|
|
|
| Three-dimensional imaging reconstruction of the kidney's anatomy for a tailored minimally invasive partial nephrectomy: A pilot study |
Daniele Amparorea,b,*( ),Angela Pecoraroa,b,Federico Piramidea,Paolo Verria,Enrico Checcuccia,c,Sabrina De Cillisa,Alberto Pianaa,Mariano Burgioa,Michele Di Diod,Matteo Manfredia,Cristian Fioria,Francesco Porpigliaa ),Angela Pecoraroa,b,Federico Piramidea,Paolo Verria,Enrico Checcuccia,c,Sabrina De Cillisa,Alberto Pianaa,Mariano Burgioa,Michele Di Diod,Matteo Manfredia,Cristian Fioria,Francesco Porpigliaa
|
aDepartment of Urology, San Luigi Gonzaga Hospital, University of Turin, Orbassano, Turin, Italy
bEuropean Association of Urology (EAU) Young Academic Urologists (YAU) Renal Cancer Working Group, Arnhem, Netherlands
cEuropean Association of Urology (EAU) Young Academic Urologists (YAU) Uro-technology and SoMe Working Group, Arnhem, Netherlands
dDivision of Urology, Department of Surgery, SS Annunziata Hospital, Cosenza, Italy |
|
|
|
|
Abstract Objective: The aim of the study was to evaluate three-dimensional virtual models (3DVMs) usefulness in the intraoperative assistance of minimally-invasive partial nephrectomy in highly complex renal tumors.
Methods: At our institution cT1-2N0M0 all renal masses with Preoperative Aspects and Dimensions Used for an Anatomical classification score ≥10 treated with minimally-invasive partial nephrectomy were considered for the present study. For inclusion a baseline contrast-enhanced computed tomography in order to obtain 3DVMs, the baseline and postoperative serum creatinine as well as estimated glomerular filtration rate values were needed. These patients, in which 3DVMs were used to assist the surgeon in the planning and intraoperative guidance, were then compared with a control group of patients who underwent minimally-invasive partial nephrectomy with the same renal function assessments, but without 3DVMs. Multivariable logistic regression models were used to predict the margin, ischemia, and complication score achievement.
Results: Overall, 79 patients met the inclusion criteria and were compared with 143 complex renal masses without 3DVM assistance. The 3DVM group showed better postoperative outcomes in terms of baseline-weighted differential estimated glomerular filtration rate (-17.7% vs. -22.2%, p=0.03), postoperative complications (16.5% vs. 23.1%, p=0.03), and major complications (Clavien Dindo >III, 2.5% vs. 5.6%, p=0.03). At multivariable logistic regression 3DVM assistance independently predicted higher rates of successful partial nephrectomy (odds ratio: 1.42, p=0.03).
Conclusion: 3DVMs represent a useful tool to plan a tailored surgical approach in case of surgically complex masses. They can be used in different ways, matching the surgeon's needs from the planning phase to the demolitive and reconstructive phase, leading towards maximum safety and efficacy outcomes.
|
|
Available online: 20 July 2022
|
|
Corresponding Authors:
Daniele Amparore
E-mail: danieleamparore@hotmail.it
|
|
|
|
|
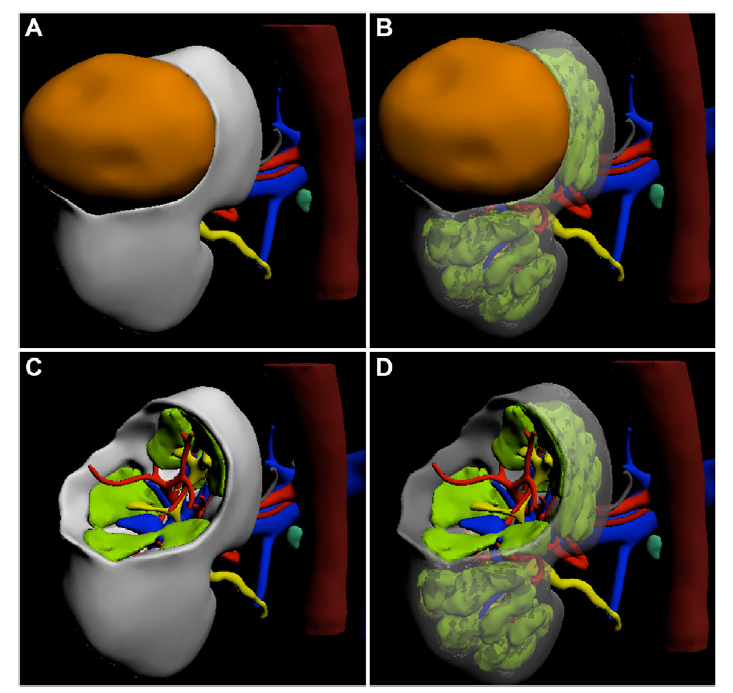
Three-dimensional virtual model of a complex left renal mass. (A) Virtual image of the tumor and renal parenchyma; (B) Virtual image of the tumor hiding the renal cortex; (C) Virtual image of the renal parenchyma focused on the tumor bed; (D) Virtual image of the tumor bed hiding the cortical portion of the kidney. The direct interaction with the virtual tool allows the surgeon to focus the attention on some structures of the kidney increasing his/her knowledge on the specific case anatomy.
