Reliability of nephrolithometric nomograms in patients treated with minimally invasive percutaneous nephrolithotomy: A precision study
a Department of Urology, San Bassiano Hospital, Bassano del Grappa, Italy b Department of Urology, University of Trieste, Trieste, Italy c Institute of Urology, University College Hospitals London, London, UK d Department of Urology, Minimally Invasive Centre, the first affiliated hospital of Guangzhou Medical University, Guangzhou, China
Objectives: The study aimed to evaluate quality of nephrolithometric nomograms to predict stone-free rates (SFRs) and complication rates (CRs) in case of minimally invasive percutaneous nephrolithotomy (PNL). In the last decade, nomograms have been introduced to estimate the SFRs and CRs of PNL. However, no data are available regarding their reliability in case of utilization of miniaturized devices. Herein we present a prospective multicentric study to evaluate reliability of Guy’s stone score (GSS), the stone size, tract length, obstruction, number of involved calyces, and essence of stone (S.T.O.N.E.) nephrolithometry score and Clinical Research Office of the Endourological Society (CROES) score in patients treated with minimally invasive PNL.
Methods:We evaluated SFRs and CRs of 222 adult patients treated with miniaturized PNL. Patients were considered stone-free if no residual fragments of any size at post-operative unenhanced computed tomography scan. Patients demographics, SFRs, and CRs were reported and analyzed. Performances of nomograms were evaluated with the area under the curve (AUC).
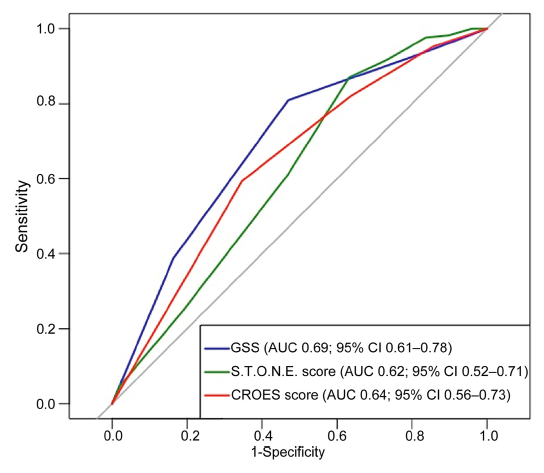
Results:We included 222 patients, the AUCs of GSS, CROES score, and S.T.O.N.E. nephrolithometry score were 0.69 (95% confidence interval [CI] 0.61-0.78), 0.64 (95% CI 0.56-0.73), and 0.62 (95% CI 0.52-0.71), respectively. Regarding SFRs, at multivariate binomial logistic regression, only the GSS had significance with an odds ratio of 0.53 (95% CI 0.31-0.95, p=0.04). We did not find significant correlation with complications, with only a trend for GSS.
Conclusion:This is the first study evaluating nomograms in miniaturized PNL. They still show good reliability; however, our data showed lower performances compared to standard PNL. We emphasize the need of further studies to confirm this trend. A dedicated nomogram for minimally invasive PNL may be necessary.
Displaced stent requiring repositioning under general anesthesia
1 (0.5)
Sepsis without organ failure requiring supportive therapy
1 (0.5)
Grade IIIb
1 (0.5)
Angio-embolization
1 (0.5)
Grade IVa
4 (1.8)
Sepsis requiring ICU stay
3 (1.4)
Pulmonary embolism requiring ICU stay
1 (0.5)
Variable
Univariate
Multivariate
OR (95% CI)
p-Value
OR (95% CI)
p-Value
Agea, years
0.99 (0.97-1.01)
0.48
Sex
Male
1.00 (Ref.)
Female
0.69 (0.36-1.31)
0.26
Side
Left
1.00 (Ref.)
Right
1.35 (0.71-2.58)
0.36
Stone burdena, mm2
0.99 (0.99-1.00)
<0.001
1.00 (0.99-1.00)
0.04
Tract lengtha
1.01 (0.99-1.02)
0.16
Renal pelvic obstruction
None or mild
1.00 (Ref.)
Moderate or severe
0.83 (0.42-1.67)
0.83
Number of calyxes involveda
0.75 (0.56-1.00)
0.05
1.36 (0.98-2.65)
0.21
Stone density (HU)a
0.99 (0.99-1.00)
0.18
Prior treatment
No
1.00 (Ref.)
PNL
1.28 (0.41-4.63)
0.67
ESWL
1.31 (0.08-NA)
0.99
Endoscopic
1.36 (0.24-NA)
0.99
Multiple
1.82 (0.52-54.36)
0.33
Presence of staghorn
No
1.00 (Ref.)
