|
|
|
| Clinical outcomes for men with positive surgical margins after radical prostatectomy—results from the South Australian Prostate Cancer Clinical Outcomes Collaborative community-based registry |
Kerri R. Beckmanna,b,*( ),Michael E. O'Callaghanc,Andrew D. Vincentd,Kim L. Morettia,c,e,Nicholas R. Brookf ),Michael E. O'Callaghanc,Andrew D. Vincentd,Kim L. Morettia,c,e,Nicholas R. Brookf
|
aCancer Epidemiology and Population Health Research, University of South Australia, Adelaide, Australia
bTranslational Oncology and Urology Research, Division of Pharmaceutical and Cancer Studies, Kings College London, London, UK
cSouth Australian Prostate Cancer Clinical Outcomes Collaborative, Flinders Medical Centre, Adelaide, Australia
dThe Freemason's Foundation Centre for Men's Health, Adelaide Medical School, University of Adelaide, Adelaide, Australia
eDiscipline of Surgery, University of Adelaide, Adelaide, Australia
fDepartment of Urology, Royal Adelaide Hospital, Adelaide, Australia |
|
|
|
|
Abstract Objective: Positive surgical margins (PSMs) after radical prostatectomy (RP) indicate failure of surgery to completely clear cancer. PSMs confer an increased risk of biochemical recurrence (BCR), but how more robust outcomes are affected is unclear. This study investigated factors associated with PSMs following RP and determined their impact on clinical outcomes (BCR, second treatment [radiotherapy and/or androgen deprivation therapy], and prostate cancer-specific mortality [PCSM]). Methods: The study cohort included men diagnosed with prostate cancer (pT2-3b/N0/M0) between January 1998 and June 2016 who underwent RP from the South Australian Prostate Cancer Clinical Outcomes Collaborative database. Factors associated with risk of PSMs were identified using Poisson regression. The impact of PSMs on clinical outcomes (BCR, second treatment, and PCSM) was assessed using competing risk regression. Results: Of the 2827 eligible participants, 28% had PSMs—10% apical, 6% bladder neck, 17% posterolateral, and 5% at multiple locations. Median follow-up was 9.6 years with 81 deaths from prostate cancer recorded. Likelihood of PSM increased with higher pathological grade and pathological tumor stage, and greater tumour volume, but decreased with increasing surgeon volume (odds ratio [OR]: 0.93; 95% confidence interval [CI]: 0.88-0.98, per 100 previous prostatectomies). PSMs were associated with increased risk of BCR (adjusted sub-distribution hazard ratio [sHR] 2.5; 95% CI 2.1-3.1) and second treatment (sHR 2.9; 95% CI 2.4-3.5). Risk of BCR was increased similarly for each PSM location, but was higher for multiple margin sites. We found no association between PSMs and PCSM. Conclusion: Our findings support previous research suggesting that PSMs are not independently associated with PCSM despite strong association with BCR. Reducing PSM rates remains an important objective, given the higher likelihood of secondary treatment with associated comorbidities.
|
|
Received: 28 May 2021
Available online: 20 October 2023
|
|
Corresponding Authors:
*Cancer Epidemiology and Population Health Research, University of South Australia, Adelaide, Australia. E-mail address: kerri.beckmann@unisa.edu.au (K.R. Beckmann).
|
|
|

| Characteristic | Margin status | Margin locationb | Multiplicity | | Negative | Positive | Apical | Bladder neck | Posterolateral | Single site | Multi-sites | | Total, n (%) | 2030 (72) | 797 (28) | 289 (10) | 172 (6) | 470 (17) | 652 (23) | 145 (5) | | NCCN risk category at Dx, n (%)c | | Low | 568 (78) | 159 (22) | 57 (8) | 30 (4) | 85 (8) | 142 (18) | 17 (2) | | Intermediate | 1232 (71) | 493 (29) | 189 (12) | 87 (5) | 314 (19) | 391 (24) | 102 (6) | | High | 230 (61) | 145 (39) | 43 (11) | 55 (15) | 71 (19) | 119 (32) | 26 (7) | | Gleason score at RP, n (%)c | | ≤6 | 502 (80) | 126 (20) | 52 (8) | 19 (3) | 60 (10) | 115 (18) | 11 (2) | | 3+4 | 932 (72) | 356 (28) | 133 (10) | 58 (5) | 215 (17) | 296 (23) | 60 (5) | | 4+3 | 416 (68) | 199 (32) | 61 (10) | 52 (8) | 127 (21) | 157 (26) | 42 (7) | | 8 | 103 (67) | 51 (33) | 19 (12) | 18 (12) | 31 (20) | 35 (23) | 16 (10) | | 9-10 | 70 (52) | 64 (48) | 24 (18) | 24 (18) | 37 (28) | 48 (36) | 16 (12) | | Missing | 7 | 1 | 0 | 0 | 0 | 1 | 0 | | Pathological stage, n (%)c | | pT2 | 1163 (82) | 257 (18) | 105 (7) | 38 (3) | 143 (10) | 223 (16) | 34 (2) | | pT3a | 743 (65) | 396 (35) | 130 (11) | 84 (7) | 241 (21) | 329 (29) | 67 (6) | | pT3b | 124 (46) | 144 (54) | 54 (20) | 50 (19) | 86 (32) | 100 (37) | 44 (16) | | Age at Dx, mean±SD, year | 62 ± 7 | 63 ± 7 | 63 ± 7 | 63 ± 6 | 62 ± 7 | 63 ± 7 | 63 ± 6 | | Pre-Rx PSA, median (IQR), ng/mL | 7 (5-9) | 8 (6-11) | 8 (6-12) | 9 (6-13) | 8 (6-11) | 8 (6-11) | 9 (6-13) | | Number of positive margin status core, median (IQR) | 3 (2-6) | 4 (2-7) | 5 (3-7) | 5 (3-7) | 4 (2-7) | 4 (2-6) | 5 (3-8) | | Tumour volume, median (IQR), cm3 | 2.3 (1.2-4.2) | 4.3 (2.3-8.3) | 4.6 (2.8-8.5) | 8.0 (3.3-12.7) | 4.0 (2.0-7.9) | 4.0 (2.2-7.7) | 7.6 (3.4-12.5) | | Nerve-sparing surgery, n (%)c | 1086 (53) | 420 (53) | 150 (10) | 71 (5) | 256 (17) | 354 (24) | 66 (4) |
|
|
Cohort profile by margin statusa.
