|
|
|
| The impact of chemotherapy-naïve open radical cystectomy delay and perioperative transfusion on the recurrence-free survival: A perioperative parameters-based nomogram |
Ahmed M. Harraz*( ),Ahmed Elkarta,Mohamed H. Zahran,Ahmed Mosbah,Atallah A. Shaaban,Hassan Abol-Enein ),Ahmed Elkarta,Mohamed H. Zahran,Ahmed Mosbah,Atallah A. Shaaban,Hassan Abol-Enein
|
| Urology and Nephrology Center, Mansoura University, Egypt |
|
|
|
|
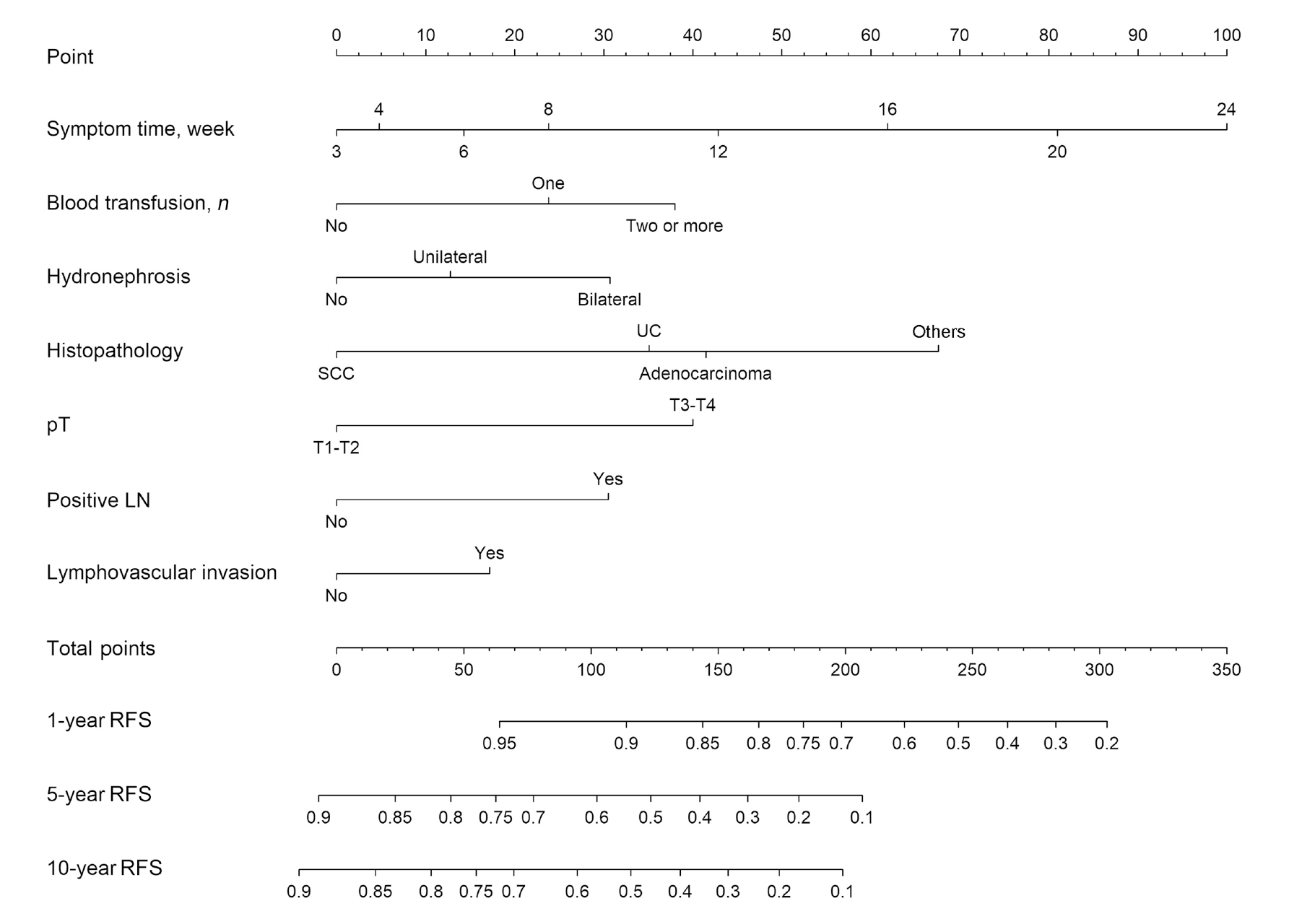
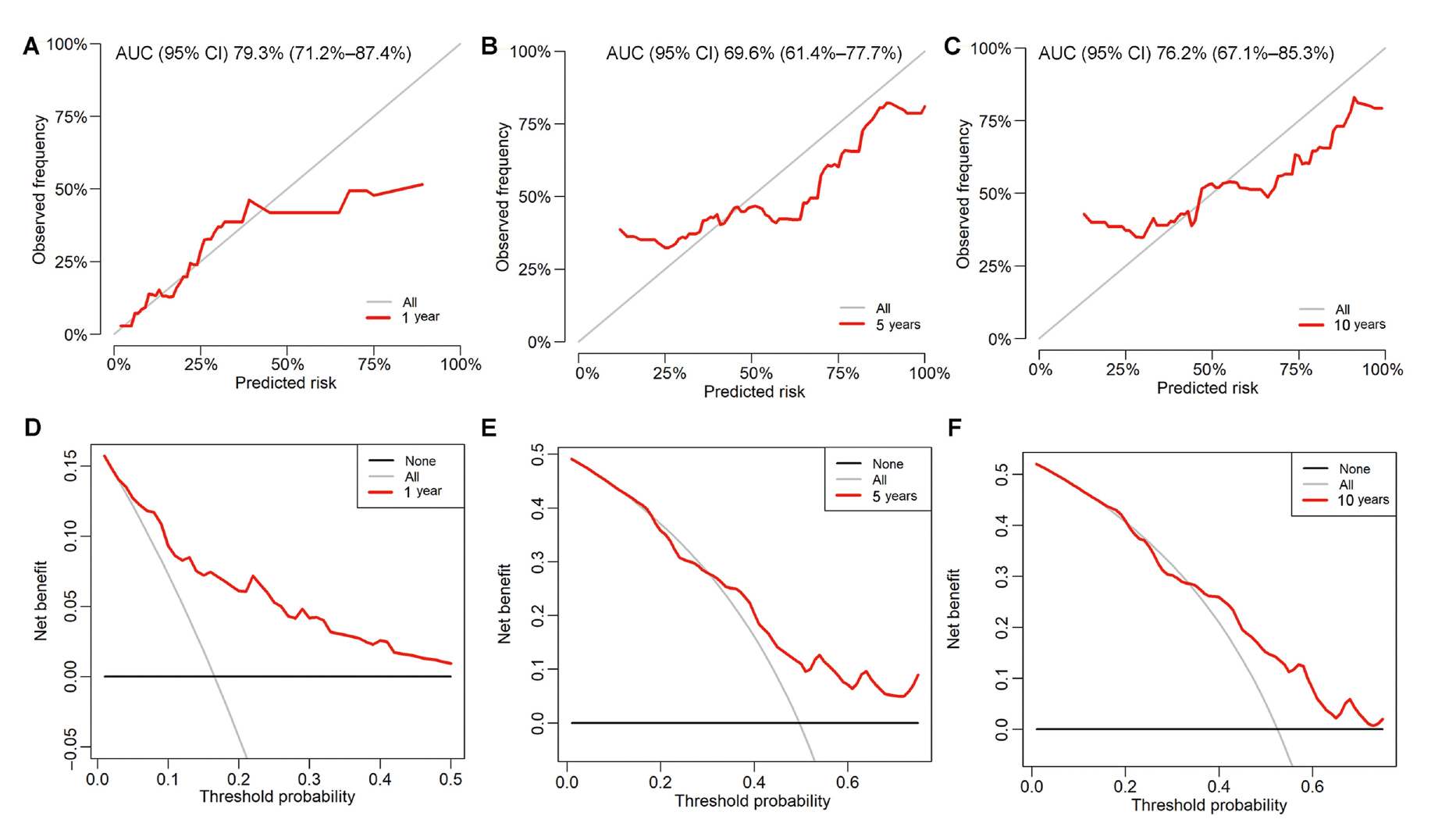
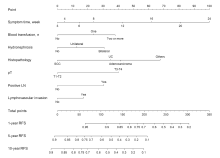
Abstract Objective: To develop and internally validate a nomogram to predict recurrence-free survival (RFS) including the time to radical cystectomy (RC) and perioperative blood transfusion (PBT) as potential predictors. Methods: Patients who underwent open RC and ileal conduit between January 1996 to December 2016 were split into developing (n=948) and validating (n=237) cohorts. The time to radical cystectomy (TTC) was defined as the interval between the onset of symptoms and RC. The regression coefficients of the independent predictors obtained by Cox regression were used to construct the nomogram. Discrimination, validation, and clinical usefulness in the