Yes
0.25 (0.12-0.48)
<0.001
0.30 (0.11-0.72)
0.01
Number of stones
Single
1.00 (Ref.)
Multiple
0.32 (0.14-0.66)
0.03
0.42 (0.18-0.91)
0.03
Guy’s stone scorea
0.47 (0.33-0.67)
<0.001
0.53 (0.31-0.95)
0.04
S.T.O.N.E. nephrolithometry scorea
0.71 (0.57-0.86)
0.001
0.95 (0.66-1.34)
0.69
CROES scorea
1.71 (1.24-2.37)
0.001
0.89 (0.41-1.74)
0.68
AUC of the model
0.72 (0.70-0.76)
Parameter
GSS
S.T.O.N.E. nephrolithometry score
CROES score
AUC (95% CI)
0.69 (0.61-0.78)
0.62 (0.52-0.71)
0.64 (0.56-0.73)
Accuracy (95% CI)
0.75 (0.50-0.81)
0.76 (0.61-0.81)
0.61 (0.55-0.77)
Best threshold
2.5
7.5
202
Sensitivity (95% CI)
0.81 (0.75-0.88)
0.87 (0.62-0.98)
0.59 (0.53-0.86)
Specificity (95% CI)
0.53 (0.41-0.68)
0.37 (0.18-0.61)
0.65 (0.31-0.78)
NPV (95% CI)
0.44 (0.29-0.55)
0.45 (0.31-0.71)
0.32 (0.27-0.47)
PPV (95% CI)
0.86 (0.83-0.93)
0.83 (0.80-0.86)
0.86 (0.80-0.91)
[1]
Turk C, Petrik A, Sarica K, Seitz C, Skolarikos A, Straub M, et al. EAU guidelines on interventional treatment for urolith-iasis. Eur Urol 2016; 69:475e82.
doi: 10.1016/j.eururo.2015.07.041
[2]
Assimos D, Krambeck A, Miller NL, Monga M, Murad MH, Nelson CP, et al. Surgical management of stones: American Urological Association/Endourological Society guideline, Part I. J Urol 2016; 196:1153e60.
doi: 10.1016/j.juro.2016.05.090
pmid: 27238616
[3]
Bryniarski P, Paradysz A, Zyczkowski M, Kupilas A, Nowakowski K, Bogacki R. A randomized controlled study to analyze the safety and ef?cacy of percutaneous nephrolithotripsy and retrograde intrarenal surgery in the management of renal stones more than 2 cm in diameter. J Endourol 2012; 26:52e7.
doi: 10.1089/end.2011.0235
pmid: 22003819
[4]
de la Rosette JJ, Opondo D, Daels FP, Giusti G, Serrano A, Kandasami SV, et al. Categorisation of complications and validation of the Clavien score for percutaneous neph-rolithotomy. Eur Urol 2012; 62:246e55.
doi: 10.1016/j.eururo.2012.03.055
pmid: 22487016
[5]
Armitage JN, Irving SO, Burgess NA; British Association of Urological Surgeons Section of Endourology. Percutaneous nephrolithotomy in the United Kingdom: results of a pro-spective data registry. Eur Urol 2012; 61:1188e93.
doi: 10.1016/j.eururo.2012.01.003
pmid: 22244778
[6]
Jackman SV, Docimo SG, Cadeddu JA, Bishoff JT, Kavoussi LR, Jarrett TW. The "mini-perc" technique: a less invasive alternative to percutaneous nephrolithotomy. World J Urol 1998; 16:371e4.
doi: 10.1007/s003450050083
pmid: 9870281
[7]
Lahme S, Zimmermanns V, Hochmuth A, Janitzki V. [Minimally invasive PCNL (mini-perc). Alternative treatment modality or replacement of conventional PCNL?]. Urologe 2008; 47:563e8.[Article in German].
doi: 10.1007/s00120-008-1708-3
Li X, He Z, Wu K, Li SK, Zeng G, Yuan J, et al. Chinese mini-mally invasive percutaneous nephrolithotomy: the Guangzhou experience. J Endourol 2009; 23:1693e7.
doi: 10.1089/end.2009.1537
[10]
Mishra S, Sharma R, Garg C, Kurien A, Sabnis R, Desai M. Prospective comparative study of miniperc and standard PNL for treatment of 1 to 2 cm size renal stone. BJU Int 2011; 108: 896e9.
doi: 10.1111/j.1464-410X.2010.09936.x
pmid: 21477212
[11]
Kamal W, Kallidonis P, Kyriazis I, Liatsikos E. Minituriazed percutaneous nephrolithotomy: what does it mean? Urolith-iasis 2016; 44:195e201.