|
| Factor | Any PSM | Apex | Bladder neck | Posterolateral | Multiple PSM sites | | OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | | Age at diagnosis, year | | <60 | 1.0 | Reference | 0.76 | 1.0 | Reference | 0.61 | 1.0 | Reference | 0.94 | 1.00 | Reference | 0.09 | 1.0 | Reference | 0.41 | | 60-69 | 0.9 | 0.8-1.1 | 0.46 | 1.1 | 0.8-1.4 | 0.59 | 0.9 | 0.6-1.4 | 0.72 | 0.8 | 0.6-1.0 | 0.08 | 0.9 | 0.6-1.4 | 0.63 | | 70-79 | 1.0 | 0.7-1.3 | 0.75 | 1.1 | 0.7-1.7 | 0.66 | 1.0 | 0.6-1.7 | 0.93 | 0.7 | 0.5-1.1 | 0.10 | 0.7 | 0.4-1.4 | 0.34 | | Treatment period | | ≤2007 | 1.0 | Reference | 0.17 | 1.0 | Reference | 0.22 | 1.0 | Reference | 0.002 | 1.0 | Reference | 0.020 | 1.0 | Reference | 0.97 | | 2008-2010 | 1.0 | 0.8-1.2 | 0.79 | 0.7 | 0.5-1.0 | 0.06 | 2.0 | 1.1-3.5 | 0.020 | 1.0 | 0.8-1.4 | 0.810 | 1.0 | 0.6-1.7 | 0.98 | | 2011-2013 | 0.6 | 0.5-0.8 | 0.01 | 0.7 | 0.4-1.1 | 0.10 | 2.6 | 1.4-4.8 | 0.003 | 0.5 | 0.3-0.7 | <0.001 | 0.6 | 0.3-1.1 | 0.09 | | 2014-2016 | 0.8 | 0.6-1.2 | 0.31 | 0.7 | 0.4-1.1 | 0.15 | 3.1 | 1.7-5.9 | 0.001 | 0.7 | 0.5-1.1 | 0.140 | 1.2 | 0.6-2.1 | 0.63 | | Pre-treatment PSA, ng/mL | | <5 | 1.0 | Reference | 0.39 | 1.0 | Reference | 0.20 | 1.0 | Reference | 0.89 | 1.0 | Reference | 0.78 | 1.0 | Reference | 0.73 | | ≥5-<10 | 0.9 | 0.7-1.2 | 0.63 | 1.1 | 0.7-1.5 | 0.79 | 0.6 | 0.4-0.9 | 0.02 | 1.0 | 0.7-1.3 | 0.86 | 0.7 | 0.4-1.1 | 0.14 | | ≥10-20 | 1.3 | 0.9-1.7 | 0.08 | 1.7 | 1.1-2.6 | 0.02 | 0.9 | 0.5-1.5 | 0.73 | 1.2 | 0.9-1.7 | 0.25 | 1.4 | 0.8-2.5 | 0.22 | | ≥20 | 1.3 | 0.8-2.3 | 0.31 | 1.4 | 0.8-2.3 | 0.19 | 1.2 | 0.5-2.6 | 0.68 | 0.9 | 0.5-1.7 | 0.67 | 1.2 | 0.5-2.9 | 0.74 | | RP Gleason score | | ≤6 | 1.0 | Reference | 0.08 | 1.0 | Reference | 0.35 | 1.0 | Reference | 0.03 | 1.0 | Reference | 0.010 | 1.0 | Reference | 0.010 | | 3+4 | 1.3 | 1.0-1.7 | 0.05 | 1.3 | 0.9-1.8 | 0.23 | 0.8 | 0.4-1.3 | 0.33 | 1.8 | 1.3-2.6 | <0.001 | 2.8 | 1.4-5.7 | 0.010 | | 4+3 | 1.4 | 1.0-1.9 | 0.05 | 1.0 | 0.7-1.6 | 0.83 | 1.2 | 0.6-2.2 | 0.63 | 2.1 | 1.4-3.1 | <0.001 | 