validation cohort were assessed by the area under the curve, the calibration plot, and decision curve analysis. Results: In the developing dataset, the 1-, 5-, and 10-year RFS were 83.0%, 47.2%, and 44.4%, respectively. On multivariate analysis, independent predictors were TTC (hazards ratio [HR] 1.07, 95% confidence interval [CI] 1.05-1.08, p<0.001), PBT (one unit: HR 1.40, 95% CI 1.03-1.90, p=0.03; two or more units: HR 1.72, 95% CI 1.29-2.29, p<0.001), bilateral hydronephrosis (HR 1.54, 95% CI 1.21-1.97, p<0.001), squamous cell carcinoma (HR 0.60, 95% CI 0.45-0.81, p=0.001), pT3-T4 (HR 1.77, 95% CI 1.41-2.22, p<0.001), lymph node status (HR 1.53, 95% CI 1.21-1.95, p<0.001), and lymphovascular invasion (HR 1.28, 95% CI 1.01-1.62, p=0.044). The areas under the curve in the validation dataset were 79.3%, 69.6%, and 76.2%, for 1-, 5-, and 10-year RFS, respectively. Calibration plots showed considerable correspondence between predicted and actual survival probabilities. The decision curve analysis revealed a better net benefit of the nomogram. Conclusion: A nomogram with good discrimination, validation, and clinical utility was constructed utilizing TTC and PBT in addition to standard pathological criteria.
