|
|
|
| Can preoperative planning using IRIS™ three-dimensional anatomical virtual models predict operative findings during robot-assisted partial nephrectomy? |
Ahmed Ghazia,Nitin Sharmaa,*( ),Ahmed Radwanb,Hani Rashida,Thomas Osinskia,Thomas Fryea,William Tabayoyonga,Jonathan Blooma,Jean Josepha ),Ahmed Radwanb,Hani Rashida,Thomas Osinskia,Thomas Fryea,William Tabayoyonga,Jonathan Blooma,Jean Josepha
|
aUniversity of Rochester, Urology Department, Rochester, NY, USA
bAin Shams University, Urology Department, Cairo, Egypt |
|
|
|
|
Abstract Objective: To evaluate the predictive validity of IRIS™ (Intuitive Surgical®, Sunnyvale, CA, USA) as a planning tool for robot-assisted partial nephrectomy (RAPN) by assessing the degree of overlap with intraoperative execution. Methods: Thirty-one patients scheduled for RAPN by four experienced urologists were enrolled in a prospective study. Prior to surgery, urologists reviewed the IRIS™ three-dimensional model on an iphone Operating System (iOS) app and completed a questionnaire outlining their surgical plan including surgical approach, and ischemia technique as well as confidence in executing this plan. Postoperatively, questionnaires assessing the procedural approach, clinical utility, efficiency, and effectiveness of IRIS™ were completed. The degree of overlap between the preoperative and intraoperative questionnaires and between the planned approach and actual execution of the procedure was analyzed. Questionnaires were answered on a 5-point Likert scale and scores of 4 or greater were considered positive. Results: Mean age was 65.1 years with a mean tumor size of 27.7 mm (interquartile range 17.5-44.0 mm). Hilar tumors consisted of 32.3%; 48.4% of patients had R.E.N.A.L. nephrometry scores of 7-9. On preoperative questionnaires, the surgeons reported that in 67.7% cases they were confident that they can perform the procedure successfully, and on intraoperative questionnaires, the surgeons reported that in 96.8% cases IRIS™ helped achieve good spatial sensation of the anatomy. There was a high degree of overlap between preoperative and intraoperative questionnaires for the surgical approach, interpreting anatomical details and clinical utility. When comparing plans for selective or off-clamp, the preoperative plan was executed in 90.0% of cases intraoperatively. Conclusion: A high degree of overlap between the preoperative surgical approach and intraoperative RAPN execution was found using IRIS™. This is the first study to evaluate the predictive accuracy of IRIS™ during RAPN by comparing preoperative plan and intraoperative execution.
|
|
