e38.
doi: 10.1038/modpathol.2010.158
[6]
Amling CL, Blute ML, Lerner SE, Bergstralh EJ, Bostwick DG, Zincke H. Influence of prostate-speci?c antigen testing on the spectrum of patients with prostate cancer undergoing radical prostatectomy at a large referral practice. Mayo Clin Proc 1998; 73:401e6.
pmid: 9581578
[7]
Mottet N, van den Bergh RCN, Briers E, Van den Broeck T, Cumberbatch MG, De Santis M, et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancerd2020 update. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2021; 79:243e62.
doi: 10.1016/j.eururo.2020.09.042
[8]
Somford DM, Hamoen EH, Fütterer JJ, van Basten JP, Hulsber-gen-van de Kaa CA, Vreuls W, et al. The predictive value of endorectal 3 Tesla multiparametric magnetic resonance imag-ing for extraprostatic extension in patients with low, interme-diate and high risk prostate cancer. J Urol 2013;190: 1728e34.
[9]
Mohler JL, Antonarakis ES, Armstrong AJ, D’Amico AV, Davis BJ, Dorff T, et al. Prostate cancer, version 2.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Netw 2019; 17:479e505.
[10]
de Rooij M, Hamoen EHJ, Witjes JA, Barentsz JO, Rovers MM. Accuracy of magnetic resonance imaging for local staging of prostate cancer: a diagnostic meta-analysis. Eur Urol 2016; 70: 233e45.
doi: 10.1016/j.eururo.2015.07.029
pmid: 26215604
[11]
Gandaglia G, De Lorenzis E, Novara G, Fossati N, De Groote R, Dovey Z, et al. Robot-assisted radical prostatectomy and extended pelvic lymph node dissection in patients with locally-advanced prostate cancer. Eur Urol 2017; 71:249e56.
doi: S0302-2838(16)30172-5
pmid: 27209538
[12]
Yuh B, Artibani W, Heidenreich A, Kimm S, Menon M, Novara G, et al. The role of robot-assisted radical prostatectomy and pelvic lymph node dissection in the management of high-risk prostate cancer: a systematic review. Eur Urol 2014; 65:918e27.
doi: 10.1016/j.eururo.2013.05.026
pmid: 23721959
[13]
Sayyid R, Perlis N, Ahmad A, Evans A, Toi A, Horrigan M, et al. Development and external validation of a biopsy-derived nomogram to predict risk of ipsilateral extraprostatic exten-sion. BJU Int 2017; 120:76e82.
doi: 10.1111/bju.13733
[14]
Martini A, Gupta A, Lewis SC, Cumarasamy S, Haines 3rd KG, Briganti A, et al. Development and internal validation of a side-speci?c, multiparametric magnetic resonance imaging-based nomogram for the prediction of extracapsular exten-sion of prostate cancer. BJU Int 2018; 122:1025e33.
doi: 10.1111/bju.14353
[15]
Patel VR, Sandri M, Grasso AAC, De Lorenzis E, Palmisano F, Albo G, et al. A novel tool for predicting extracapsular extension during graded partial nerve sparing in radical prostatectomy. BJU Int 2018; 121:373e82.
doi: 10.1111/bju.14026
pmid: 28941058
[16]
Steuber T, Graefen M, Haese A, Erbersdobler A, Chun FK, Schlom T, et al. Validation of a nomogram for prediction of side speci?c extracapsular extension at radical prostatec-tomy. J Urol 2006; 175:939e44.
doi: 10.1016/S0022-5347(05)00342-3
pmid: 16469587
[17]
Soeterik TFW, Dijksman LM, Ku¨sters-Vandevelde H, Stomps S, Schoots IG, et al. Development and external validation of a novel nomogram to predict side-speci?c extraprostatic extension in patients with prostate cancer undergoing radical prostatectomy. Eur Urol Oncol 2020;S2588e9311:30133e4. https://doi.org/10.1016/j.euo.2020.08.008.
[18]
Memorial Sloan Kettering Cancer Center. Pre-radical prosta-tectomy tool to predict probability of lymph node involve-ment in prostate cancer patients. www.mskcc.org/nomograms/prostate/pre_op. [Accessed 6 June 2021].
[19]
Makarov DV, Trock BJ, Humphreys EB, Mangold LA, Walsh PC, Epstein JI, et al. Updated nomogram to predict pathologic stage of prostate cancer given prostate-speci?c antigen level, clinical stage, and biopsy Gleason score (Partin tables) based on cases from 2000 to 2005. Urology 2007; 69:1095e101.
[20]
Eifler JB, Feng Z, Lin BM, Partin MT, Humphreys EB, Han M, et al. An updated prostate cancer staging nomogram (Partin tables) based on cases from 2006 to 2011. BJU Int 2013; 111: 22e9.
[21]
Tosoian JJ, Chappidi M, Feng Z, Humphreys EB, Han M, Pavlovich CP, et al. Prediction of pathological stage based on clinical stage, serum prostate-speci?c antigen, and biopsy Gleason score: Partin tables in the contemporary era. BJU Int 2017; 119:676e83.