|
|
Received: 30 April 2022
Available online: 20 April 2024
|
|
Corresponding Authors:
* E-mail addresses: ahmed.harraz@hotmail.com,harraza@mans.edu.eg (A.M. Harraz).
|
|
|

| Variable | Developing cohort (n=948) | Validating cohort (n=237) | Total (n=1185) | p-Value | | Age, year | 60.2±8.3 | 60.3±8.1 | 60.3±8.3 | 0.9 | | Albumin, g/dL | 3.5±0.5 | 3.5±0.4 | 3.5±0.5 | 0.4 | | BMI, kg/m2 | 27.6±4.8 | 27.9±5.2 | 27.6±4.9 | 0.4 | | Discharge eGFR, mL/min/1.73 m2 | 65.2±24.9 | 65.5±24.3 | 65.3±24.8 | 0.8 | | Hb, g/dL | 12.7±1.7 | 12.7±1.7 | 12.7±1.7 | 0.7 | | Platelet, x109/L | 273.5±105.3 | 277.8±102.3 | 274.4±104.7 | 0.5 | | TTC, weeks | 12 (4-12) | 12 (4-12) | 12 (4-12) | 0.4 | | Anemia | 0.6 | | No | 441 (46.5) | 115 (48.5) | 556 (46.9) | | | Yes | 507 (53.5) | 122 (51.5) | 629 (53.1) | | | PBT | 0.4 | | No | 182 (19.2) | 42 (17.7) | 224 (18.9) | | | One | 304 (32.1) | 69 (29.1) | 373 (31.5) | | | Two or more | 462 (48.7) | 126 (53.2) | 588 (49.6) | | | Albumin | 0.7 | | >3.5 g/dL | 430 (45.4) | 104 (43.9) | 534 (45.1) | | | ≤3.5 g/dL | 518 (54.6) | 133 (56.1) | 651 (54.9) | | | BMI | 0.7 | | <30 kg/m2 | 658 (69.4) | 161 (67.9) | 819 (69.1) | | | ≥30 kg/m2 | 290 (30.6) | 76 (32.1) | 366 (30.9) | | | Diabetes mellitus | 0.1 | | No | 807 (85.1) | 211 (89.0) | 1018 (85.9) | | | Yes | 141 (14.9) | 26 (11.0) | 167 (14.1) | | | Hypertension | 0.4 | | No | 759 (80.1) | 184 (77.6) | 943 (79.6) | | | Yes | 189 (19.9) | 53 (22.4) | 242 (20.4) | | | CCI | 0.1 | | I | 767 (80.9) | 184 (77.6) | 951 (80.3) | | | II | 167 (17.6) | 45 (19.0) | 212 (17.9) | | | III | 14 (1.5) | 8 (3.4) | 22 (1.9) | | | Gender | 0.4 | | Male | 758 (80.0) | 195 (82.3) | 953 (80.4) | | | Female | 190 (20.0) | 42 (17.7) | 232 (19.6) | | | Smoking | 0.2 | | Never | 308 (32.5) | 75 (31.6) | 383 (32.3) | | | Former | 112 (11.8) | 37 (15.6) | 149 (12.6) | | | Current | 528 (55.7) | 125 (52.7) | 653 (55.1) | | | Solitary kidney | 0.8 | | No | 756 (79.7) | 191 (80.6) | 947 (79.9) | | | Yes | 192 (20.3) | 46 (19.4) | 238 (20.1) | | | Hydronephrosis | 0.3 | | No | 420 (44.3) | 118 (49.8) | 538 (45.4) | | | Unilateral | 312 (32.9) | 72 (30.4) | 384 (32.4) | | | Bilateral | 216 (22.8) | 47 (19.8) | 263 (22.2) | | | History of NMIBC | 0.04 | | No | 842 (88.8) | 198 (83.5) | 1040 (87.8) | | | Yes | 106 (11.2) | 39 (16.5) | 145 (12.2) | | | Cell type | 0.4 | | UC | 705 (74.4) | 170 (71.7) | 875 (73.8) | | | SCC | 175 (18.5) | 53 (22.4) | 228 (19.2) | | | Adeno | 33 (3.5) | 8 (3.4) | 41 (3.5) | | | Others | 35 (3.7) | 6 (2.5) | 41 (3.5) | | | Positive lymph node | 0.9 | | No | 653 (68.9) | 162 (68.4) | 815 (68.8) | | | Yes | 295 (31.1) | 75 (31.6) | 370 (31.2) | | | LVI | | No | 640 (67.5) | 165 (69.6) | 805 (67.9) | 0.5 | | Yes | 308 (32.5) | 72 (30.4) | 380 (32.1) | | | pT | | T1-T2 | 425 (44.8) | 113 (47.7) | 538 (45.4) | 0.4 | | T3-T4 | 523 (55.2) | 124 (52.3) | 647 (54.6) | | | High-grade POC | | No | 874 (92.2) | 214 (90.3) | 1088 (91.8) | 0.4 | | Yes | 74 (7.8) | 23 (9.7) | 97 (8.2) | | | Distant metastasis | | No | 735 (77.5) | 188 (79.3) | 923 (77.9) | 0.6 | | Yes | 213 (22.5) | 49 (20.7) | 262 (22.1) | | | Local recurrence | | No | 690 (72.8) | 181 (76.4) | 871 (73.5) | 0.3 | | Yes | 258 (27.2) | 56 (23.6) | 314 (26.5) | | | Follow-up, month | 31.5 (11.0-72.2) | 29 (11-72) | 31 (11-72) | 0.8 |
|
|
The differences between the developing and validating cohorts in patients who underwent radical cystectomy and ileal conduit.
|
| Variable | Univariate | Multivariate | | HR (95% CI) | p-Value | HR (95% CI) | p-Value | | Age, 10 yearsa | 1.18 (1.05-1.33) | 0.005 | - | -b | | TTC, week | 1.08 (1.06-1.09) | <0.001 | 1.07 (1.05-1.08) | <0.001 | | Anemia | | No | Reference | - | - | - | | Yes | 1.33 (1.10-1.62) | 0.004 | - | -b | | PBT | 0.001 | | No | Reference | - | - | | | One | 1.48 (1.09-2.00) | 0.01 | 1.40 (1.03-1.90) | 0.03 | | Two or more | 1.82 (1.37-2.42) | <0.001 | 1.72 (1.29-2.29) | <0.001 | | Hydronephrosis | 0.002 | | No | Reference | - | - | | | Unilateral | 1.30 (1.04-1.63) | 0.02 | 1.20 (0.95-1.51) | 0.1 | | Bilateral | 1.73 (1.36-2.20) | <0.001 | 1.54 (1.21-1.97) | <0.001 | | Cell type | 0.001 | | UC | Reference | - | - | | | SCC | 0.50 (0.38-0.66) | <0.001 | 0.60 (0.45-0.81) | 0.001 | | Adeno | 1.01 (0.60-1.69) | 0.9 | 1.09 (0.64-1.84) | 0.7 | | Others | 1.17 (0.71-1.94) | 0.5 | 1.58 (0.95-2.64) | 0.07 | | Positive LN | | No | Reference | - | - | - | | Yes | 2.38 (1.95-2.91) | <0.001 | 1.53 (1.21-1.95) | <0.001 | | LVI | | No | Reference | - | - | - | | Yes | 2.21 (1.81-2.70) | <0.001 | 1.28 (1.01-1.62) | 0.044 | | pT | | T1-T2 | Reference | - | - | - | | T3-T4 | 2.17 (1.78-2.66) | <0.001 | 1.77 (1.41-2.22) | <0.001 |
|
|
Univariate and multivariate Cox regression model for factors associated with independent predictors of cancer-specific survival in patients underwent radical cystectomy.