Received: 18 July 2022
Available online: 20 October 2023
|
|
Corresponding Authors:
*E-mail address: drsharmanitin@gmail.com (N. Sharma).
|
|
|
|
|
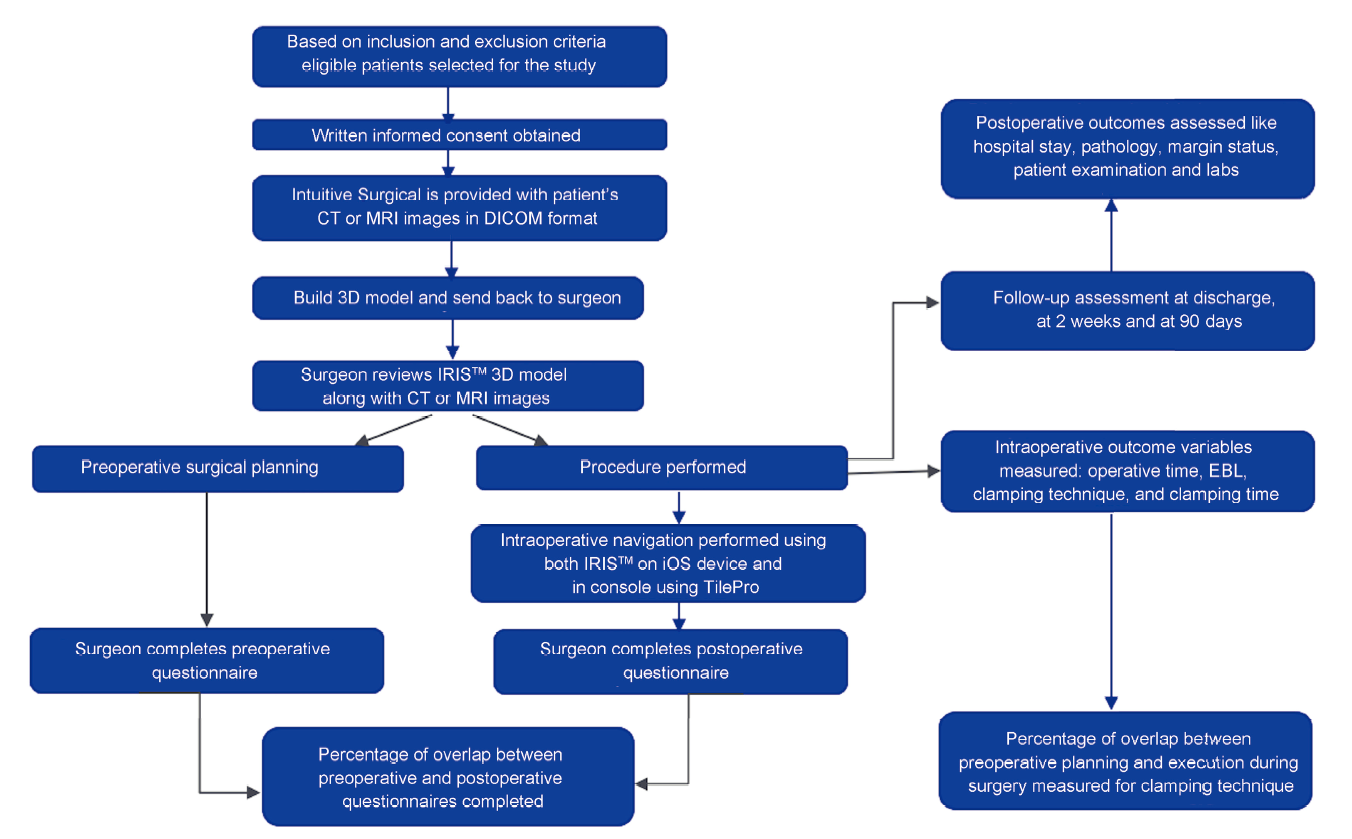
Study design. CT, computed tomography; MRI, magnetic resonance imaging; DICOM, Digital Imaging and Communications in Medicine; 3D, three-dimensional; EBL, expected blood loss; iOS, iphone Operating System.
|

| Criteria | Description | | Inclusion criteria | 1. Patient is 18 years or older | | 2. Patient should have or plan to have a contrast-enhanced CT scan or MRI | | Exclusion criteria | 1. Solitary or horseshoe kidney | | 2. More than two masses requiring multiple partial nephrectomies on the same side | | 3. Patient with prior partial nephrectomy on the affected side | | 4. Patient with renal vein or inferior vena cava thrombosis | | 5. Patient requiring bilateral partial nephrectomies | | 6. Metastatic disease with life expectancy less than 1 year | | 7. Pregnant or suspected pregnancy | | 8. Mentally handicapped, underlying psychological disorder or severe systemic illness precluding compliance with study requirements | | 9. Patient belonging to other vulnerable population, e.g., prisoner or ward of the state |
|
|
Inclusion and exclusion criteria for the study.
|
| Patient demographic | All patients for IRIS? (n=31) | R.E.N.A.L. nephrometry score | | 4-6 (n=8) | 7-9 (n=15) | 10-12 (n=8) | | Age, year | | | | | | Mean±SD | 65.1±14.9 | 55.5±21.4 | 70.1±7.4 | 65.4±14.9 | | Median (IQR) | 67.0 (57.0-74.0) | 57.0 (40.0-69.0) | 71.0 (63.0-74.0) | 66.5 (51.5-79.0) | | Gender (male:female) | 20:11 | 6:2 | 9:6 | 5:3 | | BMIa, kg/m2 | 30.6±6.5 | 27.7±3.3 | 32.1±7.7 | 30.9±6.0 | | ASA classification, n (%) | | | | | | Class 1 | 2 (6.5) | 2 (25.0) | 0 (0) | 0 (0) | | Class 2 | 12 (38.7) | 2 (25.0) | 7 (46.7) | 3 (37.5) | | Class 3 | 17 (54.8) | 4 (50.0) | 8 (53.3) | 5 (62.5) | | Class 4 | 0 (0) | 0 (0) | 0 (0) | 0 (0) | | Major abdominal surgery, n | 5 | 1 | 4 | 0 | | Laterality (left:right) | 11:20 | 4:4 | 6:9 | 1:7 | | Tumor location (anterior:hilar:posterior:other) | 11:10:9:1 | 5:0:3:0 | 5:4:5:1 | 1:6:1:0 | | Tumor sizea, mm | 27.7±17.3 | 26.5±18.9 | 25.3±12.4 | 33.1±23.5 | | Estimated hilar dissection timea, min | 12.5±8.5 | 12.5±8.5 | 11.7±9.0 | 25.0±20.6 | | Estimated tumor resection timea, min | 8.6±4.5 | 6.9±2.8 | 7.6±4.4 | 12.3±4.2 | | Estimated renorrhaphy timea, min | 12.8±7.3 | 10.3±3.9 | 14.7±13.7 | 16.5±8.5 | | LOSa, day | 1.7±1.1 | 1.1±0.4 | 1.7±1.1 | 2.3±1.3 |
|
|
Patient demographics, medical and surgical history, and surgical outcomes (grouped according to R.E.N.A.L. nephrometry scores).