[22]
Sanda MG, Cadeddu JA, Kirkby E, Chen RC, Crispino T, Fontanarosa J, et al. Clinically localized prostate cancer: AUA/ASTRO/SUO guideline.Part II: recommended ap-proaches and details of speci?c care options. J Urol 2018; 199:990e7.
doi: 10.1016/j.juro.2018.01.002
[23]
Kakehi Y, Sugimoto M, Taoka R. Evidenced-based clinical prac-tice guideline for prostate cancer (summary: Japanese Urologi-cal Association, 2016 edition). Int J Urol 2017; 24:648e66.
doi: 10.1111/iju.13380
[24]
Murakami T, Otsubo S, Namitome R, Shiota M, Inokuchi J, Takeuchi A, et al. Clinical factors affecting perioperative outcomes in robot-assisted radical prostatectomy. Mol Clin Oncol 2018; 9:575e81.
doi: 10.3892/mco.2018.1718
pmid: 30279989
[25]
Naito S, Kuroiwa K, Kinukawa N, Goto K, Koga H, Ogawa O, et al. Validation of Partin tables and development of a pre-operative nomogram for Japanese patients with clinically localized prostate cancer using 2005 International Society of Urological Pathology consensus on Gleason grading: data from the clinicopathological. J Urol 2008; 180:904e10.
doi: 10.1016/j.juro.2008.05.047
[26]
D’Amico AV, Whittington R, Bruce Malkowicz S, Schultz D, Blank K, Broderick GA, et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. J Am Med Assoc 1998; 280:969e74.
doi: 10.1001/jama.280.11.969
[27]
Roach M, Marquez C, Yuo HS, Narayan P, Coleman L, Nseyo UO, et al. Predicting the risk of lymph node involve-ment using the pre-treatment prostate speci?c antigen and Gleason score in men with clinically localized prostate cancer. Int J Radiat Oncol Biol Phys 1994; 28:33e7.
doi: 10.1016/0360-3016(94)90138-4
[28]
Hosmer JDW, Lemeshow S, Sturdivant RX. Applied logistic regression. 3rd ed. USA: John Wiley & Sons; 2013. p. 177.
[29]
Vickers AJ, van Calster B, Steyerberg EW. A simple, step-by-step guide to interpreting decision curve analysis. Diagnostic Progn Res 2019; 3:1e8.
doi: 10.1186/s41512-019-0047-8
[30]
Rocco B, Sighinol? MC, Sandri M, Eissa A, Elsherbiny A, Zoeir A, et al. Is extraprostatic extension of cancer predictable? A review of predictive tools and an external validation based on a large and a single center cohort of prostate cancer patients. Urology 2019; 129:8e20.
doi: S0090-4295(19)30316-4
pmid: 30928608
[31]
Martini A, Soeterik TFW, Haverdings H, Rahota RG, Checcucci E, De Cillis S, et al. An algorithm to personalize nerve sparing in men with unilateral high-risk prostate cancer. J Urol 2022; 207:350e7.
doi: 10.1097/JU.0000000000002205
[32]
Soeterik TFW, Dijksman LM, Küsters-Vandevelde HVN, Biesma DH, Witjes JA, et al. External vali-dation of the Martini nomogram for prediction of side-speci?c extraprostatic extension of prostate cancer in patients un-dergoing robot-assisted radical prostatectomy. Urol Oncol Semin Orig Investig 2020; 38:372e8.
[33]
Song C, Ro JY, Lee MS, Hong SJ, Chung BH, Choi HY, et al. Prostate cancer in Korean men exhibits poor differentiation and is adversely related to prognosis after radical prostatec-tomy. Urology 2006; 68:820e4.
doi: 10.1016/j.urology.2006.04.029
[34]
Byun SS, Lee S, Lee SE, Lee E, Seo SI, Lee HM, et al. Recent changes in the clinicopathologic features of Korean men with prostate cancer: a comparison with Western populations. Yonsei Med J 2012; 53:543e9.
doi: 10.3349/ymj.2012.53.3.543
[35]
Epstein JI, Carmichael MJ, Pizov G, Walsh v. Influence of capsular penetration on progression following radical prosta-tectomy: a study of 196 cases with long-term followup. J Urol 1993; 150:135e41.
doi: 10.1016/s0022-5347(17)35415-0
pmid: 7685422
[36]
Sung MT, Lin H, Koch MO, Davidson DD, Cheng L. Radial dis-tance of extraprostatic extension measured by ocular micro-meter is an independent predictor of prostate-speci?c antigen recurrence: a new proposal for the substaging of pT3a pros-tate cancer. Am J Surg Pathol 2007; 31:311e8.
doi: 10.1097/01.pas.0000213359.26003.37
[37]
Ball MW, Partin AW, Epstein JI. Extent of extraprostatic extension independently influences biochemical recurrence-free survival: evidence for further PT3 subclassi?cation. Urology 2015; 85:161e4.
doi: 10.1016/j.urology.2014.08.025
[38]
Jeong BC, Chal?n HJ, Lee SB, Feng Z, Epstein JI, Trock BJ, et al. The relationship between the extent of extraprostatic extension and survival following radical prostatectomy. Eur Urol 2015; 67:342e6.
doi: 10.1016/j.eururo.2014.06.015
pmid: 24968968
[39]
Hou Y, Zhang YH, Bao J, Bao ML, Yang G, Shi HB, et al. Arti-?cial intelligence is a promising prospect for the detection of prostate cancer extracapsular extension with mpMRI: a two-center comparative study. Eur J Nucl Med Mol Imaging 2021; 48:3805e16.
doi: 10.1007/s00259-021-05381-5