3.6 | 1.7-7.6 | 0.001 | | 8 | 1.5 | 0.9-2.3 | 0.10 | 1.3 | 0.7-2.5 | 0.36 | 1.7 | 0.8-3.7 | 0.17 | 2.1 | 1.2-3.5 | 0.006 | 4.9 | 2.0-11.4 | <0.001 | | 9-10 | 1.7 | 1.0-2.7 | 0.02 | 1.6 | 0.8-2.9 | 0.16 | 1.4 | 0.7-3.1 | 0.35 | 2.2 | 1.3-3.9 | 0.003 | 3.4 | 1.4-8.5 | 0.010 | | pT | | 2 | 1.0 | Reference | <0.001 | 1.0 | Reference | 0.01 | 1.0 | Reference | <0.001 | 1.0 | Reference | <0.001 | 1.0 | Reference | <0.001 | | 3a | 2.3 | 1.9-2.8 | <0.001 | 1.4 | 1.0-1.9 | 0.03 | 1.9 | 1.2-3.0 | 0.004 | 2.5 | 2.0-3.2 | <0.001 | 2.1 | 1.3-3.4 | 0.001 | | 3b | 3.4 | 2.5-4.7 | <0.001 | 1.9 | 1.2-2.8 | 0.003 | 3.4 | 2.0-5.8 | <0.001 | 3.4 | 2.4-4.9 | <0.001 | 4.0 | 2.3-7.0 | <0.001 | | Tumour volume, per 10 cm3 | | Q1 (≤1.4) | 1.0 | Reference | <0.001 | 1.0 | Reference | <0.001 | 1.0 | Reference | <0.001 | 1.0 | Reference | <0.001 | 1.0 | Reference | <0.001 | | Q2 (>1.4-2.7) | 1.3 | 0.9-1.9 | 0.10 | 2.3 | 1.2-4.5 | 0.01 | 2.1 | 0.8-5.6 | 0.14 | 1.2 | 0.8-1.7 | 0.47 | 2.3 | 0.7-7.2 | 0.170 | | Q3 (>2.7-5.4) | 1.7 | 1.2-2.5 | <0.001 | 3.7 | 2.2-7.5 | <0.001 | 3.0 | 1.2-7.6 | 0.02 | 0.9 | 0.6-1.4 | 0.62 | 1.7 | 0.5-5.5 | 0.380 | | Q4 (>5.4) | 2.9 | 2.0-4.0 | <0.001 | 5.3 | 2.8-9.9 | <0.001 | 8.9 | 3.7-20.4 | <0.001 | 1.5 | 1.0-2.3 | 0.05 | 7.8 | 2.5-20.6 | <0.001 | | Surgeon volumea | 0.93 | 0.88-0.98 | 0.004 | 0.96 | 0.89-1.03 | 0.26 | 0.90 | 0.82-0.97 | 0.010 | 0.91 | 0.87-0.97 | 0.003 | 0.85 | 0.76-0.95 | 0.003 | | Nerve-sparing surgery | 0.9 | 0.7-1.2 | 0.45 | 1.1 | 0.7-1.5 | 0.78 | 0.7 | 0.4-1.0 | 0.070 | 0.9 | 0.6-1.1 | 0.32 | 0.7 | 0.4-1.1 | 0.110 |
|
|
Factors associated with any PSM, specific PSM sites, and multiple PSM sites derived from multivariable logistic regression models (1998-2016).
|

|
|
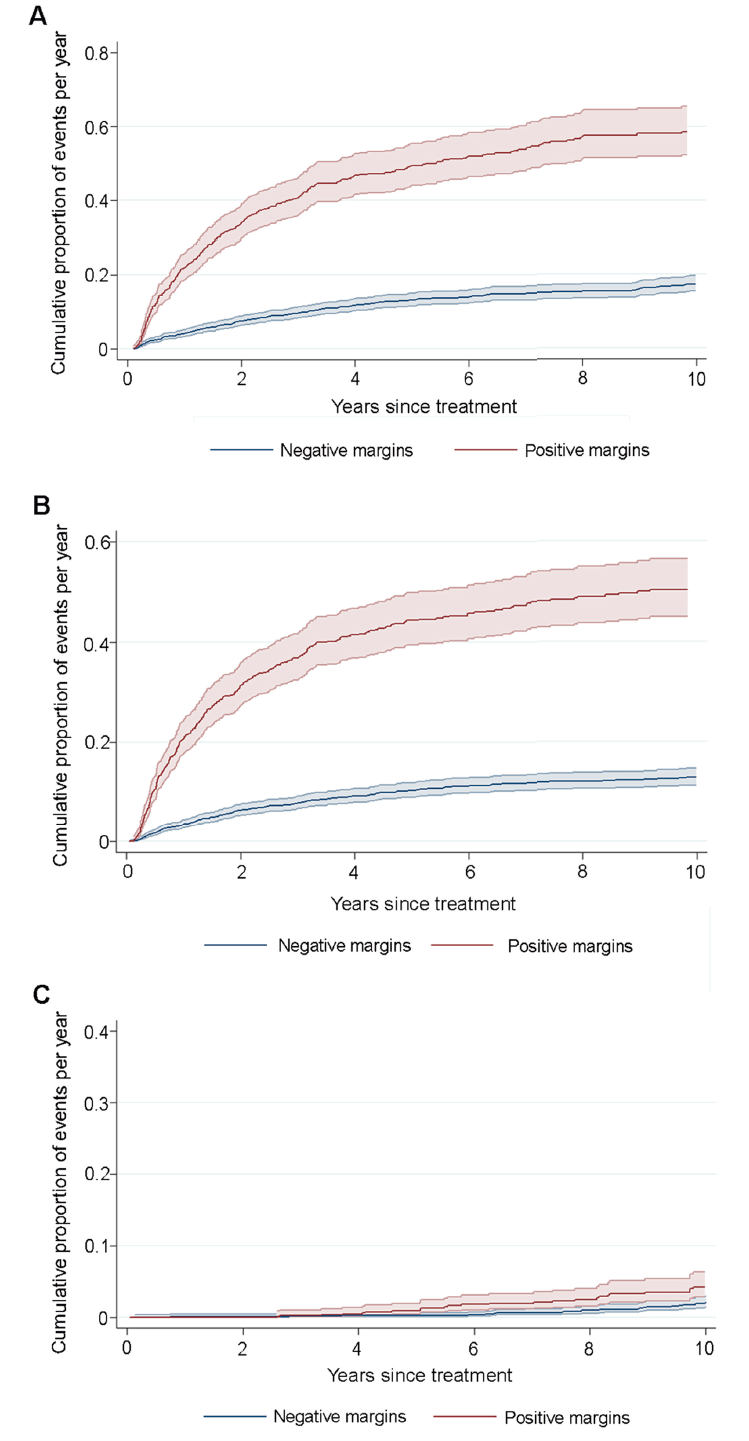
Cumulative incidence plots with 95% confidence intervals by surgical margin status (any positive vs. negative). (A) Cumulative incidence of biochemical recurrence; (B) Cumulative incidence of second treatment; (C) Cumulative incidence of prostate cancer death.
