|
|
|
| Laparoscopic retroperitoneal lymph node dissection versus open retroperitoneal lymph node dissection for testicular cancer: A comparison of clinical and perioperative outcomes |
Toshihide Shishidoa,b,Takatsugu Okegawab,*( ),Kenjiro Hayashia,b,Kazuki Masudab,Satoru Taguchib,Yu Nakamurab,Mitsuhiro Tambob,Hiroshi Fukuharab ),Kenjiro Hayashia,b,Kazuki Masudab,Satoru Taguchib,Yu Nakamurab,Mitsuhiro Tambob,Hiroshi Fukuharab
|
a Department of Urology, Hachioji Medical Center, Tokyo Medical University, 1163, Tatemachi,Hachioji, Tokyo, Japan
b Department of Urology, Kyorin University School of Medicine, 6-20-2 Shinkawa, Mitaka, Tokyo, Japan |
|
|
|
|
Abstract Objective: This study was performed to evaluate the clinical and perioperative outcomes of laparoscopic retroperitoneal lymph node dissection (L-RPLND) and open retroperitoneal lymph node dissection (O-RPLND) performed by one surgeon at a single center. Methods: We evaluated 30 patients with stage IIA germ cell tumors who underwent retroperitoneal lymph node dissection (15 underwent L-RPLND and 15 underwent O-RPLND) at our institution between April 1, 2010 and March 31, 2018. The clinical parameters were compared between patients who underwent L-RPLND using the retroperitoneal approach and those who underwent O-RPLND using the transperitoneal approach. There were no significant differences in the background characteristics of the two groups except for the median follow-up duration (46 months for L-RPLND and 71 months for O-RPLND, p=0.02). Results: L-RPLND was associated with a shorter mean operative time (mean 222 min for L-RPLND vs. 453 min for O-RPLND, p<0.001). There was significantly less blood loss during surgery in the L-RPLND group compared to the O-RPLND group (mean 165 mL for L-RPLND vs. 403 mL for O-RPLND, p<0.001). Parameters related to postoperative recovery were significantly better for the L-RPLND group than for the O-RPLND group. There were no differences in the histopathological characteristics between the two groups. No patients in either group exhibited disease recurrence. Conclusion: Patients who underwent L-RPLND had more rapid recovery, and shorter hospital stay compared to those who underwent O-RPLND; complications were comparable between the two groups. L-RPLND is an efficient procedure with the benefits of minimally invasive surgery.
|
|
Received: 18 March 2020
Available online: 20 April 2022
|
|
Corresponding Authors:
Takatsugu Okegawa
E-mail: toke@ks.kyorin-u.ac.jp
|
|
|

| Characteristic | L-RPLND, n=15 | O-RPLND, n=15 | p-Value | | Age, mean (range), year | 26 (18-52) | 27 (19-48) | 0.156 | | BMI, mean (range), kg/m2 | 24.2 (19.2-30.5) | 25.3 (18.9-31.1) | 0.207 | | Tumor side, left/right | 13/2 | 14/1 | 0.425 | | Pathology diagnosis, n (%) | 0.161 | | Seminoma | 6 (40.0) | 5 (33.3) | | | NSGCT | 9 (60.0) | 10 (66.7) | | Embryonal carcinoma | 2 (13.3) | 1 (6.7) | | Mixed | 6 (40.0) | 8 (53.3) | | Teratoma | 1 (6.7) | 1 (6.7) | | IGCCC, n (%) | 0.253 | | Good | 12 (80.0) | 11 (73.3) | | | Intermediate | 3 (20.0) | 4 (26.7) | | Poor | 0 | 0 | | Pre-chemotherapy tumor size, mean (range), mm | 25.6 (5-49) | 28.5 (8-48) | 0.318 | | Post-chemotherapy tumor size, mean (range), mm | 12.3 (4-23) | 13.1 (7-21) | 0.285 | | Blood loss, mean (range), mL | 165 (68-371) | 403 (220-1355) | <0.001 | | Operation time, mean (range), min | 222 (186-324) | 453 (280-780) | <0.001 | | Oral intake (postoperative), mean (range), day | 2 (2-5) | 3 (2-6) | 0.002 | | Permission of discharge (postoperative), mean (range), day | 8 (6-20) | 11 (10-18) | 0.014 | | Histology of RPLND, n (%) | 0.028 | | Necrosis | 13 (86.7) | 10 (66.7) | | | Teratoma | 1 (6.7) | 3 (20.0) | | Viable cancer | 1 (6.7) | 2 (13.3) | | Antegrade ejaculation, n (%) | 15 (100) | 14 (93.3) | 0.371 | | Follow-up, median (range), month | 46 (13-61) | 71 (22-96) | 0.023 |
|
|
Patient characteristics.