|
|
|
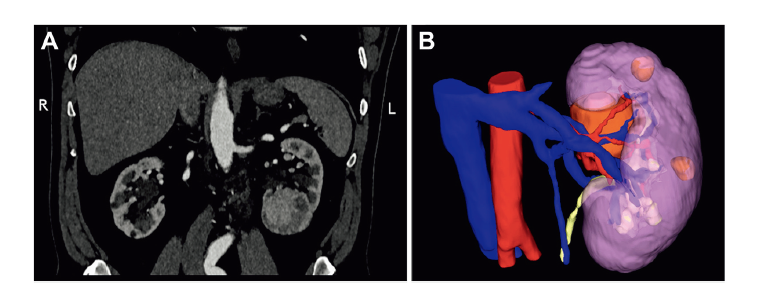
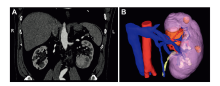
A patient with a complex left renal mass (R.E.N.A.L. nephrometry score of 10). (A) Coronal images of abdominal computerized tomography scan; (B) IRIS? three-dimensional virtual reconstruction image on iphone Operating System device (Apple Park, Cupertino, CA, USA) of the same patient. R, right; L, left.
|
| Preoperative questionnaires to surgeons' evaluating imaging using both IRIS? and CT scan | R.E.N.A.L. nephrometry score | All patients for IRIS? (n=31) | | 4-6 (n=8) | 7-9 (n=15) | 10-12 (n=8) | | Which part of the renal anatomy was IRIS? with CT scan helpful to achieve good spatial sensation | | Tumor location | 7 (87.5) | 15 (100.0) | 8 (100.0) | 30 (96.8) | | Renal artery identification | 7 (87.5) | 15 (100.0) | 8 (100.0) | 30 (96.8) | | Renal vein identification | 8 (100.0) | 15 (100.0) | 8 (100.0) | 31 (100.0) | | Tumor depth identification | 7 (87.5) | 15 (100.0) | 8 (100.0) | 30 (96.8) | | Relationship of tumor to surrounding structures | 6 (75.0) | 15 (100.0) | 8 (100.0) | 29 (93.5) | | Which part of the operation were you satisfied with the information available using IRIS? and CT scan | | Identification of ureter and vessels | 4 (50.0) | 11 (73.3) | 3 (37.5) | 18 (58.1) | | Identification of tumor location | 6 (75.0) | 15 (100.0) | 8 (100.0) | 29 (93.5) | | Identification of tumor depth | 6 (75.0) | 14 (93.3) | 8 (100.0) | 28 (90.3) | | Tumor resection for a complex tumor | 2 (25.0) | 8 (53.3) | 7 (87.5) | 17 (54.8) | | Aided in planning of off-clamp or segmental clamping | 3 (37.5) | 7 (46.7) | 4 (50.0) | 14 (45.2) | | Identification of feeding vessel to the tumor | 2 (25.0) | 11 (73.3) | 7 (87.5) | 20 (64.5) | | Not useful in this procedure | 1 (12.5) | 0 (0) | 0 (0) | 1 (3.2) | | You are confident that you will successfully complete the planned procedure | 8 (100.0) | 9 (60.0) | 4 (50.0) | 21 (67.7) | | How long did it take to visualize, assess, and interpret the IRIS? 3D model with CT scan for the purpose of surgical planning | | <1 min | 4 (50.0) | 4 (26.7) | 1 (12.5) | 9 (29.0) | | 2-5 min | 3 (37.5) | 9 (60.0) | 7 (87.5) | 19 (61.3) | | >5 min | 1 (12.5) | 2 (13.3) | 0 (0) | 3 (9.7) | | Which artery branch will you select for clamping based on IRIS? 3D model with CT scan | | Primary renal artery | 5 (62.5) | 4 (26.7) | 2 (25.0) | 11 (35.5) | | Secondary branch | 1 (12.5) | 4 (26.7) | 5 (62.5) | 10 (32.3) | | Tertiary branch | 0 (0) | 3 (20.0) | 1 (25.0) | 4 (12.9) | | Not applicable | 2 (25.0) | 4 (26.7) | 0 (0) | 6 (19.4) | | You feel the extra time spent on IRIS? technology was valuable | | Yes | 7 (87.5) | 15 (100.0) | 8 (100.0) | 30 (96.8) |
|
|
Preoperative questionnaires given to surgeon.