|
|
|
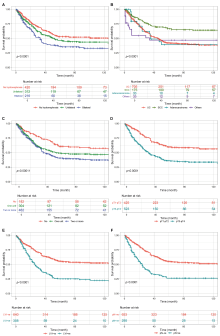
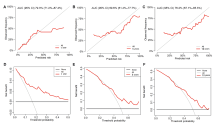
Kaplan-Meier survival curves for significant factors associated with recurrence-free survival in the developing set of patients who underwent radical cystectomy. (A) Hydronephrosis; (B) Histopathological diagnosis; (C) Perioperative blood transfusion (number of packed red blood cells transfused); (D) pT; (E) Lymphovascular invasion; (F) pN. p-Values were obtained by the log-rank test. UC, urothelial carcinoma; SCC, squamous cell carcinoma; pT, pathological tumor stage; pN, pathological lymph node; LVI?ve, negative lymphovascular invasion; LVI+ve, positive lymphovascular invasion; pN?ve, pathological negative lymph node; pN+ve, pathological positive lymph node.
|
|
|
Nomogram to predict the probability of 1-, 5-, and 10-year RFS in patients who underwent radical cystectomy and ileal conduit. LN, lymph node; n, number of packed red blood cells; SCC, squamous cell carcinoma; pT, pathological tumor stage; RFS, recurrence-free survival.
|
|
|
The validation dataset. (A-C) Calibration plot of the predicted probabilities of recurrence-free survival and the actual probabilities obtained by the Kaplan-Meier method: (A) 1 year; (B) 5 years; (C) 10 years. The closer the values to the diagonal line, the better the calibration. (D-F) Decision curve analysis depicting the net benefit against a range of threshold probabilities in comparison to treating-all or treating-none: (D) 1 year; (E) 5 years; (F) 10 years. AUC, area under the curve; CI, confidence interval.
|
| [1] |
Kluth LA, Black PC, BochnerBH, Catto J, Lerner SP, Stenzl A, et al. Prognostic and prediction tools in bladder cancer: a comprehensive review of the literature. Eur Urol 2015; 68:238e53.
doi: 10.1016/j.eururo.2015.01.032
pmid: 25709027
|
| [2] |
Williams SB, Huo J, Chu Y, Baillargeon JG, Daskivich T, Kuo YF, et al. Cancer and all-cause mortality in bladder cancer patients undergoing radical cystectomy: development and validation of a nomogram for treatment decision-making. Urology 2017; 110:76e83.
doi: S0090-4295(17)30886-5
pmid: 28847688
|
| [3] |
Di Trapani E, Sanchez-Salas R, Gandaglia G, Rocchini L, Moschini M, Lizee D, et al. A nomogram predicting the cancerspecific mortality in patients eligible for radical cystectomy evaluating clinical data and neoadjuvant cisplatinum-based chemotherapy. World J Urol 2016; 34:207e13.
doi: 10.1007/s00345-015-1640-2
pmid: 26198750
|
| [4] |
Simone G, Bianchi M, Giannarelli D, Daneshmand S, Papalia R, Ferriero M, et al. Development and external validation of nomograms predicting disease-free and cancer-specific survival after radical cystectomy. World J Urol 2015; 33:1419e28.
doi: 10.1007/s00345-014-1465-4
pmid: 25542395
|
| [5] |
el-Mekresh M, Akl A, Mosbah A, Abdel-Latif M, Abol-Enein H, Ghoneim MA. Prediction of survival after radical cystectomy for invasive bladder carcinoma: risk group stratification, nomograms or artificial neural networks? J Urol 2009; 182: 466e72. discussion 72.
doi: 10.1016/j.juro.2009.04.018
pmid: 19524972
|
| [6] |
Boeri L, Soligo M, Frank I, Boorjian SA, Thompson RH, Tollefson M, et al. Delaying radical cystectomy after neoadjuvant chemotherapy for muscle-invasive bladder cancer is associated with adverse survival outcomes. Eur Urol Oncol 2019; 2:390e6.
doi: S2588-9311(18)30161-5
pmid: 31277775
|
| [7] |
Audenet F, Sfakianos JP, Waingankar N, Ruel NH, Galsky MD, Yuh BE, et al. A delay ≥8 weeks to neoadjuvant chemotherapy before radical cystectomy increases the risk of upstaging. Urol Oncol 2019;37:116e22.
|
| [8] |
Chu AT, Holt SK, Wright JL, Ramos JD, Grivas P, Yu EY, et al. Delays in radical cystectomy for muscle-invasive bladder cancer. Cancer 2019; 125:2011e7.