|
|
|
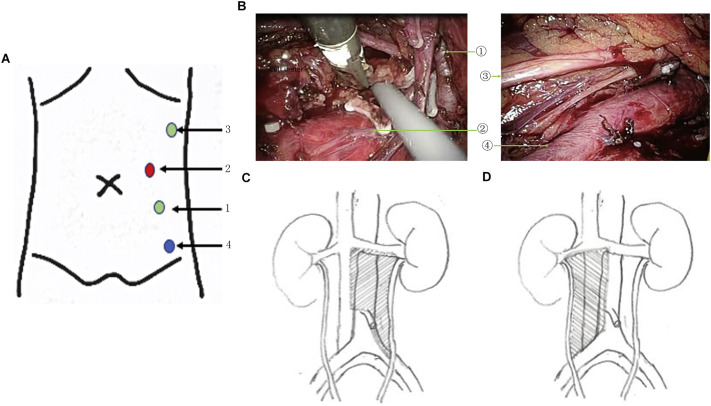
Placement of the ports for left-sided retroperitoneal lymph node dissection and intraoperative view. (A) Schematic diagram of placement of left retroperitoneal lymph node dissection port. 1. First port for the left hand (11 mm); 2. Second port for the laparoscope; 3. Third port for the right port (5 mm); 4. Fourth port (5 mm). (B) Para-aortal area after dissection shown (① Left renal artery; ② abdominal aorta; ③ Left ureter; ④ Left common iliac artery). (C) Template dissection limits for left-sided tumors consist of ureter (lateral), midpoint of vena cava (medial), bifurcation of iliac vessels (distal), and renal hilum (superior). (D) Template dissection limits for right-sided tumors consist of ureter (lateral), midpoint of aorta (medial), bifurcation of iliac vessels (inferior), and renal hilum (superior).
|
| Clavien-Dindo classification grade | L-RPLND, n=15 | O-RPLND, n=15 | | 1 | 2 | 3a | 1 | 2 | 3a | | Lymphatic cyst, n (%) | 0 | 1 (7) | 1 (7) | 0 | 0 | 0 | | Chyle leak, n (%) | 0 | 1 (7) | 0 | 0 | 1 (7) | 0 | | Sub-ileus, n (%) | 0 | 0 | 0 | 2 (14) | 0 | 0 | | Surgical site infection, n (%) | 0 | 0 | 0 | 2 (14) | 0 | 0 |
|
|
Perioperative complications.
|
| Variable | Janetschek et al. [11] | Poulakis et al. [12] | Abdel-Aziz et al. [13] | Nakamura et al. [14] | | L-RPLND | O-RPLND | L-RPLND | O-RPLND | L-RPLND | O-RPLND | L-RPLND | O-RPLND | | Patients, n | 29 | 30 | 21 | 29 | 22 | 6 | 14 | 14 | | Operative time, mean, min | 390 | 252 | 233 | 203 | 313 | 284 | 439 | 408 | | Estimated blood loss, mean, mL | N/A | N/A | 270 | 422 | 159 | 254 | 155 | 700 | | Length of stay, mean, day | 4.7 | 10.6 | 2 | 7 | 1.2 | 8.5 | 7 | 10.5 | | Complication rate, % | 41.4 | 30 | 15 | 86 | 18 | 17 | 50 | 35.7 | | Positive nodes, % | 27.6 | 16.7 | 19 | 24 | 32 | 0 | 0 | 21.4 |
|
|
Comparative studies of laparoscopic versus open retroperitoneal lymph node dissection: Operative data.
|
| [1] |
Hermans BP, Sweeney CJ, Foster RS, Einhorn LE, Donohue JP. Risk of systemic metastases in clinical stage I nonseminoma germ cell testis tumor managed by retroperitoneal lymph node dissection. J Urol 2000; 163:1721-4.
pmid: 10799168
|
| [2] |
Rukstalis DB, Chodak GW. Laparoscopic retroperitoneal lymph node dissection in a patient with stage 1 testicular carcinoma. J Urol 1992; 148:1907-9.
|
| [3] |
Arai Y, Kaiho Y, Yamada S, Saito H, Mitsuzuka K, Yamashita S, et al. Extraperitoneal laparoscopic retroperitoneal lymph node dissection after chemotherapy for nonseminomatous testicular germ-cell tumor: Surgical and oncological outcomes. Int Urol Nephrol 2012; 44:1389-95.