|
| Margin statusa | BCRb | Any secondary treatmentc | PCa deathd | | sHR | 95% CI | p-Value | sHR | 95% CI | p-Value | sHR | 95% CI | p-Value | | Any PSM vs. negative margin | 2.5 | 2.1-3.1 | <0.001 | 2.9 | 2.4-3.5 | <0.001 | 1.3 | 0.8-2.0 | 0.18 | | PSM at apex vs. all other casese | 1.7 | 1.3-2.2 | <0.001 | 2.0 | 1.6-2.5 | <0.001 | 1.3 | 0.7-2.4 | 0.39 | | PSM at bladder neck vs. all other casese | 1.9 | 1.4-2.5 | <0.001 | 1.8 | 1.3-2.5 | <0.001 | 1.7 | 0.9-3.5 | 0.11 | | PSM at posterolateral vs. all other casese | 2.1 | 1.7-2.5 | <0.001 | 2.3 | 1.9-2.8 | <0.001 | 0.9 | 0.6-1.6 | 0.83 | | Single PSM site vs. negative | 2.3 | 1.9-2.8 | <0.001 | 2.6 | 2.1-3.1 | <0.001 | 1.4 | 0.9-2.2 | 0.25 | | Multiple PSM sites vs. negative | 3.6 | 2.6-4.8 | <0.001 | 4.7 | 3.5-6.3 | <0.001 | 1.2 | 0.5-2.9 | 0.66 | | Intra-prostatic PSM vs. negativef | 4.5 | 3.2-6.3 | <0.001 | 4.8 | 3.3-7.0 | <0.001 | 0.8 | 0.3-2.2 | 0.59 |
|
|
Risk of BCR, second treatment, and PCa mortality, associated with any PSM, PSM site, and multiplicity of sites, derived from competing risk regression models.
|
| Margin status and pT | Relative to pT2 clear margin | PSM vs. clear margina | | sHR | 95% CI | p-Value | sHR | 95% CI | p-Value | | pT2 | | Clear margins | 1.0 | Reference | - | 1.0 | Reference | - | | Positive margin | 4.3 | 3.2-5.9 | <0.001 | 4.6 | 3.2-6.2 | <0.001 | | pT3a | | Clear margin | 2.2 | 1.7-2.9 | <0.001 | 1.0 | Reference | - | | Positive margin | 5.5 | 4.2-7.2 | <0.001 | 2.6 | 2.0-3.3 | <0.001 | | pT3b | | Clear margin | 4.9 | 3.4-7.0 | <0.001 | 1.0 | Reference | - | | Positive margin | 7.1 | 5.0-10.0 | <0.001 | 1.4 | 1.0-2.0 | 0.06 |
|
|
Risk of biochemical recurrence by margin status and pT derived from competing risk regression models.
|
| [1] |
Patel VR, Coelho RF, Rocco B, Orvieto M, Sivaraman A, Palmer KJ, et al. Positive surgical margins after robotic assisted radical prostatectomy: a multi-institutional study. J Urol 2011; 186:511-6.
doi: 10.1016/j.juro.2011.03.112
pmid: 21680001
|
| [2] |
Savdie R, Horvath LG, Benito RP, Rasiah KK, Haynes AM, Chatfield M, et al. High Gleason grade carcinoma at a positive surgical margin predicts biochemical failure after radical prostatectomy and may guide adjuvant radiotherapy. BJU Int 2012; 109:1794-800.
doi: 10.1111/j.1464-410X.2011.10572.x
pmid: 21992536
|
| [3] |
Shapiro EY, Scarberry K, Patel T, Bergman A, Ahn JJ, Sahi N, et al. Comparison of robot-assisted and open retropubic radical prostatectomy for risk of biochemical progression in men with positive surgical margins. J Endourol 2014; 28: 208-13.
doi: 10.1089/end.2013.0393
pmid: 24044423
|
| [4] |
Shikanov S, Song J, Royce C, Al-Ahmadie H, Zorn K, Steinberg G, et al. Length of positive surgical margin after radical prostatectomy as a predictor of biochemical recurrence. J Urol 2009; 182:139-44.
doi: 10.1016/j.juro.2009.02.139
pmid: 19450829
|
| [5] |
Smith JA Jr, Chan RC, Chang SS, Herrell SD, Clark PE, Baumgartner R, et al. A comparison of the incidence and location of positive surgical margins in robotic assisted laparoscopic radical prostatectomy and open retropubic radical prostatectomy. J Urol 2007; 178:2385-9.
pmid: 17936849
|
| [6] |
Tsivian M, Zilberman DE, Ferrandino MN, Madden JF, Mouraviev V, Albala DM. Apical surgical margins status in robot-assisted laparoscopic radical prostatectomy does not depend on disease characteristics. J Endourol 2012; 26:361-5.