|
| Aspect of surgery | Questionnaire result | Overlap, % | | Preoperative | Intraoperative | | Interpretation of anatomy, n (%) | 31 (100.0) | 31 (100.0) | 100.0 | | Tumor location | 30 (96.8) | 31 (100) | 96.8 | | Renal artery | 30 (96.8) | 31 (100) | 96.8 | | Renal vein | 31 (100) | 31 (100) | 100.0 | | Tumor depth | 30 (96.8) | 31 (100) | 96.8 | | Relationship to surrounding structures | 29 (93.5) | 30 (96.8) | 96.7 | | The part of the operation or clinical situation where you were satisfied with the information available in the IRIS? 3D model with CT scan, n (%) | | Identification of ureter and vessels | 22 (71.0) | 21 (67.7) | 95.5 | | Identification of tumor location | 29 (93.5) | 30 (96.8) | 96.7 | | Identification of tumor depth | 28 (90.3) | 30 (96.8) | 93.3 | | Tumor resection for complex tumor | 17 (54.8) | 17 (54.8) | 100.0 | | Aided in planning of off-clamping or segmental clamping | 14 (45.2) | 14 (45.2) | 100.0 | | Identification of feeding vessel to the tumor | 20 (64.5) | 19 (61.3) | 95.0 | | Clamping techniquea, n | | | | | Primary renal artery clamping | 11 | 13 | 84.6 | | Off-clamp and selective clamping | 20 | 18 | 90.0 | | No clamp | 6 | 8 | 75.0 | | Secondary artery clamping | 10 | 7 | 70.0 | | Tertiary artery clamping | 4 | 3 | 75.0 |
|
|
Preoperative predictive accuracy of IRIS? in comparison to intraoperative findings based on comparison of preoperative and intraoperative questionnaires.
|
| Intraoperative questionnaires given to surgeons evaluating imaging using both IRIS? and CT scan | R.E.N.A.L. nephrometry score | All patients for IRIS? (n=31) | | 4-6 (n=8) | 7-9 (n=15) | 10-12 (n=8) | | The IRIS? 3D model with CT scan visualization method made your procedure efficient | | Agree and strongly agree | 5 (62.5) | 14 (93.3) | 8 (100.0) | 27 (87.1) | | The IRIS? 3D model with CT scan visualization method allowed the identification of target anatomy for this procedure | | Agree and strongly agree | 7 (87.5) | 15 (100.0) | 8 (100.0) | 30 (96.8) | | Does use of IRIS? model lead to any alteration in intraoperative plan compared to preoperative plan | | No | 8 (100.0) | 15 (100.0) | 8 (100.0) | 31 (100.0) | | How easy is IRIS? technology to use intraoperatively | | Very easy | 4 (50.0) | 11 (73.3) | 7 (87.5) | 22 (71.0) | | Easy | 4 (50.0) | 4 (26.7) | 1 (12.5) | 9 (29.0) | | Neutral, difficult, very difficult | 0 (0.0) | 0 (0.0) | 0 (0) | 0 (0.0) | | How many times did you refer to the IRIS? model with CT scan during the procedure | | 1-2 times | 6 (75.0) | 4 (26.7) | 1 (12.5) | 11 (35.5) | | 3 times | 2 (25.0) | 8 (53.3) | 3 (37.5) | 13 (41.9) | | 4-10 times | 0 (0) | 3 (20.0) | 2 (25.0) | 5 (16.1) | | >10 times | 0 (0) | 0 (0) | 2 (25.0) | 2 (6.5) | | Did you use the IRIS? model on iOS device or TilePro | | iOS device only | 7 (87.5) | 10 (66.7) | 1 (12.5) | 18 (58.1) | | TilePro only | 0 (0) | 0 (0) | 1 (12.5) | 1 (3.2) | | Both iOS and TilePro | 1 (12.5) | 5 (33.3) | 6 (75.0) | 12 (38.7) | | Do you think that using IRIS? model during surgery caused disruption to the procedure | | Yes | 0 (0) | 0 (0) | 0 (0) | 0 (0) | | Which feature of IRIS? software was most valuable | | Pan and rotate | 5 (62.5) | 14 (93.3) | 8 (100.0) | 27 (87.1) | | Alternating component transparency | 4 (50.0) | 11 (73.3) | 7 (87.5) | 22 (71.0) | | Slice display | 2 (25.0) | 1 (6.7) | 0 (0) | 3 (9.7) | | Windowing | 3 (37.5) | 1 (6.7) | 1 (12.5) | 5 (16.1) | | Do you think that interaction of the IRIS? software with CT scan was very intuitive | | Agree and strongly agree | 7 (87.5) | 15 (100.0) | 8 (100.0) | 30 (96.8) | | The IRIS? 3D model with CT scans could simplify the clinical case discussion with the patient | | Agree and strongly agree | 6 (75.0) | 15 (100.0) | 8 (100.0) | 29 (93.5) | | Was IRIS? a useful tool for discussion of the case with your trainees intraoperatively | | Agree and strongly agree | 7 (87.5) | 15 (100.0) | 8 (100.0) | 30 (96.8) | | The visual quality of the IRIS? is sufficient to support you preoperatively and intraoperatively | | Agree and strongly agree | 8 (100.0) | 14 (93.3) | 8 (100.0) | 30 (96.8) |
|
|
Intraoperative questionnaires given to surgeons.