[12]
Thomas K, Smith NC, Hegarty N, Glass JM. The Guy’s stone scoredgrading the complexity of percutaneous neph-rolithotomy procedures. Urology 2011; 78:277e81.
doi: 10.1016/j.urology.2010.12.026
pmid: 21333334
[13]
Okhunov Z, Friedlander JI, George AK, Duty BD, Moreira DM, Srinivasan AK, et al. S.T.O.N.E. nephrolithometry: novel sur-gical classi?cation system for kidney calculi. Urology 2013; 81: 1154e9.
doi: 10.1016/j.urology.2012.10.083
[14]
Opondo D, Gravas S, Joyce A, Pearle M, Matsuda T, Sun YH, et al. Standardization of patient outcomes reporting in percutaneous nephrolithotomy. J Endourol 2014; 28:767e74.
doi: 10.1089/end.2014.0057
pmid: 24571713
[15]
Al Adl AM, Mohey A, Abdel Aal A, Abu-Elnasr HAF, El Karamany T, Noureldin YA. Percutaneous nephrolithotomy outcomes based on S.T.O.N.E., GUY, CROES, and S-ReSC scoring systems: the ?rst prospective study. J Endourol 2020; 34:1223e8.
doi: 10.1089/end.2019.0856
[16]
Kumar S, Sreenivas J, Karthikeyan VS, Mallya A, Keshavamurthy R. Evaluation of CROES nephrolithometry nomogram as a preoperative predictive system for percutaneous nephrolithotomy outcomes. J Endourol 2016; 30:1079e83.
pmid: 27550775
[17]
Tailly TO, Okhunov Z, Nadeau BR, Huynh MJ, Labadie K, Akhavein A, et al. Multicenter external validation and com-parison of stone scoring systems in predicting outcomes after percutaneous nephrolithotomy. J Endourol 2016; 30:594e601.
doi: 10.1089/end.2015.0700
[18]
Zeng G, Wan S, Zhao Z, Zhu J, Tuerxun A, Song C, et al. Super-mini percutaneous nephrolithotomy (SMP): a new concept in technique and instrumentation. BJU Int 2016; 117:655e61.
doi: 10.1111/bju.13242
pmid: 26220396
[19]
Tiselius HG, Andersson A. Stone burden in an average Swedish population of stone formers requiring active stone removal: how can the stone size be estimated in the clinical routine? Eur Urol 2003; 43:275e81.
doi: 10.1016/S0302-2838(03)00006-X
[20]
Wu WJ, Okeke Z. Current clinical scoring systems of percu-taneous nephrolithotomy outcomes. Nat Rev Urol 2017; 14: 459e69.
doi: 10.1038/nrurol.2017.71
[21]
Mitropoulos D, Artibani W, Graefen M, Remzi M, Roupret M, Truss M, et al. Reporting and grading of complications after urologic surgical procedures: an ad hoc EAU guidelines panel assessment and recommendations. Eur Urol 2012; 61:341e9.
doi: 10.1016/j.eururo.2011.10.033
pmid: 22074761
[22]
Pietropaolo A, Proietti S, Geraghty R, Skolarikos A, Papatsoris A, Liatsikos E, et al. Trends of “urolithiasis: in-terventions, simulation, and laser technology” over the last 16 years (2000e2015) as published in the literature (PubMed): a systematic review from European section of Uro-technology (ESUT). World J Urol 2017; 35:1651e8.
doi: 10.1007/s00345-017-2055-z
[23]
Chung KJ, Kim JH, Min GE, Park HK, Li S, Del Giudice F, et al. Changing trends in the treatment of nephrolithiasis in the real world. J Endourol 2019; 33:248e53.
doi: 10.1089/end.2018.0667
pmid: 30628473
[24]
Ahmad AA, Alhunaidi O, Aziz M, Omar M, Al-Kandari AM, El-Nahas A, et al. Current trends in percutaneous nephrolithotomy: an internet-based survey. Ther Adv Urol 2017; 9:219e26.
doi: 10.1177/1756287217724726
[25]
Feng D, Hu X, Tang Y, Han P, Wei X. The ef?cacy and safety of miniaturized percutaneous nephrolithotomy versus standard percutaneous nephrolithotomy: a systematic review and meta-analysis of randomized controlled trials. Investig Clin Urol 2020; 61:115e26.
doi: 10.4111/icu.2020.61.2.115