doi: 10.1089/end.2011.0336
pmid: 22192106
|
| [7] |
Warner JN, Nunez RN, Mmeje CO, Colby TV, Ferrigni RG, Humphreys MR, et al. Impact of margin status at 37 months after robot assisted radical prostatectomy. Can J Urol 2011; 18:6043-9.
pmid: 22166333
|
| [8] |
Williams SB, D’Amico AV, Weinberg AC, Gu X, Lipsitz SR, Hu JC. Population-based determinants of radical prostatectomy surgical margin positivity. BJU Int 2011; 107:1734-40.
doi: 10.1111/j.1464-410X.2010.09662.x
pmid: 20942827
|
| [9] |
Tan PH, Cheng L, Srigley JR, Griffiths D, Humphrey PA, van der Kwast TH, et al. International Society of Urological Pathology (ISUP) consensus conference on handling and staging of radical prostatectomy specimens. Working group 5: surgical margins. Mod Pathol 2011; 24:48-57.
doi: 10.1038/modpathol.2010.155
|
| [10] |
Evans SM, Millar JL, Frydenberg M, Murphy DG, Davis ID, Spelman T, et al. Positive surgical margins: rate, contributing factors and impact on further treatment: findings from the Prostate Cancer Registry. BJU Int 2014; 114:680-90.
doi: 10.1111/bju.12509
pmid: 24128010
|
| [11] |
Yossepowitch O, Briganti A, Eastham JA, Epstein J, Graefen M, Montironi R, et al. Positive surgical margins after radical prostatectomy: a systematic review and contemporary update. Eur Urol 2014; 65:303-13.
doi: 10.1016/j.eururo.2013.07.039
pmid: 23932439
|
| [12] |
Retel VP, Bouchardy C, Usel M, Neyroud-Caspar I, Schmidlin F, Wirth G, et al. Determinants and effects of positive surgical margins after prostatectomy on prostate cancer mortality: a population-based study. BMC Urol 2014; 14:86. https://doi.org/10.1186/1471-2490-14-86.
doi: 10.1186/1471-2490-14-86
pmid: 25374000
|
| [13] |
Alkhateeb S, Alibhai S, Fleshner N, Finelli A, Jewett M, Zlotta A, et al. Impact of positive surgical margins after radical prostatectomy differs by disease risk group. J Urol 2010; 183:145-50.
doi: 10.1016/j.juro.2009.08.132
pmid: 19913824
|
| [14] |
Tuliao PH, Koo KC, Komninos C, Chang CH, Choi YD, Chung BH, et al. Number of positive preoperative biopsy cores is a predictor of positive surgical margins (PSM) in small prostates after robot-assisted radical prostatectomy (RARP). BJU Int 2015; 116:897-904.
doi: 10.1111/bju.12888
pmid: 25098818
|
| [15] |
Thompson JE, Egger S, Bohm M, Haynes AM, Matthews J, Rasiah K, et al. Superior quality of life and improved surgical margins are achievable with robotic radical prostatectomy after a long learning curve: a prospective single-surgeon study of 1552 consecutive cases. Eur Urol 2014; 65:521-31.
doi: 10.1016/j.eururo.2013.10.030
pmid: 24287319
|
| [16] |
Vickers A, Bianco F, Cronin A, Eastham J, Klein E, Kattan M, et al. The learning curve for surgical margins after open radical prostatectomy: implications for margin status as an oncological end point. J Urol 2010; 183:1360-5.
doi: 10.1016/j.juro.2009.12.015
pmid: 20171687
|
| [17] |
Vickers AJ, Bianco FJ, Gonen M, Cronin AM, Eastham JA, Schrag D, et al. Effects of pathologic stage on the learning curve for radical prostatectomy: evidence that recurrence in organ-confined cancer is largely related to inadequate surgical technique. Eur Urol 2008; 53:960-6.
doi: 10.1016/j.eururo.2008.01.005
pmid: 18207316
|
| [18] |
Lightfoot AJ, Su YK, Sehgal SS, Lee Z, Greaves GH, Yu SJ, et al. Positive surgical margin trends in patients with pathologic T3 prostate cancer treated with robot-assisted radical prostatectomy. J Endourol 2015; 29:634-9.
doi: 10.1089/end.2014.0242
pmid: 25506629
|
| [19] |
Trinh QD, Bjartell A, Freedland SJ, Hollenbeck BK, Hu JC, Shariat SF, et al. A systematic review of the volume-outcome relationship for radical prostatectomy. Eur Urol 2013; 64: 786-98.
doi: 10.1016/j.eururo.2013.04.012
|
| [20] |
Schiavina R, Chessa F, Borghesi M, Gaudiano C, Bianchi L, Corcioni B, et al. State-of-the-art imaging techniques in the management of preoperative staging and re-staging of prostate cancer. Int J Urol 2019; 26:18-30.
doi: 10.1111/iju.13797
pmid: 30238516
|
| [21] |
Shin T, Ukimura O, Gill IS. Three-dimensional printed model of prostate anatomy and targeted biopsy-proven index tumor to facilitate nerve-sparing prostatectomy. Eur Urol 2016; 69: 377-9.
doi: 10.1016/j.eururo.2015.09.024
pmid: 26431913
|
| [22] |
Dinneen EP, Van Der Slot M, Adasonla K, Tan J, Grierson J, Haider A, et al. Intraoperative frozen section for margin evaluation during radical prostatectomy: a systematic review. Eur Urol Focus 2020; 6:664-73.
|
| [23] |
Thompson IM, Valicenti RK, Albertsen P, Davis BJ, Goldenberg SL, Hahn C, et al. Adjuvant and salvage radiotherapy after prostatectomy: AUA/ASTRO guideline. J Urol 2013; 190:441-9.