doi: 10.1002/cncr.32048
pmid: 30840335
|
| [9] |
Weiner AB, Keeter MK, Manjunath A, Meeks JJ. Discrepancies in staging, treatment, and delays to treatment may explain disparities in bladder cancer outcomes: an update from the National Cancer Data Base (2004e2013). Urol Oncol 2018; 36: 237e9e17. https://doi.org/10.1016/j.urolonc.2017.12.015.
|
| [10] |
Santos F, Dragomir A, Kassouf W, Franco EL, Aprikian A. Predictors of preoperative delays before radical cystectomy for bladder cancer in Quebec, Canada: a population-based study. BJU Int 2015; 115:389e96.
doi: 10.1111/bju.12742
pmid: 24656061
|
| [11] |
Russell B, Liedberg F, Khan MS, Nair R, Thurairaja R, Malde S, et al. A Systematic review and meta-analysis of delay in radical cystectomy and the effect on survival in bladder cancer patients. Eur Urol Oncol 2020; 3:239e49.
doi: S2588-9311(19)30151-8
pmid: 31668714
|
| [12] |
Wallis CJD, Novara G, Marandino L, Bex A, Kamat AM, Karnes RJ, et al. Risks from deferring treatment for genitourinary cancers: a collaborative review to aid triage and management during the COVID-19 pandemic. Eur Urol 2020; 78:29e42.
doi: S0302-2838(20)30331-6
pmid: 32414626
|
| [13] |
Mmeje CO, Benson CR, Nogueras-Gonzalez GM, Jayaratna IS, Gao J, Siefker-Radtke AO, et al. Determining the optimal time for radical cystectomy after neoadjuvant chemotherapy. BJU Int 2018; 122:89e98.
doi: 10.1111/bju.14211
pmid: 29569824
|
| [14] |
Antonelli A, Zamboni S, Palumbo C, Belotti S, Lattarulo M, Furlan M, et al. Prognostic role of delay before radical cystectomy: retrospective analysis of a single-centre cohort with 376 patients. Minerva Urol Nefrol 2018; 70:494e500.
|
| [15] |
Bruins HM, Aben KK, Arends TJ, van der Heijden AG, Witjes AJ. The effect of the time interval between diagnosis of muscle-invasive bladder cancer and radical cystectomy on staging and survival: a Netherlands Cancer Registry analysis. Urol Oncol 2016; 34:166.e1e6. https://doi.org/10.1016/j.urolonc.2015.11.006.
|
| [16] |
Furrer MA, Fellmann A, Schneider MP, Thalmann GN, Burkhard FC, Wuethrich PY. Impact of packed red blood cells and fresh frozen plasma given during radical cystectomy and urinary diversion on cancer-related outcome and survival: an observational cohort study. Eur Urol Focus 2018; 4:916e23.
doi: S2405-4569(17)30214-6
pmid: 28951117
|
| [17] |
Ceanga AI, Ceanga M, Eveslage M, Herrmann E, Fischer D, Haferkamp A, et al. Preoperative anemia and extensive transfusion during stay-in-hospital are critical for patient’s mortality: a retrospective multicenter cohort study of oncological patients undergoing radical cystectomy. Transfus Apher Sci 2018; 57:739e45.
doi: 10.1016/j.transci.2018.08.003
|
| [18] |
Buchner A, Grimm T, Schneevoigt BS, Wittmann G, Kretschmer A, Jokisch F, et al. Dramatic impact of blood transfusion on cancer-specific survival after radical cystectomy irrespective of tumor stage. Scand J Urol 2017; 51: 130e6.
doi: 10.1080/21681805.2017.1295399
pmid: 28332428
|
| [19] |
Schulz GB, Grimm T, Buchner A, Jokisch F, Grabbert M, Schneevoigt BS, et al. Prognostic value of the preoperative platelet-to-leukocyte ratio for oncologic outcomes in patients undergoing radical cystectomy for bladder cancer. Clin Genitourin Cancer 2017; 15:e915e21. https://doi.org/10.1016/j.clgc.2017.05.009.
|
| [20] |
Santos F, Dragomir A, Kassouf W, Franco E, Aprikian A. Urologist referral delay and its impact on survival after radical cystectomy for bladder cancer. Curr Oncol 2015; 22:e20e6. https://doi.org/10.3747/co.22.2052.
|
| [21] |
Rosenblatt R, Lorentzi G, Bahar M, Asad D, Forsman R, Johansson M, et al. Blood transfusions during neoadjuvant chemotherapy for muscle-invasive urinary bladder cancer may have a negative impact on overall survival. Scand J Urol 2020; 54:46e51.
