aInstitute for Urology and Reproductive Health, Sechenov University, Moscow, Russia bYoung Academic Urologists, EAU, the Netherlands cDepartment of Urology, James Buchanan Brady Urological Institute, The Johns Hopkins University School of Medicine, Baltimore, USA dDepartment of Urology, Institut Mutualiste Montsouris, Paris, France eSechenov University, Moscow, Russia;f Hertsen Moscow Oncology Research Institute, Moscow, Russia fHertsen Moscow Oncology Research Institute, Moscow, Russia gMartini Clinic, University Medical Center Hamburg-Eppendorf, Hamburg, Germany hDepartment of Urology, Clinico San Carlos University Hospital, Madrid, Spain iDepartment of Urology, Medical University of Vienna, Vienna, Austria
Objective: To analyze outcomes and complications of cytoreductive prostatectomy (CRP) for oligometastatic prostate cancer (PCa) in order to elucidate its role in this space.
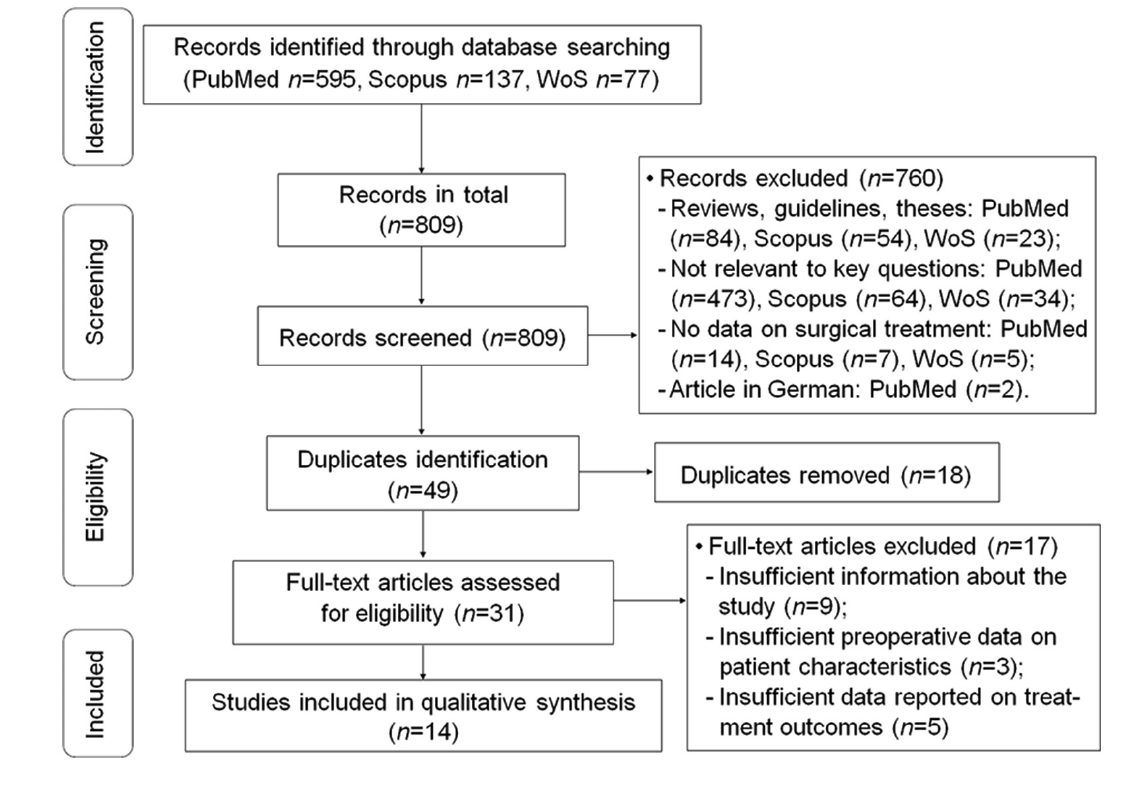
Methods: We performed a systematic literature search using three databases (Medline, Scopus, and Web of Science). The primary endpoints were oncologic outcomes. The secondary endpoints were complication rates and functional results.