|
|
|
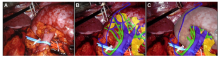
Example of augmented reality technology during left robot-assisted partial nephrectomy. (A) Left kidney after its complete isolation from perirenal fat and vascular pedicle dissection; (B) Overlapping of virtual images over the real kidney enhancing the vascular structures and the collecting system; (C) Overlapping of virtual images focusing on the renal parenchyma. The intraoperative target was identified in order to overlap on the 3D virtual model comprehensive of all its components, which could be visualized separately on the basis of the surgeon's preference.
|

| Variable | Overall, n=222 | Without 3DVM, n=143, 64.4% | With 3DVM, n=79, 35.6% | p-Value | | Agea, year | 61 (51-72) | 61 (52-72) | 60 (51-72) | 0.71 | | BMIa, kg/m2 | 25.7 (24.3-26.0) | 25.7 (24.8-26.0) | 25.5 (22.9-26.2) | 0.06 | | PADUA scorea | 11 (10-11) | 11 (10-11) | 11 (10-12) | 0.40 | | CCIa | 1 (0-2) | 0 (0-1) | 1 (0-2) | 0.08 | | Clinical tumor sizea, mm | 47.0 (36.0-60.0) | 45.0 (30.5-59.0) | 50.0 (43.5-60.0) | 0.01 | | R.E.N.A.L. nephrometry scorea | 9 (8-10) | 9 (8-10) | 9 (8-10) | 0.98 | | ASA scoreb | | | | 0.12 | | 0 | 2 (0.9) | 0 (0) | 2 (2.5) | | 1 | 51 (23.0) | 28 (19.6) | 23 (29.1) | | 2 | 129 (58.1) | 90 (62.9) | 39 (49.4) | | 3 | 40 (18.0) | 25 (17.5) | 15 (19.0) | | cTb | | | | | | cT1a | 75 (33.8) | 62 (43.4) | 13 (16.5) | | | cT1b | 118 (53.2) | 62 (43.4) | 56 (70.9) | 0.0003 | | cT2a | 24 (10.8) | 16 (11.2) | 8 (10.1) | | | cT2b | 2 (0.9) | 2 (1.4) | 0 (0.0) | | | cT3a | 3 (1.4) | 1 (0.7) | 2 (2.5) | |
|
|
Preoperative characteristics of 222 patients with high complexity renal masses treated with minimally-invasive partial nephrectomy with (n=79) or without (n=143) the perioperative assistance of 3DVM.