doi: 10.1080/21681805.2020.1716067
pmid: 31960752
|
| [22] |
Vamvakas EC, Blajchman MA. Transfusion-related immunomodulation (TRIM): an update. Blood Rev 2007; 21:327e48.
doi: 10.1016/j.blre.2007.07.003
pmid: 17804128
|
| [23] |
Xia L, Guzzo TJ. Preoperative anemia and low hemoglobin level are associated with worse clinical outcomes in patients with bladder cancer undergoing radical cystectomy: a metaanalysis. Clin Genitourin Cancer 2017; 15:263e272.e4. https://doi.org/10.1016/j.clgc.2016.08.017.
doi: 10.1016/j.clgc.2016.08.017
|
| [24] |
Moschini M. The impact of perioperative blood transfusion on survival outcomes in radical cystectomy patients. Transl Androl Urol 2017; 6:1205e7.
doi: 10.21037/tau.2017.11.25
pmid: 29354514
|
| [25] |
Zhou N, Tian F, Feng Y, Zhao K, Chen L, Fan R, et al. Perioperative outcomes of intracorporeal robot-assisted radical cystectomy versus open radical cystectomy: a systematic review and meta-analysis of comparative studies. Int J Surg 2021; 94:106137. https://doi.org/10.1016/j.ijsu.2021.106137.
doi: 10.1016/j.ijsu.2021.106137
|
| [26] |
Mastroianni R, Ferriero M, Tuderti G, Anceschi U, Bove AM, Brassetti A, et al. Open radical cystectomy versus robotassisted radical cystectomy with intracorporeal urinary diversion: early outcomes of a single-center randomized controlled trial. J Urol 2022; 207:982e92.
doi: 10.1097/JU.0000000000002422
pmid: 34986007
|
| [27] |
Catto JWF, Khetrapal P, Ricciardi F, Ambler G, Williams NR, Al-Hammouri T, et al. Effect of robot-assisted radical cystectomy with intracorporeal urinary diversion vs. open radical cystectomy on 90-day morbidity and mortality among patients with bladder cancer: a randomized clinical trial. JAMA 2022; 327:2092e103.
doi: 10.1001/jama.2022.7393
pmid: 35569079
|
| [28] |
Su X, Wu K, Wang S, Su W, Li C, Li B, et al. The impact of orthotopic neobladder vs. ileal conduit urinary diversion after cystectomy on the survival outcomes in patients with bladder cancer: a propensity score matched analysis. Cancer Med 2020; 9:7590e600.
doi: 10.1002/cam4.v9.20
|
| [29] |
Flegar L, Kraywinkel K, Zacharis A, Aksoy C, Koch R, Eisenmenger N, et al. Treatment trends for muscle-invasive bladder cancer in Germany from 2006 to 2019. World J Urol 2022; 40:1715e21.
doi: 10.1007/s00345-022-04017-z
|
| [30] |
Mitra AP, Cai J, Miranda G, Bhanvadia S, Quinn DI, Schuckman AK, et al. Management trends and outcomes of patients undergoing radical cystectomy for urothelial carcinoma of the bladder: evolution of the university of Southern California experience over 3347 cases. J Urol 2022; 207:302e13.
doi: 10.1097/JU.0000000000002242
|
| [1] |
Jordan M. Rich, Shivaram Cumarasamy, Daniel Ranti, Etienne Lavallee, Kyrollis Attalla, John P. Sfakianos, Nikhil Waingankar, Peter N. Wiklund, Reza Mehrazin. Contemporary outcomes of patients undergoing robotic-assisted radical cystectomy: A comparative analysis between intracorporeal ileal conduit and neobladder urinary diversions[J]. Asian Journal of Urology, 2023, 10(4): 446-452. |
| [2] |
Angelo Territo, Alessandro Uleri, Andrea Gallioli, Josep Maria Gaya, Paolo Verri, Giuseppe Basile, Alba Farré, Alejandra Bravo, Alessandro Tedde, Óscar Rodríguez Faba, Joan Palou, Alberto Breda. Robot-assisted oncologic pelvic surgery with Hugo™ robot-assisted surgery system: A single-center experience[J]. Asian Journal of Urology, 2023, 10(4): 461-466. |
| [3] |
Giorgio Mazzon,Simon Choong,Antonio Celia. Stone-scoring systems for predicting complications in percutaneous nephrolithotomy: A systematic review of the literature[J]. Asian Journal of Urology, 2023, 10(3): 226-238. |