Results: In all studies, overall survival was better or at least comparable variable in the groups with CRP compared to no local treatment. The greatest benefit from CRP in 5-year overall survival in one study was 67.4% for CRP versus 22.5% for no local treatment. Cancer-specific survival (CSS) showed the same trend. Several authors found significant benefits from CSS in the CRP group: from 79% vs. 46% to 100% vs. 61%. CRP was a predictor of better CSS (hazard ratio 0.264, p=0.004). Positive surgical margin rates differed widely from 28.6% to 100.0%. Urinary continence in CRP versus RP for localized PCa was significantly lower (57.4% vs. 90.8%, p<0.0001). Severe incontinence occurred seldom (2.5%-18.6%). Total complication rates after CRP differed widely, from 7.0% to 43.6%. Rates of grades 1 and 2 events prevailed. Patients on ADT alone also showed a considerable number of complications varying from 5.9% to 57.7%.
Conclusion: CRP improves medium-term cancer control in patients with oligometastatic PCa. The morbidity and complication rates of this surgery are comparable with other approaches, but postoperative incontinence rate is higher compared with RP for localized disease.
. [J]. Asian Journal of Urology, 2024, 11(2): 208-220.
Andrey Morozov, Leonid Chuvalov, Mark Taratkin, Mikhail Enikeev, Leonid Rapoport, Nirmish Singla, Eric Barret, Elena Poddubskaya, Maria Borodina, Georg Salomon, Juan Gomez Rivas, Dmitry Enikeev. A systematic review of cytoreductive prostatectomy outcomes and complications in oligometastatic disease. Asian Journal of Urology, 2024, 11(2): 208-220.
Wang G, Zhao D, Spring DJ, DePinho RA. Genetics and biology of prostate cancer. Genes Dev 2018; 32:1105e40.
doi: 10.1101/gad.315739.118
[2]
James ND, Spears MR, Clarke NW, Dearnaley DP, De Bono JS, Gale J, et al. Survival with newly diagnosed metastatic prostate cancer in the “docetaxel era”: data from 917 patients in the control arm of the STAMPEDE trial (MRC PR08, CRUK/06/019). Eur Urol 2015; 67:1028e38.
doi: 10.1016/j.eururo.2014.09.032
[3]
Kyriakopoulos CE, Chen YH, Carducci MA, Liu G, Jarrard DF, Hahn NM, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer: long-term survival analysis of the randomized phase III E3805 CHAARTED trial. J Clin Oncol 2018; 36:1080e7.
doi: 10.1200/JCO.2017.75.3657
pmid: 29384722
[4]
Gómez Rivas J, Carrion DM, Alvarez-Maestro M, Cathelineau X, Sanchez-Salas R, Di Lorenzo G, et al. Bone-targeted therapy in castration-resistant prostate cancer: where do we stand? Minerva Urol Nefrol 2019; 71:445e56.
doi: 10.23736/S0393-2249.19.03420-9
pmid: 31353876
[5]
Hong MK, Kong J, Namdarian B, Longano A, Grummet J, Hovens CM, et al. Paraneoplastic syndromes in prostate cancer. Nat Rev Urol 2010; 7:681e92.
doi: 10.1038/nrurol.2010.186
pmid: 21139643
Chambers AF, Groom AC, MacDonald IC. Dissemination and growth of cancer cells in metastatic sites. Nat Rev Cancer 2002; 2:563e72.
doi: 10.1038/nrc865
pmid: 12154349
Pagliarulo V, Bracarda S, Eisenberger MA, Mottet N, Schr?der FH, Sternberg CN, et al. Contemporary role of androgen deprivation therapy for prostate cancer. Eur Urol 2012; 61:11e25.
[11]
Aus G, Hugosson J, Norlén L. Need for hospital care and palliative treatment for prostate cancer treated with noncurative intent. J Urol 1995; 154:466e9.
doi: 10.1097/00005392-199508000-00034
pmid: 7541865
[12]
Won ACM, Gurney H, Marx G, De Souza P, Patel MI. Primary treatment of the prostate improves local palliation in men who ultimately develop castrate-resistant prostate cancer. BJU Int 2013; 112:E250e5. https://doi.org/10.1111/bju.12169.