|
| Variable | Overall, n=222 | Without 3DVM, n=143, 64.4% | With 3DVM, n=79, 35.6% | p-Value | | Type of techniquea | | | | 0.06 | | Laparoscopic | 117 (52.7) | 70 (49.0) | 47 (59.5) | | Robot-assisted | 105 (47.3) | 73 (51.0) | 32 (40.5) | | Hilar clampinga | | | | 0.03 | | Clampless | 67 (30.2) | 43 (30.1) | 24 (30.4) | | Global ischemia | 71 (32.0) | 49 (34.3) | 22 (27.8) | | Selective ischemia | 84 (37.8) | 51 (35.7) | 33 (41.8) | | Ischemia timeb, min | 15.1 (6.0-23.0) | 16.0 (9.5-24.0) | 15.0 (10.0-20.5) | 0.79 | | Blood lossb, mL | 100 (50-200) | 100 (50-200) | 100 (50-200) | 0.36 | | Operative timeb, min | 97 (75-130) | 105 (77-130) | 90 (70-120) | 0.23 | | Tumor locationa | | | | 0.56 | | Middle | 141 (63.5) | 88 (61.5) | 53 (67.1) | | Upper/inferior | 81 (36.5) | 55 (38.5) | 26 (32.9) | | Tumor growth patterna | | | | 0.68 | | <50% | 116 (52.3) | 76 (53.1) | 40 (50.6) | | ≥50% | 32 (14.4) | 22 (15.4) | 10 (12.7) | | Entirely endophytic | 74 (33.3) | 45 (31.5) | 29 (36.7) | | Kidney face locationa | | | | <0.001 | | Anterior | 97 (43.7) | 56 (39.2) | 41 (51.9) | | Cross or coronal | 60 (27.0) | 49 (34.3) | 11 (13.9) | | Posterior | 65 (29.3) | 38 (26.6) | 27 (34.2) | | Kidney rim locationa | | | | 0.40 | | Lateral | 57 (25.7) | 36 (25.2) | 21 (26.6) | | Medial | 165 (74.3) | 107 (74.8) | 58 (73.4) | | Sidea | | | | 0.45 | | Right | 110 (49.5) | 74 (51.7) | 36 (45.6) | | Left | 112 (50.5) | 69 (48.3) | 43 (54.4) | | Type of accessa | | | | 0.87 | | Retroperitoneal | 124 (55.9) | 79 (55.2) | 45 (57.0) | | Transperitoneal | 98 (44.1) | 64 (44.8) | 34 (43.0) | | Pathological sizeb, mm | 35.0 (25.0-45.5) | 35.0 (25.0-45.0) | 35.0 (25.0-50.0) | 0.30 | | Length of stayb, day | 6 (5-7) | 6 (5-8) | 6 (5-7) | 0.86 | | Opening collecting systema | 27 (12.2) | 21 (14.7) | 6 (7.6) | 0.21 | | Intraoperative complicationa | 6 (2.7) | 4 (2.8) | 2 (2.5) | 0.70 | | Postoperative complicationa | 46 (20.7) | 33 (23.1) | 13 (16.5) | 0.03 | | Clavien Dindoa | | | | | | 0 | 101 (45.5) | 65 (45.5) | 36 (45.6) | | I | 71 (32.0) | 43 (30.1) | 28 (35.4) | | II | 25 (11.3) | 17 (11.9) | 8 (10.1) | | III | 15 (6.8) | 10 (7.0) | 5 (6.3) | | >III | 10 (4.5) | 8 (5.6) | 2 (2.5) | 0.03 | | Benign histologya,c | | | | 0.62 | | Overall | 41 (18.5) | 28 (19.6) | 13 (16.5) | | Angiomyolipoma | 20 (9.0) | 12 (8.4) | 8 (10.1) | | Oncocytoma | 15 (6.8) | 12 (8.4) | 3 (3.8) | | Other benign | 6 (2.7) | 4 (2.8) | 2 (2.5) | | Malignant histologya,c | | | | 0.43 | | Overall | 181 (81.5) | 113 (79.0) | 68 (87.1) | | Clear cell | 120 (54.1) | 79 (55.2) | 41 (51.9) | | Papillary | 37 (16.7) | 18 (12.6) | 19 (24.1) | | Chromophobe | 20 (9.0) | 13 (9.1) | 7 (8.9) | | NOS, RCC | 4 (1.8) | 3 (2.1) | 1 (1.2) | | Tumor gradea,c | | | | 0.36 | | 1 | 73 (32.9) | 41 (28.7) | 32 (40.5) | | 2 | 93 (41.9) | 60 (42.0) | 33 (41.8) | | 3 | 12 (5.4) | 11 (7.7) | 1 (1.3) | | 4 | 3 (1.4) | 1 (0.7) | 2 (2.5) | | Presence of necrosisa | 96 (43.2) | 63 (44.1) | 33 (41.8) | 0.70 | | Achievement of MICa | 131 (59.0) | 79 (55.2) | 52 (65.8) | 0.01 | | Positive surgical marginsa | 6 (2.7) | 4 (2.8) | 2 (2.5) | 0.89 |
|
|
Perioperative and pathological characteristics of 222 patients with renal masses treated with minimally-invasive partial nephrectomy with or without the perioperative assistance of 3DVM.