doi: 10.1016/j.juro.2013.05.032
pmid: 23707439
|
| [24] |
Pfitzenmaier J, Pahernik S, Tremmel T, Haferkamp A, Buse S, Hohenfellner M. Positive surgical margins after radical prostatectomy: do they have an impact on biochemical or clinical progression? BJU Int 2008; 102:1413-8.
doi: 10.1111/j.1464-410X.2008.07791.x
pmid: 18537951
|
| [25] |
Wright JL, Dalkin BL, True LD, Ellis WJ, Stanford JL, Lange PH, et al. Positive surgical margins at radical prostatectomy predict prostate cancer specific mortality. J Urol 2010; 183: 2213-8.
doi: 10.1016/j.juro.2010.02.017
pmid: 20399459
|
| [26] |
Chalfin HJ, Dinizo M, Trock BJ, Feng Z, Partin AW, Walsh PC, et al. Impact of surgical margin status on prostate-cancerspecific mortality. BJU Int 2012; 110:1684-9.
doi: 10.1111/bju.2012.110.issue-11
|
| [27] |
Stephenson AJ, Kattan MW, Eastham JA, Dotan ZA, Bianco Jr FJ, Lilja H, et al. Defining biochemical recurrence of prostate cancer after radical prostatectomy: a proposal for a standardized definition. J Clin Oncol 2006; 24:3973-8.
doi: 10.1200/JCO.2005.04.0756
pmid: 16921049
|
| [28] |
Chen ME, Johnston D, Reyes AO, Soto CP, Babaian RJ, Troncoso P. A streamlined three-dimensional volume estimation method accurately classifies prostate tumors by volume. Am J Surg Pathol 2003; 27:1291-301.
doi: 10.1097/00000478-200310000-00001
pmid: 14508390
|
| [29] |
Fine J, Gray R. A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc 1999; 94: 496-509.
doi: 10.1080/01621459.1999.10474144
|
| [30] |
Tatsugami K, Yoshioka K, Shiroki R, Eto M, Yoshino Y, Tozawa K, et al. Reality of nerve sparing and surgical margins in surgeons’ early experience with robot-assisted radical prostatectomy in Japan. Int J Urol 2017; 24:191-6.
doi: 10.1111/iju.2017.24.issue-3
|
| [31] |
Doumerc N, Yuen C, Savdie R, Rahman MB, Rasiah KK, Pe Benito R, et al. Should experienced open prostatic surgeons convert to robotic surgery? The real learning curve for one surgeon over 3 years. BJU Int 2010; 106:378-84.
doi: 10.1111/j.1464-410X.2009.09158.x
pmid: 20067454
|
| [32] |
Bellangino M, Verrill C, Leslie T, Bell RW, Hamdy FC, Lamb AD. Systematic review of studies reporting positive surgical margins after bladder neck sparing radical prostatectomy. Curr Urol Rep 2017; 18:99. https://doi.org/10.1007/s11934-017-0745-0.
doi: 10.1007/s11934-017-0745-0
pmid: 29116405
|
| [33] |
Wang Y, Gao X, Yang Q, Wang H, Shi T, Chang Y, et al. Threedimensional printing technique assisted cognitive fusion in targeted prostate biopsy. Asian J Urol 2015; 2:214-9.
doi: 10.1016/j.ajur.2015.09.002
pmid: 29264148
|
| [34] |
Schlomm T, Tennstedt P, Huxhold C, Steuber T, Salomon G, Michl U, et al. Neurovascular structure-adjacent frozen-section examination (NeuroSAFE) increases nerve-sparing frequency and reduces positive surgical margins in open and robot-assisted laparoscopic radical prostatectomy: experience after 11 069 consecutive patients. Eur Urol 2012; 62: 333-40.
doi: 10.1016/j.eururo.2012.04.057
|
| [35] |
Dev HS, Wiklund P, Patel V, Parashar D, Palmer K, Nyberg T, et al. Surgical margin length and location affect recurrence rates after robotic prostatectomy. Urol Oncol 2015; 33: 109.e7-13. https://doi.org/10.1016/j.urolonc.2014.11.005.
doi: 10.1016/j.urolonc.2014.11.005
|
| [36] |
Ploussard G, Drouin SJ, Rode J, Allory Y, Vordos D, Hoznek A, et al. Location, extent, and multifocality of positive surgical margins for biochemical recurrence prediction after radical prostatectomy. World J Urol 2014; 32:1393-400.
doi: 10.1007/s00345-014-1243-3
pmid: 24445447
|
| [37] |
O’Neil LM, Walsh S, Cohen RJ, Lee S. Prostate carcinoma with positive margins at radical prostatectomy: role of tumour zonal origin in biochemical recurrence. BJU Int 2015; 116: 42-8.
doi: 10.1111/bju.2015.116.issue-S3
|
| [38] |
Roder MA, Kawa S, Scheike T, Toft BG, Hansen JB, Brasso K, et al. Non-apical positive surgical margins after radical prostatectomy for pT2 prostate cancer is associated with the highest risk of recurrence. J Surg Oncol 2014; 109:818-22.
doi: 10.1002/jso.23573
pmid: 24522971
|
| [39] |
Lake AM, He C, Wood DP Jr. Focal positive surgical margins decrease disease-free survival after radical prostatectomy even in organ-confined disease. Urology 2010; 76:1212-6.
doi: 10.1016/j.urology.2009.08.088
pmid: 20110115
|
| [40] |
Pettenati C, Neuzillet Y, Radulescu C, Herve JM, Molinie V, Lebret T. Positive surgical margins after radical prostatectomy: what should we care about? World J Urol 2015; 33. 1973-8.