|
|
|
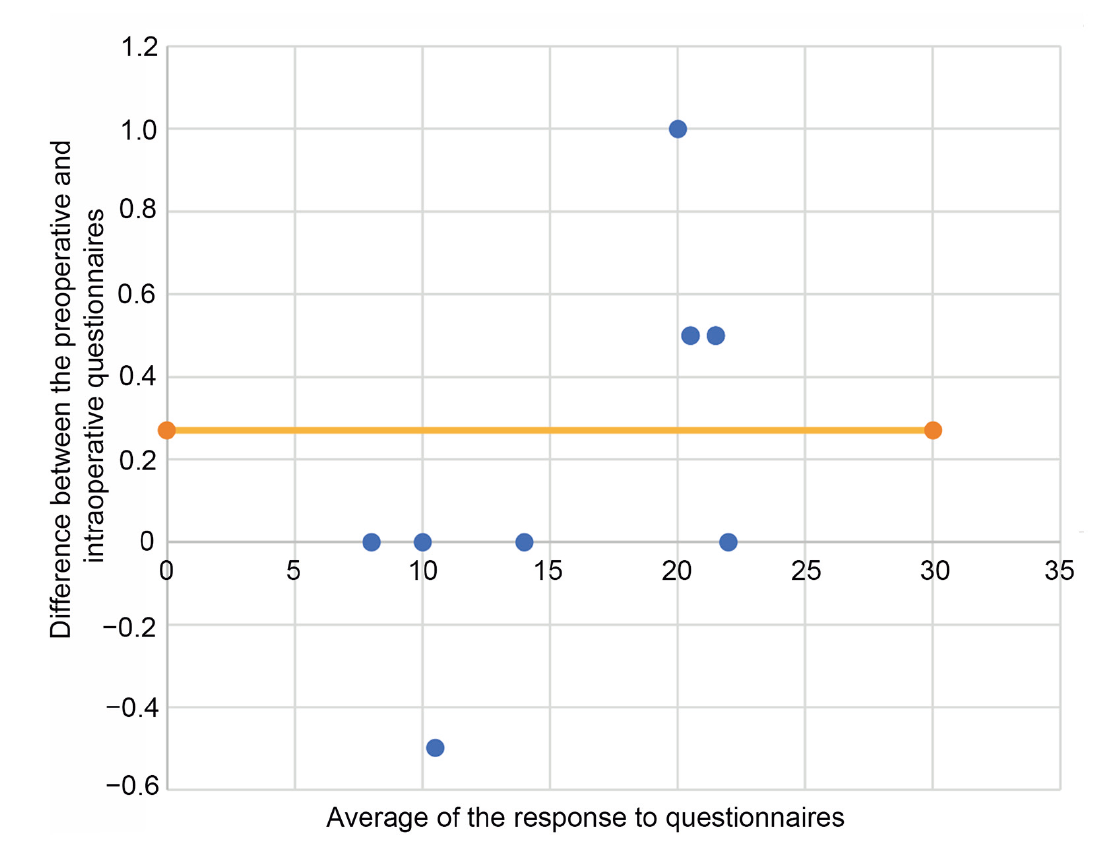
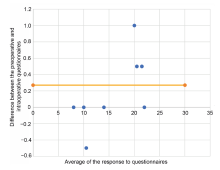
Bland-Altman plot evaluating the difference in intraoperative and preoperative assessment on IRIS?. Orange line indicates the mean difference in questionnaires. 95% of the values (blue dot) lie within 2 standard deviation of mean difference in questionnaires. The calculated 95% confidence interval of ?0.531-1.076 is suggestive of insignificant or no difference between preoperative and intraoperative response based on the questionnaires.
|
| [1] |
Tan HJ, Filson CP, Litwin MS. Contemporary, age-based trends in the incidence and management of patients with early-stage kidney cancer. Urol Oncol 2015; 33:21.e19-26. https://doi.org/10.1016/j.urolonc.2014.10.002.
doi: 10.1016/j.urolonc.2014.10.002
|
| [2] |
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin 2000; 70:7-30.
doi: 10.3322/caac.v70.1
|
| [3] |
Venkatramani V, Koru-Sengul T, Miao F, Nahar B, Prakash NS, Swain S, et al. A comparison of overall survival and perioperative outcomes between partial and radical nephrectomy for cT1b and cT 2 renal cell carcinomadanalysis of a national cancer registry. Urol Oncol 2018; 36:90.e9-14. https://doi.org/10.1016/j.urolonc.2017.11.008.