|
| Variable | Overall, n=222 | With 3DVM, n=143, 64.4% | Without 3DVM, n=79, 35.6% | p-Value | | Baseline SCra, mg/dL | 1.0 (0.8-1.1) | 1.0 (0.8-1.1) | 0.9 (0.8-1.1) | 0.40 | | Postoperative SCra, mg/dL | 1.1 (0.9-1.3) | 1.1 (0.9-1.3) | 1.0 (0.8-1.3) | 0.10 | | b-WD SCra, % | 9.2 (-0.9-25.3) | 8.8 (1.1-29.3) | 9.3 (-0.9-20.4) | 0.30 | | Baseline eGFRa, mL/min/1.73 m2 | 64.9 (54.4-79.1) | 63.1 (54.2-75.2) | 68.6 (55.7-92.7) | 0.30 | | Postoperative eGFRa, mL/min/1.73 m2 | 75.2 (58.7-94.6) | 73.1 (58.4-92.8) | 83.1 (62.7-100.0) | 0.10 | | b-WD eGFRa, % | -21.0 (-32.7--1.8) | -22.2 (-33.0--1.3) | -17.7 (-30.6--2.6) | 0.03 |
|
|
Functional outcomes of 222 patients harboring renal masses treated with minimally-invasive partial nephrectomy with (n=79) or without (n=143) the perioperative assistance of 3DVM.
|
| Variable | Odds ratio | Confidence interval | p-Value | | Empty Cell | 2.5% | 97.5% | Empty Cell | | Age, year | 0.81 | 0.96 | 1.01 | 0.03 | | CCI<2 | Reference (1.00) | | | | | CCI>2 | 1.3809 | 0.44 | 4.80 | 0.58 | | Preoperative eGFR, mL/min/1.73 m2 | 1.00 | 0.97 | 1.01 | 0.59 | | No 3DVM available | Reference (1.00) | | | | | 3DVM available | 1.42 | 0.69 | 2.97 | 0.03 |
|
|
Multivariate logistic regression model in 163 patients with renal masses treated with minimally-invasive partial nephrectomy with or without the perioperative assistance of 3DVMs, predicting the achievement of MIC defined as ischemia time <20 min, negative margins, and no significant complications (Clavien Dindo<3)a.
|
| [1] |
Buffi NM, Saita A, Lughezzani G, Porter J, Dell’Oglio P, Amparore D, et al. Robot-assisted partial nephrectomy for complex (PADUA Score _10) tumors: techniques and results from a multicenter experience at four high-volume centers. Eur Urol 2020; 77:95e100.
doi: 10.1016/j.eururo.2019.03.006
|
| [2] |
Moglia A, Georgiou K, Georgiou E, Satava RM, Cuschieri A. A systematic review on artificial intelligence in robot-assisted surgery. Int J Surg 2021; 95:106151. https://doi.org/10.1016/j.ijsu.2021.106151.
doi: 10.1016/j.ijsu.2021.106151
|
| [3] |
Checcucci E, Autorino R, Cacciamani GE, Amparore D, De Cillis S, Piana A, et al. Uro-technology and SoMe working group of the young academic urologists working party of the European association of urology. Artificial intelligence and neural networks in urology: current clinical applications. Minerva Urol Nefrol 2020; 72:49e57.
doi: 10.23736/S0393-2249.19.03613-0
pmid: 31833725
|
| [4] |
Autorino R, Porpiglia F, Dasgupta P, Rassweiler J, Catto JW, Hampton LJ, et al. Precision surgery and genitourinary cancers. Eur J Surg Oncol 2017; 43:893e908.
doi: S0748-7983(17)30350-5
pmid: 28254473
|
| [5] |
Checcucci E, Amparore D, De Luca S, Autorino R, Fiori C, Porpiglia F. Precision prostate cancer surgery: an overview of new technologies and techniques. Minerva Urol Nefrol 2019; 71:487e501.
doi: 10.23736/S0393-2249.19.03365-4
pmid: 30700084
|
| [6] |
Hyde ER, Berger LU, Ramachandran N, Hughes-Hallett A, Pavithran NP, Tran MGB, et al. Interactive virtual 3D models of renal cancer patient anatomies alter partial nephrectomy surgical planning decisions and increase surgeon confidence compared to volume-rendered images. Int J Comput Assist Radiol Surg 2019; 14:723e32.
doi: 10.1007/s11548-019-01913-5
pmid: 30680601
|
| [7] |
Antonelli A, Veccia A, Palumbo C, Peroni A, Mirabella G, Cozzoli A, et al. Holographic reconstructions for preoperative planning before partial nephrectomy: a head-to-head comparison with standard CT scan. Urol Int 2019; 102:212e7.