doi: 10.1007/s11255-012-0195-z
|
| [4] |
Weissbach L, Boedefeld EA. Localization of solitary and multiple metastases in stage II nonseminomatous testis tumor as basis for a modified staging lymph node dissection in stage I. J Urol 1987; 138:77-82.
doi: 10.1016/s0022-5347(17)42997-1
pmid: 3599225
|
| [5] |
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004; 240:205-13.
doi: 10.1097/01.sla.0000133083.54934.ae
|
| [6] |
Klotz L. Laparoscopic retroperitoneal lymphadenectomy for high-risk stage I nonseminomatous germ cell tumor: Report of four cases. Urology 1994; 43:752-6.
|
| [7] |
Janetschek G, Reissigl A, Peschel R, Hobisch A, Bartsch G. Laparoscopic retroperitoneal lymph node dissection for clinical stage I nonseminomatous testicular tumor. Urology 1994; 44:382-91.
pmid: 8073551
|
| [8] |
Palese MA, Su LM, Kavoussi LR. Laparoscopic retroperitoneal lymph node dissection after chemotherapy. Urology 2002; 60: 130-4.
|
| [9] |
Maldonado-Valadez R, Schilling D, Anastasiadis AG, Sturm W, Stenzl A, Corvin S. Post-chemotherapy laparoscopic retroperitoneal lymph-node dissection in testis cancer patients. J Endourol 2007; 21:1501-4.
doi: 10.1089/end.2006.0441
pmid: 18186691
|
| [10] |
Calestroupat JP, Sanchez-Salas R, Cathelineau X, Rozet F, Galiano M, Smyth G, et al. Postchemotherapy laparoscopic retroperitoneal lymph node dissection in nonseminomatous germ-cell tumor. J Endourol 2009; 23:645-50.
doi: 10.1089/end.2008.0423
|
| [11] |
Janetschek G, Hobisch A, Höltl L, Bartsch G. Retroperitoneal lymphadenectomy for clinical stage I nonseminomatous testicular tumor: Laparoscopy versus open surgery and impact of learning curve. J Urol 1996; 156:89-94.
doi: 10.1016/s0022-5347(01)65948-2
pmid: 8648847
|
| [12] |
Poulakis V, Skriapas K, de Vries R, Dillenburg W, Ferakis N, Witzsch U, et al. Quality of life after laparoscopic and open retroperitoneal lymph node dissection in clinical stage I nonseminomatous germ cell tumor: A comparison study. Urology 2006; 68:154-60.
|
| [13] |
Abdel-Aziz KF, Anderson JK, Svatek R, Margulis VM, Sagalowski AI, Cadeddu JA. Laparoscopic and open retroperitoneal lymph-node dissection for clinical stage I nonseminomatous germ-cell cancer tumors. J Endourol 2006; 20: 627-31.
pmid: 16999613
|
| [14] |
Nakamura T, Kawauchi A, Oishi M, Ueda T, Shiraishi T, Nakanishi H, et al. Post-chemotherapy laparoscopic retroperitoneal lymph node dissection is feasible for stage IIA/B nonseminoma germ cell tumors. Int J Clin Oncol 2016; 21:791-5.
doi: 10.1007/s10147-015-0934-0
|
| [15] |
Rassweiler JJ, Scheitlin W, Heidenreich A, Laguna MP, Janetschek G. Laparoscopic retroperitoneal lymph node dissection: Does it still have a role in the management of clinical stage I nonseminomatous testis cancer? A European perspective. Eur Urol 2008; 54:1004-15.
doi: 10.1016/j.eururo.2008.08.022
pmid: 18722704
|
| [16] |
Tselos A, Moris D, Tsilimigras DI, Fragkiadis E, Mpaili E, Sakarellos P. Vet al. Robot-assisted retroperitoneal lymphadenectomy in testicular cancer treatment: A systematic review. J Laparoendosc Adv Surg Tech A 2018; 28:682-9.
doi: 10.1089/lap.2017.0672
|
| [1] |
Christian Winter,Andreas Hiester. Treatment of clinical stage I non-seminoma[J]. Asian Journal of Urology, 2021, 8(2): 161-169. |
| [2] |
Zoe Loh,Todd G. Manning,Jonathan S. O’Brien,Marlon Perera,Nathan Lawrentschuk. Mesenteric metastases from mature teratoma of the testis: A case report[J]. Asian Journal of Urology, 2020, 7(3): 322-325. |
| [3] |
Su Jiarui,Jonathan Aslim Edwin,Aydin Hakan,HoonTan Puay,Sun SienHo Henry. A rare case of isolated castrate resistant bilateral testicular metastases in advanced prostate cancer[J]. Asian Journal of Urology, 2018, 5(2): 127-130. |
|
|
|
|