doi: 10.1016/j.urolonc.2017.11.008
pmid: 29254672
|
| [4] |
Mir MC, Derweesh I, Porpiglia F, Zargar H, Mottrie A, Autorino R. Partial nephrectomy versus radical nephrectomy for clinical T1b and T2 renal tumors: a systematic review and meta-analysis of comparative studies. Eur Urol 2017; 71:606-17.
doi: S0302-2838(16)30533-4
pmid: 27614693
|
| [5] |
Rogers C, Sukumar S, Gill IS. Robotic partial nephrectomy: the real benefit. Curr Opin Urol 2011; 21:60-4.
doi: 10.1097/MOU.0b013e3283402232
pmid: 20962648
|
| [6] |
Kutikov A, Uzzo RG, The RENAL. Nephrometry score: a comprehensive standardized system for quantitating renal tumor size, location, and depth. J Urol 2009; 182:844-53.
doi: 10.1016/j.juro.2009.05.035
|
| [7] |
Ficarra V, Novara G, Secco S, Macchi V, Porzionato A, De Caro R, et al. Preoperative aspects, and dimensions used for an anatomical (PADUA) classification of renal tumors in patients who are candidates for nephron-sparing surgery. Eur Urol 2009; 56:786-93.
doi: 10.1016/j.eururo.2009.07.040
|
| [8] |
Autorino R, Porpiglia F, Dasgupta P, Rassweiler J, Catto JW, Hampton LJ, et al. Precision surgery, and genitourinary cancers. Eur J Surg Oncol 2017; 43:893-908.
doi: S0748-7983(17)30350-5
pmid: 28254473
|
| [9] |
Lasser MS, Doscher M, Keehn A, Chernyak V, Garfein E, Ghavamian R. Virtual surgical planning: a novel aid to robotassisted laparoscopic partial nephrectomy. J Endourol 2012; 26:1372-9.
doi: 10.1089/end.2012.0093
|
| [10] |
Shirk JD, Kwan L, Saigal C. The use of 3-dimensional, virtual reality models for surgical planning of robotic partial nephrectomy. Urology 2019; 125:92-7.
doi: S0090-4295(18)31351-7
pmid: 30597166
|
| [11] |
Shirk JD, Thiel DD, Wallen EM, Linehan JM, White WM, Badani KK, et al. Effect of 3-dimensional virtual reality models for surgical planning of robotic-assisted partial nephrectomy on surgical outcomes: a randomized clinical trial. JAMA Netw Open 2019; 4:2-11.
|
| [12] |
Wake N, Nussbaum JE, Elias MI, Nikas CV, Bjurlin MA. 3D printing, augmented reality, and virtual reality for the assessment and management of kidney and prostate cancer: a systematic review. Urology 2020; 143:20-32.
doi: S0090-4295(20)30663-4
pmid: 32535076
|
| [13] |
Gurung PMS, Melnyk R, Holler T, Oppenhimer D, Witthaus M, Hani HH, et al. Application of IRIS three-dimensional anatomical models as preoperative surgical planning tools in the management of localized renal masses. J Endourol 2021; 35: 383-9.
doi: 10.1089/end.2020.0405
pmid: 33451273
|
| [14] |
Giavarina D. Understanding Bland Altman analysis. Biochem Med (Zagreb) 2015; 25:141-51.
doi: 10.11613/issn.1846-7482
|
| [15] |
Porpiglia F, Fiori C, Checcucci E, Amparore D, Bertolo R. Hyperaccuracy three-dimensional reconstruction is able to maximize the efficacy of selective clamping during robotassisted partial nephrectomy for complex renal masses. Eur Urol 2018; 74:651-60.
doi: 10.1016/j.eururo.2017.12.027
|
| [16] |
Checcucci F, Amparore D, Fiori C, Manfredi M, Ivano M, Di Dio M, et al. 3D imaging applications for robotic urologic surgery: an ESUT YAUWP review. World J Urol 2020; 38:869-81.
doi: 10.1007/s00345-019-02922-4
pmid: 31456017
|
| [17] |
Hung AJ, Shah SH, Dalag L, Shin D, Gill IS. Development and validation of a novel robotic procedure specific simulation platform: partial nephrectomy. J Urol 2015; 194:520-6.
doi: 10.1016/j.juro.2015.02.2949
pmid: 25801765
|
| [18] |
Kobayashi S, Cho B, Huaulmé A, Tatsugami K, Honda H, Jannin P, et al. Assessment of surgical skills by using surgical navigation in robot-assisted partial nephrectomy. Int J Comput Assist Radiol Surg 2019; 14:1449-59.
doi: 10.1007/s11548-019-01980-8
pmid: 31119486
|
| [19] |
Kobayashi S, Cho B, Mutaguchi J, Inokuchi J, Tatsugami K, Hashizume M, et al. Surgical navigation improves renal parenchyma volume preservation in robot-assisted partial nephrectomy: a propensity score matched comparative analysis. J Urol 2020; 204:149-56.