doi: 10.1159/000495618
|
| [8] |
Bertolo R, Autorino R, Fiori C, Amparore D, Checcucci E, Mottrie A, et al. Expanding the indications of robotic partial nephrectomy for highly complex renal tumors: urologists’ perception of the impact of hyperaccuracy three-dimensional reconstruction. J Laparoendosc Adv Surg Tech 2019; 29:233e9.
doi: 10.1089/lap.2018.0486
|
| [9] |
Checcucci E, Amparore D, Pecoraro A, Peretti D, Aimar R, Cillis SDE, et al. 3D mixed reality holograms for preoperative surgical planning of nephron-sparing surgery: evaluation of surgeons’ perception. Minerva Urol Nephrol 2021; 73:367e75.
doi: 10.23736/S2724-6051.19.03610-5
pmid: 31486325
|
| [10] |
Wake N, Rosenkrantz AB, Huang WC, Wysock JS, Taneja SS, Sodickson DK, et al. A workflow to generate patient-specific three-dimensional augmented reality models from medical imaging data and example applications in urologic oncology. 3D Print Med 2021; 7:34. https://doi.org/10.1186/s41205-021-00125-5.
doi: 10.1186/s41205-021-00125-5
|
| [11] |
Wellens LM, Meulstee J, van de Ven CP, Littooij AS, van den Heuvel-Eibrink MM, et al. Comparison of 3-dimensional and augmented reality kidney models with conventional imaging data in the preoperative assessment of childrenwith Wilms tumors. JAMA NetwOpen 2019; 2:e192633. https://doi.org/10.1001/jamanetworkopen.2019.2633.
|
| [12] |
Porpiglia F, Amparore D, Checcucci E, Manfredi M, Stura I, Migliaretti G, et al. Three-dimensional virtual imaging of renal tumours: a new tool to improve the accuracy of nephrometry scores. BJU Int 2019; 124:945e54.
doi: 10.1111/bju.14894
|
| [13] |
Sutherland J, Belec J, Sheikh A, Chepelev L, Althobaity W, Chow BJW, et al. Applying modern virtual and augmented reality technologies to medical images and models. J Digit Imag 2019; 32:38e53.
doi: 10.1007/s10278-018-0122-7
|
| [14] |
Hekman MCH, Rijpkema M, Langenhuijsen JF, Boerman OC, Oosterwijk E, Mulders PFA. Intraoperative imaging techniques to support complete tumor resection in partial nephrectomy. Eur Urol Focus 2018; 4:960e8.
|
| [15] |
Makary J, van Diepen DC, Arianayagam R, McClintock G, Fallot J, Leslie S, et al. The evolution of image guidance in robotic-assisted laparoscopic prostatectomy (RALP): a glimpse into the future. J Robot Surg 2021. https://doi.org/10.1007/s11701-021-01305-5.
|
| [16] |
Porpiglia F, Checcucci E, Amparore D, Piramide F, Volpi G, Granato S, et al. Three-dimensional augmented reality robotassisted partial nephrectomy in case of complex tumours (PADUA _10):a new intraoperative tool overcoming the ultrasound guidance. Eur Urol 2020; 78:229e38.
doi: 10.1016/j.eururo.2019.11.024
|
| [17] |
Amparore D, Pecoraro A, Checcucci E, De Cillis S, Piramide F, Volpi G, et al. 3D imaging technologies in minimally-invasive kidney and prostate cancer surgery: which is the urologists’ perception? Minerva Urol Nephrol 2022; 74:178e85.
|
| [18] |
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chron Dis 1987; 40:373e83.
doi: 10.1016/0021-9681(87)90171-8
|
| [19] |
Ament R. Origin of the ASA classification. Anesthesiology 1979; 51:179. https://doi.org/10.1097/00000542-197908000-00023.
pmid: 453623
|
| [20] |
Ficarra V, Novara G, Secco S, Macchi V, Porzionato A, De Caro R, et al. Preoperative aspects and dimensions used for an anatomical (PADUA) classification of renal tumours in patients who are candidates for nephron-sparing surgery. Eur Urol 2009; 56:786e93.
doi: 10.1016/j.eururo.2009.07.040
|
| [21] |
Kutikov A, Uzzo RG. The R.E.N.A.L. nephrometry score: a comprehensive standardized system for quantitating renal tumor size, location and depth. J Urol 2009:844e53.
|
| [22] |
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004; 240:205e10.
doi: 10.1097/01.sla.0000133083.54934.ae
|
| [23] |
Buffi N, Lista G, Larcher A, Lughezzani G, Ficarra V, Cestari A, et al. Margin, ischemia, and complications (MIC) score in partial nephrectomy: a new system for evaluating achievement of optimal outcomes in nephron-sparing surgery. Eur Urol 2012; 62:617e8.