doi: 10.1007/s00345-015-1580-x
pmid: 25939539
|
| [41] |
Servoll E, Vlatkovic L, Saeter T, Nesland JM, Axcrona U, Waaler G, et al. The length of a positive surgical margin is of prognostic significance in patients with clinically localized prostate cancer treated with radical prostatectomy. Urol Int 2014; 93:289-95.
doi: 10.1159/000362342
pmid: 25170745
|
| [42] |
Stephenson AJ, Wood DP, Kattan MW, Klein EA, Scardino PT, Eastham JA, et al. Location, extent and number of positive surgical margins do not improve accuracy of predicting prostate cancer recurrence after radical prostatectomy. J Urol 2009; 182:1357-63.
doi: 10.1016/j.juro.2009.06.046
pmid: 19683274
|
| [43] |
Huang JG, Pedersen J, Hong MK, Harewood LM, Peters J, Costello AJ, et al. Presence or absence of a positive pathological margin outperforms any other margin-associated variable in predicting clinically relevant biochemical recurrence in Gleason 7 prostate cancer. BJU Int 2013; 111:921-7.
doi: 10.1111/j.1464-410X.2012.11665.x
pmid: 23350712
|
| [44] |
Rouanne M, Rode J, Campeggi A, Allory Y, Vordos D, Hoznek A, et al. Long-term impact of positive surgical margins on biochemical recurrence after radical prostatectomy: ten years of follow-up. Scand J Urol 2014; 48:131-7.
doi: 10.3109/21681805.2013.813067
pmid: 23883410
|
| [45] |
Boorjian SA, Karnes RJ, Crispen PL, Carlson RE, Rangel LJ, Bergstralh EJ, et al. The impact of positive surgical margins on mortality following radical prostatectomy during the prostate specific antigen era. J Urol 2010; 183:1003-9.
doi: 10.1016/j.juro.2009.11.039
pmid: 20092854
|
| [46] |
Mauermann J, Fradet V, Lacombe L, Dujardin T, Tiguert R, Tetu B, et al. The impact of solitary and multiple positive surgical margins on hard clinical end points in 1712 adjuvant treatment-naive pT2-4 N0 radical prostatectomy patients. Eur Urol 2013; 64:19-25.
doi: 10.1016/j.eururo.2012.08.002
pmid: 22901983
|
| [47] |
Izard JP, True LD, May P, Ellis WJ, Lange PH, Dalkin B, et al. Prostate cancer that is within 0.1 mm of the surgical margin of a radical prostatectomy predicts greater likelihood of recurrence. Am J Surg Pathol 2014; 38:333-8.
doi: 10.1097/PAS.0000000000000162
pmid: 24525503
|
| [48] |
Lu J, Wirth GJ, Wu S, Chen J, Dahl DM, Olumi AF, et al. A close surgical margin after radical prostatectomy is an independent predictor of recurrence. J Urol 2012; 188:91-7.
doi: 10.1016/j.juro.2012.02.2565
pmid: 22578729
|
| [49] |
Tallman JE, Packiam VT, Wroblewski KE, Paner GP, Eggener SE. Influence of pathologist experience on positive surgical margins following radical prostatectomy. Urol Oncol 2017; 35:461.e1-6. https://doi.org/10.1016/j.urolonc.2017.02.007.
doi: 10.1016/j.urolonc.2017.02.007
|
| [50] |
Meeks JJ, Eastham JA. Radical prostatectomy: positive surgical margins matter. Urol Oncol 2013; 31:974-9.
doi: 10.1016/j.urolonc.2011.12.011
pmid: 22244265
|
| [51] |
Mauermann J, Fradet V, Fradet Y. Reply from authors re: Martin Spahn, Steven Joniau. Positive surgical margin at radical prostatectomy: futile or surgeon-dependent predictor of prostate cancer death? Eur Urol 2013; 64:26-8: adjuvant versus salvage radiotherapy in patients with positive surgical margins at radical prostatectomy: that is the question. Eur Urol 2013;64:28e9.
doi: 10.1016/j.eururo.2012.08.063
pmid: 22999520
|
| [52] |
Damani A, Van Hemelrijck M, Wulaningsih W, Crawley D, Cahill D. Are you now a good surgeon? T2 positive margin status as a quality outcome measure following radical prostatectomy. World J Urol 2017; 35:35-43.