doi: 10.1097/JU.0000000000000709
pmid: 31859597
|
| [20] |
Ukimura O, Nakamoto M, Gill IS. Three-dimensional reconstruction of renovascular-tumor anatomy to facilitate zeroischemia partial nephrectomy. Eur Urol 2012; 61:211-7.
doi: 10.1016/j.eururo.2011.07.068
pmid: 21937162
|
| [21] |
Porpiglia F, Amparore D, Checcucci E, Maanfredi M, Stura I, Migliaretti G, et al. Three-dimensional virtual imaging of renal tumours: a new tool to improve the accuracy of nephrometry scores. BJU Int 2019; 124:945-54.
doi: 10.1111/bju.14894
pmid: 31390140
|
| [22] |
Hyde ER, Berger LU, Ramachandran N, Hughes-Hallett A, Pavithran NP, Tran MGB, et al. Interactive virtual 3D models of renal cancer patient anatomies alter partial nephrectomy surgical planning decisions and increase surgeon confidence compared to volume-rendered images. Int J Comput Assist Radiol Surg 2019; 14:723-32.
doi: 10.1007/s11548-019-01913-5
pmid: 30680601
|
| [23] |
Antonelli A, Veccia A, Palumbo C, Peroni A, Mirabella G, Cozzoli A, et al. Holographic reconstructions for preoperative planning before partial nephrectomy: a head-to-head comparison with standard CT scan. Urol Int 2019; 102:212-7.
doi: 10.1159/000495618
pmid: 30540991
|
| [24] |
Checcucci E, Amparore D, Pecoraro A, Peretti D, Aimar R, De Cillis S, et al. Mixed reality holograms for preoperative surgical planning of nephron-sparing surgery: evaluation of surgeons’ perception. Minerva Urol Nephrol 2021; 73:367-75.
doi: 10.23736/S2724-6051.19.03610-5
pmid: 31486325
|
| [1] |
Savio Domenico Pandolfo, Clara Cerrato, Zhenjie Wu, Antonio Franco, Francesco Del Giudice, Alessandro Sciarra, Paolo Verze, Giuseppe Lucarelli, Ciro Imbimbo, Sisto Perdonà, Edward E. Cherullo, Francesco Porpiglia, Ithaar H. Derweesh, Riccardo Autorino. A systematic review of robot-assisted partial nephrectomy outcomes for advanced indications: Large tumors (cT2-T3), solitary kidney, completely endophytic, hilar, recurrent, and multiple renal tumors[J]. Asian Journal of Urology, 2023, 10(4): 390-406. |
| [2] |
Enrico Checcucci, Alberto Piana, Gabriele Volpi, Pietro Piazzolla, Daniele Amparore, Sabrina De Cillis, Federico Piramide, Cecilia Gatti, Ilaria Stura, Enrico Bollito, Federica Massa, Michele Di Dio, Cristian Fiori, Francesco Porpiglia. Three-dimensional automatic artificial intelligence driven augmented-reality selective biopsy during nerve-sparing robot-assisted radical prostatectomy: A feasibility and accuracy study[J]. Asian Journal of Urology, 2023, 10(4): 407-415. |
| [3] |
Brianna Ruch, Deki Tsering, Chandra Bhati, Dhiren Kumar, Muhammad Saeed, Seung Duk Lee, Aamir Khan, Daisuke Imai, David Bruno, Marlon Levy, Adrian Cotterell, Amit Sharma. Right versus left fully robotic live donor nephrectomy and open kidney transplantation: Does the laterality of the donor kidney really matter?[J]. Asian Journal of Urology, 2023, 10(4): 453-460. |
| [4] |
Silu Chen, Shubo Fan, Hua Guan, Kunlin Yang, Zhihua Li, Shengwei Xiong, Xiang Wang, Zhenyu Li, Cheng Shen, Liqun Zhou, Xuesong Li. The application of internal suspension technique in retroperitoneal robot-assisted laparoscopic partial nephrectomy with a new robotic system KangDuo Surgical Robot-01: Initial experience[J]. Asian Journal of Urology, 2023, 10(4): 482-487. |
| [5] |
Federico Piramide, Carlo Andrea Bravi, Marco Paciotti, Luca Sarchi, Luigi Nocera, Adele Piro, Maria Peraire Lores, Eleonora Balestrazzi, Angelo Mottaran, Rui Farinha, Hubert Nicolas, Pieter De Backer, Frederiek D'hondt, Peter Schatteman, Ruben De Groote, Geert De Naeyer, Alexandre Mottrie. Robot-assisted adrenalectomy: Step-by-step technique and surgical outcomes at a high-volume robotic center[J]. Asian Journal of Urology, 2023, 10(4): 475-481. |
| [6] |