doi: 10.1016/j.eururo.2012.06.001
|
| [24] |
Amparore D, Pecoraro A, Piramide F, Checcucci E, De Cillis S, Volpi G, et al. Comparison between minimally-invasive partial and radical nephrectomy for the treatment of clinical T2 renal masses: results of a 10-year study in a tertiary care center. Minerva Urol Nephrol 2021; 73:509e17.
doi: 10.23736/S2724-6051.21.04390-1
pmid: 33887896
|
| [25] |
Daza J, Okhawere KE, Ige O, Elbakry A, Sfakianos JP, Abaza R, et al. The role of RENAL score in predicting complications after robotic partial nephrectomy. Minerva Urol Nefrol 2022; 74:57e62.
|
| [26] |
Beksac AT, Okhawere KE, Elbakry AA, Dayal BD, Paulucci DJ, Rothberg MB, et al. Management of high complexity renal masses in partial nephrectomy: a multicenter analysis. Urol Oncol 2019; 37:437e44.
doi: S1078-1439(19)30152-8
pmid: 31103334
|
| [27] |
Lin P, Wu M, Gu H, Tu Lanzhen, Liu Shilan, Yu Zhiling, et al. Comparison of outcomes between laparoscopic and robot-assisted partial nephrectomy for complex renal tumors:RENAL score _7 or maximum tumor size >4cm. Minerva Urol Nephrol 2021; 73:154e64.
|
| [28] |
Checcucci E, Amparore D, Fiori C, Manfredi M, Ivano M, Di Dio M, et al. 3D imaging applications for robotic urologic surgery: an ESUT YAUWP review. World J Urol 2020; 38:869e81.
doi: 10.1007/s00345-019-02922-4
pmid: 31456017
|
| [29] |
Bianchi L, Schiavina R, Bortolani B, Cercenelli L, Gaudiano C, Carpani G, et al. Interpreting nephrometry scores with three-dimensional virtual modelling for better planning of robotic partial nephrectomy and predicting complications. Urol Oncol 2021; 39:e1e9. https://doi.org/10.1016/j.urolonc.2021.07.024.
|
| [30] |
Porpiglia F, Fiori C, Checcucci E, Amparore D, Bertolo R. Hyperaccuracy three-dimensional reconstruction is able to maximize the efficacy of selective clamping during robot-assisted partial nephrectomy for complex renal masses. Eur Urol 2018; 74: 651e60.
doi: 10.1016/j.eururo.2017.12.027
|
| [31] |
Amparore D, Pecoraro A, Checcucci E, Piramide F, Verri P, De Cillis S, et al. Three-dimensional virtual models’ assistance during minimally invasive partial nephrectomy minimizes the impairment of kidney function. Eur Urol Oncol 2022; 5:104e8.
|
| [32] |
Zhang C, Guo F, Jing T, Wang F, Wang H, Ye C, et al. The margin strategy in laparoscopic partial nephrectomy with selective renal artery clamping: anatomical basis, surgical technique and comparative outcomes. Asian J Surg 2020; 43:417e22.
doi: S1015-9584(18)30637-7
pmid: 31253384
|
| [33] |
Cacciamani GE, Medina LG, Gill TS, Mendelsohn A, Husain F, Bhardwaj L, et al. Impact of renal hilar control on outcomes of robotic partial nephrectomy: systematic review and cumulative meta-analysis. Eur Urol Focus 2019; 5:619e35.
doi: S2405-4569(18)30013-0
pmid: 29422419
|
| [34] |
Brassetti A, Anceschi U, Bertolo R, Ferriero M, Tuderti G, Capitanio U, et al. Surgical quality, cancer control and functional preservation: introducing a novel trifecta for robot-assisted partial nephrectomy. Minerva Urol Nefrol 2020; 72:82e90.
doi: 10.23736/S0393-2249.19.03570-7
pmid: 31833720
|
| [35] |
Antonelli A, Mari A, Longo N, Novara G, Porpiglia F, Schiavina R, et al. Role of clinical and surgical factors for the prediction of immediate, early and late functional results, and its relationship with cardiovascular outcome after partial nephrectomy: results from the prospective multicenter RECORd 1 project. J Urol 2018; 199:927e32.