| [4] |
. Reliability of nephrolithometric nomograms in patients treated with minimally invasive percutaneous nephrolithotomy: A precision study[J]. Asian Journal of Urology, 2023, 10(1): 70-80. |
| [5] |
Leandro Blas,Masaki Shiota,Shohei Nagakawa,Shigehiro Tsukahara,Takashi Matsumoto,Ken Lee,Keisuke Monji,Eiji Kashiwagi,Junichi Inokuchi,Masatoshi Eto. Validation of user-friendly models predicting extracapsular extension in prostate cancer patients[J]. Asian Journal of Urology, 2023, 10(1): 81-88. |
| [6] |
Victor Chalfant,Michael L. BluteJr.,Peter Silberstein. Treatment trends of muscle invasive bladder cancer: Evidence from the Surveillance, Epidemiology, and End Results database, 1988 to 2013[J]. Asian Journal of Urology, 2023, 10(1): 9-18. |
| [7] |
Abhay D. Mahajan,Lakshman P. Singh,Prashant P. Darakh,Sandeep T. Bathe,Martand G. Patil,Arpit R. Sharma. Uroflowmetric analysis and derivation of nomograms for normal paediatric Indian population between 5 to 15 years of age[J]. Asian Journal of Urology, 2022, 9(2): 125-131. |
| [8] |
Yucong Zhang,Gongwei Long,Haojie Shang,Beichen Ding,Guoliang Sun,Wei Ouyang,Man Liu,Yuan Chen,Heng Li,Hua Xu,Zhangqun Ye. Comparison of the oncological, perioperative and functional outcomes of partial nephrectomy versus radical nephrectomy for clinical T1b renal cell carcinoma: A systematic review and meta-analysis of retrospective studies[J]. Asian Journal of Urology, 2021, 8(1): 117-125. |
| [9] |
Marcio Covas Moschovas,Kulthe Ramesh Seetharam Bhat,Cathy Jenson,Vipul R. Patel,Gabriel Ogaya-Pinies. Robtic-assisted radical cystectomy: Literature review[J]. Asian Journal of Urology, 2021, 8(1): 14-19. |
| [10] |
Hugo Otaola-Arca,Rafael Coelho,Vipul R. Patel,Marcelo Orvieto. Totally intracorporeal robot-assisted urinary diversion for bladder cancer (Part 1). Review and detailed characterization of ileal conduit and modified Indiana pouch[J]. Asian Journal of Urology, 2021, 8(1): 50-62. |
| [11] |
Hugo Otaola-Arca,Kulthe Ramesh Seetharam Bhat,Vipul R. Patel,Marcio Covas Moschovas,Marcelo Orvieto. Totally intracorporeal robot-assisted urinary diversion for bladder cancer (part 2). Review and detailed characterization of the existing intracorporeal orthotopic ileal neobladder[J]. Asian Journal of Urology, 2021, 8(1): 63-80. |
| [12] |
Carlotta Palumbo,Elio Mazzone,Francesco A. Mistretta,Sophie Knipper,Zhe Tian,Paul Perrotte,Francesco Montorsi,Shahrokh F. Shariat,Fred Saad,Claudio Simeone,Alberto Briganti,Alessandro Antonelli,Pierre I. Karakiewicz. Primary lymphomas of the genitourinary tract: A population-based study[J]. Asian Journal of Urology, 2020, 7(4): 332-339. |
| [13] |
Weibin Xie,Junming Bi,Qiang Wei,Ping Han,Dongkui Song,Lei Shi,Dingwei Ye,Yijun Shen,Xin Gou,Weiyang He,Shaogang Wang,Zheng Liu,Jinhai Fan,Kaijie Wu,Zhiwen Chen,Xiaozhou Zhou,Chuize Kong,Yang Liu,Chunxiao Liu,Abai Xu,Baiye Jin,Guanghou Fu,Wei Xue,Haige Chen,Tiejun Pan,Zhong Tu,Tianxin Lin,Jian Huang. Survival after radical cystectomy for bladder cancer: Multicenter comparison between minimally invasive and open approaches[J]. Asian Journal of Urology, 2020, 7(3): 291-300. |
| [14] |
Sunny Goel,Rahul J. Sinha,Ved Bhaskar,Ruchir Aeron,Ashish Sharma,Vishwajeet Singh. Role of gemcitabine and cisplatin as neoadjuvant chemotherapy in muscle invasive bladder cancer: Experience over the last decade[J]. Asian Journal of Urology, 2019, 6(3): 222-229. |
| [15] |
Olivier Rouviere,Paul Cezar Moldovan. The current role of prostate multiparametric magnetic resonance imaging[J]. Asian Journal of Urology, 2019, 6(2): 137-145. |
|
|
|
|