doi: 10.1007/s00345-016-1836-0
pmid: 27112152
|
| [1] |
Enrico Checcucci, Alberto Piana, Gabriele Volpi, Pietro Piazzolla, Daniele Amparore, Sabrina De Cillis, Federico Piramide, Cecilia Gatti, Ilaria Stura, Enrico Bollito, Federica Massa, Michele Di Dio, Cristian Fiori, Francesco Porpiglia. Three-dimensional automatic artificial intelligence driven augmented-reality selective biopsy during nerve-sparing robot-assisted radical prostatectomy: A feasibility and accuracy study[J]. Asian Journal of Urology, 2023, 10(4): 407-415. |
| [2] |
Roxana Ramos-Carpinteyro, Ethan L. Ferguson, Jaya S. Chavali, Albert Geskin, Jihad Kaouk. First 100 cases of transvesical single-port robotic radical prostatectomy[J]. Asian Journal of Urology, 2023, 10(4): 416-422. |
| [3] |
Umberto Carbonara, Giuseppe Lippolis, Luciano Rella, Paolo Minafra, Giuseppe Guglielmi, Antonio Vitarelli, Giuseppe Lucarelli, Pasquale Ditonno. Intermediate-term oncological and functional outcomes in prostate cancer patients treated with perineal robot-assisted radical prostatectomy: A single center analysis[J]. Asian Journal of Urology, 2023, 10(4): 423-430. |
| [4] |
Jordan M. Rich, Shivaram Cumarasamy, Daniel Ranti, Etienne Lavallee, Kyrollis Attalla, John P. Sfakianos, Nikhil Waingankar, Peter N. Wiklund, Reza Mehrazin. Contemporary outcomes of patients undergoing robotic-assisted radical cystectomy: A comparative analysis between intracorporeal ileal conduit and neobladder urinary diversions[J]. Asian Journal of Urology, 2023, 10(4): 446-452. |
| [5] |
Brianna Ruch, Deki Tsering, Chandra Bhati, Dhiren Kumar, Muhammad Saeed, Seung Duk Lee, Aamir Khan, Daisuke Imai, David Bruno, Marlon Levy, Adrian Cotterell, Amit Sharma. Right versus left fully robotic live donor nephrectomy and open kidney transplantation: Does the laterality of the donor kidney really matter?[J]. Asian Journal of Urology, 2023, 10(4): 453-460. |
| [6] |
Angelo Territo, Alessandro Uleri, Andrea Gallioli, Josep Maria Gaya, Paolo Verri, Giuseppe Basile, Alba Farré, Alejandra Bravo, Alessandro Tedde, Óscar Rodríguez Faba, Joan Palou, Alberto Breda. Robot-assisted oncologic pelvic surgery with Hugo™ robot-assisted surgery system: A single-center experience[J]. Asian Journal of Urology, 2023, 10(4): 461-466. |
| [7] |
Thomas Whish-Wilson, Jo-Lynn Tan, William Cross, Lih-Ming Wong, Tom Sutherland. Prostate magnetic resonance imaging and the value of experience: An intrareader variability study[J]. Asian Journal of Urology, 2023, 10(4): 488-493. |
| [8] |
Thitipat Hansomwong, Pat Saksirisampant, Sudhir Isharwal, Pubordee Aussavavirojekul, Varat Woranisarakul, Siros Jitpraphai, Sunai Leewansangtong, Tawatchai Taweemonkongsap, Sittiporn Srinualnad. Role of preoperative magnetic resonance imaging on the surgical outcomes of radical prostatectomy: Does preoperative tumor recognition reduce the positive surgical margin in a specific location? Experience from a Thailand prostate cancer specialized center[J]. Asian Journal of Urology, 2023, 10(4): 494-501. |
| [9] |
Wei He,Yutian Xiao,Shi Yan,Yasheng Zhu,Shancheng Ren. Cell-free DNA in the management of prostate cancer: Current status and future prospective[J]. Asian Journal of Urology, 2023, 10(3): 298-316. |
| [10] |
Shulin Wu,Sharron X. Lin,Kristine M. Cornejo,Rory K. Crotty,Michael L. Blute,Douglas M. Dahl,Chin-Lee Wu. Clinicopathological and oncological significance of persistent prostate-specific antigen after radical prostatectomy: A systematic review and meta-analysis[J]. Asian Journal of Urology, 2023, 10(3): 317-328. |
| [11] |
Stefano Alba,Deborah Fimognari,Fabio Crocerossa,Luigi Ascalone,Carmine Pullano,Fernando Chiaravalloti,Francesco Chiaradia,Umberto Carbonara,Matteo Ferro,Ottavio de Cobelli,Vincenzo Pagliarulo,Giuseppe Lucarelli,Michele Battaglia,Rocco Damiano,Francesco Cantiello. Neuraxial anesthesia versus general anesthesia in patients undergoing three-dimensional laparoscopic radical prostatectomy: Preliminary results of a prospective comparative study[J]. Asian Journal of Urology, 2023, 10(3): 329-336. |
| [12] |
Fabricio B. Carrerette,Daniela B. Rodeiro,Rui T. F. Filho,Paulo A. Santos,Celso C. Lara,Ronaldo Damião. Randomized controlled trial comparing open anterograde anatomic radical retropubic prostatectomy with retrograde technique[J]. Asian Journal of Urology, 2023, 10(2): 151-157. |
| [13] |
Sat Prasad Nepal,Takehiko Nakasato,Takashi Fukagai,Yoshio Ogawa,Yoshihiro Nakagami,Takeshi Shichijo,Jun Morita,Yoshiko Maeda,Kazuhiko Oshinomi,Tsutomu Unoki,Tetsuo Noguchi,Tatsuki Inoue,Ryosuke Kato,Satoshi Amano,Moyuru Mizunuma,Masahiro Kurokawa,Yoshiki Tsunokawa,Sou Yasuda. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios alone or combined with prostate-specific antigen for the diagnosis of prostate cancer and clinically significant prostate cancer[J]. Asian Journal of Urology, 2023, 10(2): 158-165. |
| [14] |
Hua Gong,Kang Chen,Lan Zhou,Yongchao Jin,Weihua Chen. Deleted in liver cancer 1 suppresses the growth of prostate cancer cells through inhibiting Rho-associated protein kinase pathway[J]. Asian Journal of Urology, 2023, 10(1): 50-57. |
| [15] |
Leandro Blas,Masaki Shiota,Shohei Nagakawa,Shigehiro Tsukahara,Takashi Matsumoto,Ken Lee,Keisuke Monji,Eiji Kashiwagi,Junichi Inokuchi,Masatoshi Eto. Validation of user-friendly models predicting extracapsular extension in prostate cancer patients[J]. Asian Journal of Urology, 2023, 10(1): 81-88. |
|
|
|
|