doi: 10.1016/j.juro.2017.11.065
|
| [36] |
Introini C, Di Domenico A, Ennas M, Campodonico F, Brusasco C, Benelli A. Functional and oncological outcomes of 3D clampless sutureless laparoscopic partial nephrectomy for renal tumors with lownephrometry score. MinervaUrol Nefrol 2020; 72:723e8.
|
| [37] |
Mitsui Y, Sadahira T, Araki M, Maruyama Y, Nishimura S, Wada K, et al. The 3-D volumetric measurement including resected specimen for predicting renal function after robot-assisted partial nephrectomy. Urology 2019; 125:104e10.
doi: 10.1016/j.urology.2018.12.020
|
| [38] |
Klingler MJ, Babitz SK, Kutikov A, Campi R, Hatzichristodoulou G, Sanguedolce F, et al. Assessment of volume preservation performed before or after partial nephrectomy accurately predicts postoperative renal function: results from a prospective multicenter study. Urol Oncol 2019; 37:33e9.
doi: S1078-1439(18)30453-8
pmid: 30473205
|
| [39] |
Ficarra V, Caloggero S, Rossanese M, Giannarini G, Crestani A, Ascenti G, et al. Computed tomography features predicting aggressiveness of malignant parenchymal renal tumors suitable for partial nephrectomy. Minerva Urol Nephrol 2021; 73:17e31.
|
| [40] |
Zhang H, Yin F, Yang L, Qi A, Cui W, Yang S, et al. Computed tomography image under three-dimensional reconstruction algorithm based in diagnosis of renal tumors and retroperitoneal laparoscopic partial nephrectomy. J Healthc Eng 2021; 2021:3066930. https://doi.org/10.1155/2021/3066930.eCollection2021.
|
| [41] |
Grosso AA, Di Maida F, Tellini R, Mari A, Sforza S, Masieri L, et al. Robot-assisted partial nephrectomy with 3D preoperative surgical planning: video presentation of the Florentine experience. Int Braz J Urol 2021; 47:1272e3.
doi: 10.1590/s1677-5538.ibju.2020.1075
|
| [42] |
Michiels C, Khene ZE, Prudhomme T, de Hauteclocque AB, Cornelis FH, Percot M, et al. 3D-Image guided robotic-assisted partial nephrectomy: a multi-institutional propensity score-matched analysis (UroCCR study 51). World J Urol 2021. https://doi.org/10.1007/s00345-021-03645-1.
|
| [1] |
Karl-Friedrich Kowalewski,Luisa Egen,Chanel E. Fischetti,Stefano Puliatti,Gomez Rivas Juan,Mark Taratkin,Rivero Belenchon Ines,Marie Angela Sidoti Abate,Julia Mühlbauer,Frederik Wessels,Enrico Checcucci,Giovanni Cacciamani,on behalf of the Young Academic Urologists (YAU)-Urotechnology-Group . Artificial intelligence for renal cancer: From imaging to histology and beyond[J]. Asian Journal of Urology, 2022, 9(3): 243-252. |
| [2] |
Michele Marchioni,Daniele Amparore,Igino Andrea Magli,Riccardo Bertolo,Umberto Carbonara,Selcuk Erdem,Alexandre Ingels,Constantijn H.J. Muselaers,Onder Kara,Marco Mascitti,Tobias Klatte,Maximilian Kriegmair,Nicola Pavan,Eduard Roussel,Angela Pecoraro,Laura Marandino,Riccardo Campi,Luigi Schips,on behalf of the European Association of Urology (EAU) Young Academic Urologists (YAU) Renal Cancer group . Potential benefit of lymph node dissection during radical nephrectomy for kidney cancer: A review and critical analysis of current literature[J]. Asian Journal of Urology, 2022, 9(3): 215-226. |
| [3] |
Stefano Puliatti,Ahmed Eissa,Enrico Checcucci,Pietro Piazza,Marco Amato,Stefania Ferretti,Simone Scarcella,Juan Gomez Rivas,Mark Taratkin,Josè Marenco,Ines Belenchon Rivero,Karl-Friedrich Kowalewski,Giovanni Cacciamani,Ahmed El-Sherbiny,Ahmed Zoeir,Abdelhamid M. El-Bahnasy,Ruben De Groote,Alexandre Mottrie,Salvatore Micali. New imaging technologies for robotic kidney cancer surgery[J]. Asian Journal of Urology, 2022, 9(3): 253-262. |
| [4] |