Thomas Whish-Wilson, Jo-Lynn Tan, William Cross, Lih-Ming Wong, Tom Sutherland. Prostate magnetic resonance imaging and the value of experience: An intrareader variability study[J]. Asian Journal of Urology, 2023, 10(4): 488-493. |
| [7] |
Thitipat Hansomwong, Pat Saksirisampant, Sudhir Isharwal, Pubordee Aussavavirojekul, Varat Woranisarakul, Siros Jitpraphai, Sunai Leewansangtong, Tawatchai Taweemonkongsap, Sittiporn Srinualnad. Role of preoperative magnetic resonance imaging on the surgical outcomes of radical prostatectomy: Does preoperative tumor recognition reduce the positive surgical margin in a specific location? Experience from a Thailand prostate cancer specialized center[J]. Asian Journal of Urology, 2023, 10(4): 494-501. |
| [8] |
Donghua Xie,Di Gu,Ming Lei,Cong Cai,Wen Zhong,Defeng Qi,Wenqi Wu,Guohua Zeng,Yongda Liu. The application of indocyanine green in guiding prostate cancer treatment[J]. Asian Journal of Urology, 2023, 10(1): 1-8. |
| [9] |
Kumawat Ghanshyam,Vyas Nachiket,Sharma Govind,Priyadarshi Shivam,Gupta Bhagwan Sahay,Singla Mohit,Kumar Ashok. Validation of Vesical Imaging Reporting and Data System score for the diagnosis of muscle-invasive bladder cancer: A prospective cross-sectional study[J]. Asian Journal of Urology, 2022, 9(4): 467-472. |
| [10] |
Karl-Friedrich Kowalewski,Luisa Egen,Chanel E. Fischetti,Stefano Puliatti,Gomez Rivas Juan,Mark Taratkin,Rivero Belenchon Ines,Marie Angela Sidoti Abate,Julia Mühlbauer,Frederik Wessels,Enrico Checcucci,Giovanni Cacciamani,on behalf of the Young Academic Urologists (YAU)-Urotechnology-Group . Artificial intelligence for renal cancer: From imaging to histology and beyond[J]. Asian Journal of Urology, 2022, 9(3): 243-252. |
| [11] |
Alberto Piana,Iulia Andras,Pietro Diana,Paolo Verri,Andrea Gallioli,Riccardo Campi,Thomas Prudhomme,Vital Hevia,Romain Boissier,Alberto Breda,Angelo Territo,on behalf of European Association of Urology (EAU) Young Academic Urologists (YAU) Kidney Transplantation Working Group, Arnhem, Netherlands . Small renal masses in kidney transplantation: Overview of clinical impact and management in donors and recipients[J]. Asian Journal of Urology, 2022, 9(3): 208-214. |
| [12] |
Umberto Carbonara,Daniele Amparore,Cosimo Gentile,Riccardo Bertolo,Selcuk Erdem,Alexandre Ingels,Michele Marchioni,Constantijn H.J. Muselaers,Onder Kara,Laura Marandino,Nicola Pavan,Eduard Roussel,Angela Pecoraro,Fabio Crocerossa,Giuseppe Torre,Riccardo Campi,Pasquale Ditonno. Current strategies to diagnose and manage positive surgical margins and local recurrence after partial nephrectomy[J]. Asian Journal of Urology, 2022, 9(3): 227-242. |
| [13] |
Stefano Puliatti,Ahmed Eissa,Enrico Checcucci,Pietro Piazza,Marco Amato,Stefania Ferretti,Simone Scarcella,Juan Gomez Rivas,Mark Taratkin,Josè Marenco,Ines Belenchon Rivero,Karl-Friedrich Kowalewski,Giovanni Cacciamani,Ahmed El-Sherbiny,Ahmed Zoeir,Abdelhamid M. El-Bahnasy,Ruben De Groote,Alexandre Mottrie,Salvatore Micali. New imaging technologies for robotic kidney cancer surgery[J]. Asian Journal of Urology, 2022, 9(3): 253-262. |
| [14] |
Luke P. O’Connor,Shayann Ramedani,Michael Daneshvar,Arvin K. George,Andre Luis Abreu,Giovanni E. Cacciamani,Amir H. Lebastchi. Future perspective of focal therapy for localized prostate cancer[J]. Asian Journal of Urology, 2021, 8(4): 354-361. |
| [15] |
Yucong Zhang,Gongwei Long,Haojie Shang,Beichen Ding,Guoliang Sun,Wei Ouyang,Man Liu,Yuan Chen,Heng Li,Hua Xu,Zhangqun Ye. Comparison of the oncological, perioperative and functional outcomes of partial nephrectomy versus radical nephrectomy for clinical T1b renal cell carcinoma: A systematic review and meta-analysis of retrospective studies[J]. Asian Journal of Urology, 2021, 8(1): 117-125. |
|
|
|
|