Riccardo Campi,Paolo Barzaghi,Alessio Pecoraro,Maria Lucia Gallo,Damiano Stracci,Alberto Mariotti,Saverio Giancane,Simone Agostini,Vincenzo Li Marzi,Arcangelo Sebastianelli,Pietro Spatafora,Mauro Gacci,Graziano Vignolini,Francesco Sessa,Paolo Muiesan,Sergio Serni. Contemporary techniques and outcomes of surgery for locally advanced renal cell carcinoma with focus on inferior vena cava thrombectomy: The value of a multidisciplinary team[J]. Asian Journal of Urology, 2022, 9(3): 272-281. |
| [5] |
Liang Zhang,Danlei Chen,Yingxian Pang,Xiao Guan,Xiaowen Xu,Cikui Wang,Qiao Xiao,Longfei Liu. Surgical treatment of large pheochromocytoma (>6 cm): A 10-year single-center experience[J]. Asian Journal of Urology, 2022, 9(3): 294-300. |
| [6] |
Toshihide Shishido,Takatsugu Okegawa,Kenjiro Hayashi,Kazuki Masuda,Satoru Taguchi,Yu Nakamura,Mitsuhiro Tambo,Hiroshi Fukuhara. Laparoscopic retroperitoneal lymph node dissection versus open retroperitoneal lymph node dissection for testicular cancer: A comparison of clinical and perioperative outcomes[J]. Asian Journal of Urology, 2022, 9(2): 119-124. |
| [7] |
Reza Alaghehbandan,Christopher G. Przybycin,Virginie Verkarre,Rohit Mehra. Chromophobe renal cell carcinoma: Novel molecular insights and clinicopathologic updates[J]. Asian Journal of Urology, 2022, 9(1): 1-11. |
| [8] |
Shuchi Gulati,Nicholas J. Vogelzang. Biomarkers in renal cell carcinoma: Are we there yet?[J]. Asian Journal of Urology, 2021, 8(4): 362-375. |
| [9] |
Wattanachai Ratanapornsompong,Suthep Pacharatakul,Premsant Sangkum,Chareon Leenanupan,Wisoot Kongcharoensombat. Effect of puboprostatic ligament preservation during robotic-assisted laparoscopic radical prostatectomy on early continence: Randomized controlled trial[J]. Asian Journal of Urology, 2021, 8(3): 260-268. |
| [10] |
Santosh Kumar,Abhishek Chandna,Vignesh Manoharan,Kalpesh M. Parmar,Subhajit Mandal. Conquering new battlegrounds: Successful management of isolated giant retrovesical hydatid cyst with robotic assistance[J]. Asian Journal of Urology, 2021, 8(3): 327-331. |
| [11] |
Fubo Wang,Chao Zhang,Fei Guo,Xia Sheng,Jin Ji,Yalong Xu,Zhi Cao,Ji Lyu,Xiaoying Lu,Bo Yang. The application of virtual reality training for anastomosis during robot-assisted radical prostatectomy[J]. Asian Journal of Urology, 2021, 8(2): 204-208. |
| [12] |
Marcio Covas Moschovas,Frederico Timóteo,Leonardo Lins,Oséas de Castro Neves,Kulthe Ramesh Seetharam Bhat,Vipul R. Patel. Robotic surgery techniques to approach benign prostatic hyperplasia disease: A comprehensive literature review and the state of art[J]. Asian Journal of Urology, 2021, 8(1): 81-88. |
| [13] |
Kulthe Ramesh Seetharam Bhat,Marcio Covas Moschovas,Fikret Fatih Onol,Travis Rogers,Shannon Roof,Vipul R. Patel,Oscar Schatloff. Robotic renal and adrenal oncologic surgery: A contemporary review[J]. Asian Journal of Urology, 2021, 8(1): 89-99. |
| [14] |
Marcio Covas Moschovas,Kulthe Ramesh Seetharam Bhat,Fikret Fatih Onol,Travis Rogers,Gabriel Ogaya-Pinies,Shannon Roof,Vipul R. Patel. Single-port technique evolution and current practice in urologic procedures[J]. Asian Journal of Urology, 2021, 8(1): 100-104. |
| [15] |
Yucong Zhang,Gongwei Long,Haojie Shang,Beichen Ding,Guoliang Sun,Wei Ouyang,Man Liu,Yuan Chen,Heng Li,Hua Xu,Zhangqun Ye. Comparison of the oncological, perioperative and functional outcomes of partial nephrectomy versus radical nephrectomy for clinical T1b renal cell carcinoma: A systematic review and meta-analysis of retrospective studies[J]. Asian Journal of Urology, 2021, 8(1): 117-125. |
|
|
|
|