[13]
Antonarakis ES, Lu C, Wang H, Luber B, Nakazawa M, Roeser JC, et al. AR-V7 and resistance to enzalutamide and abiraterone in prostate cancer. N Engl J Med 2014; 371:1028e38.
doi: 10.1056/NEJMoa1315815
Parker CC, James ND, Brawley CD, Clarke NW, Hoyle AP, Ali A, et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): a randomised controlled phase 3 trial. Lancet 2018; 392: 2353e66.
doi: S0140-6736(18)32486-3
pmid: 30355464
[16]
Glehen O, Mohamed F, Gilly FN. Peritoneal carcinomatosis from digestive tract cancer: new management by cytoreductive surgery and intraperitoneal chemohyperthermia. Lancet Oncol 2004; 5:219e28.
doi: 10.1016/S1470-2045(04)01425-1
pmid: 15050953
[17]
Roviello F, Caruso S, Marrelli D, Pedrazzani C, Neri A, De Stefano A, et al. Treatment of peritoneal carcinomatosis with cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. G Chir 2011; 32:211e33.
[18]
Heng DYC, Wells JC, Rini BI, Beuselinck B, Lee JL, Knox JJ, et al. Cytoreductive nephrectomy in patients with synchronous metastases from renal cell carcinoma: results from the International Metastatic Renal Cell Carcinoma Database Consortium. Eur Urol 2014; 66:704e10.
doi: 10.1016/j.eururo.2014.05.034
pmid: 24931622
[19]
Choueiri TK, Xie W, Kollmannsberger C, North S, Knox JJ, Lampard JG, et al. The impact of cytoreductive nephrectomy on survival of patients with metastatic renal cell carcinoma receiving vascular endothelial growth factor targeted therapy. J Urol 2011; 185:60e6.
doi: 10.1016/j.juro.2010.09.012
pmid: 21074201
[20]
Swanson G, Thompson I, Basler J, Crawford D. Metastatic prostate cancerddoes treatment of the primary tumor matter? J Urol 2006; 176:1292e8.
doi: 10.1016/j.juro.2006.06.069
[21]
Wells GA, Shea B, O’Connell D. The Newcastle Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses. Available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. [Accessed 06 August 2021].
[22]
Phillips B, Ball C, Sackett D, Badenoch D, Straus S, Haynes B, et al. Levels of evidence. Oxford Centre for evidence-based medicine. Available from: https://www.cebm.net/2009/06/oxford-centre-evidence-based-medicine-levels-evidencemarch-2009/. [Accessed 20 August 2020].
[23]
Jang WS, Kim MS, Jeong WS, Chang KD, Cho KS, Ham WS, et al. Does robot-assisted radical prostatectomy benefit patients with prostate cancer and bone oligometastases? BJU Int 2018; 121:225e31.
doi: 10.1111/bju.13992
pmid: 28834084
[24]
Leyh-Bannurah SR, Gazdovich S, Bud?us L, Zaffuto E, Briganti A, Abdollah F, et al. Local therapy improves survival in metastatic prostate cancer. Eur Urol 2017; 72:118e24.
doi: S0302-2838(17)30231-2
pmid: 28385454
[25]
Steuber T, Berg KD, R?der MA, Brasso K, Iversen P, Huland H, et al. Does cytoreductive prostatectomy really have an impact on prognosis in prostate cancer patients with low-volume bone metastasis? Results from a prospective case-control study. Eur Urol Focus 2017; 3:646e9.
doi: S2405-4569(17)30171-2
pmid: 28753877
[26]
Yuh BE, Kwon YS, Shinder BM, Singer EA, Jang TL, Kim S, et al. Results of Phase 1 study on cytoreductive radical prostatectomy in men with newly diagnosed metastatic prostate cancer. Prostate Int 2019; 7:102e7.
doi: 10.1016/j.prnil.2018.10.002
[27]
Lan T, Chen Y, Su QJ, Ye JJ. Oncological outcome of cytoreductive radical prostatectomy in prostate cancer patients with bone oligometastases. Urology 2019; 131:166e75.
doi: S0090-4295(19)30507-2
pmid: 31181273
[28]
Simforoosh N, Dadpour M, Mofid B. Cytoreductive and palliative radical prostatectomy, extended lymphadenectomy and bilateral orchiectomy in advanced prostate cancer with oligo and widespread bone metastases: result of a feasibility, our initial experience. Urol J 2019; 16:162e7.
doi: 10.22037/uj.v0i0.4783
pmid: 30393838
[29]
Kim DK, Parihar JS, Kwon YS, Kim S, Shinder B, Lee N, et al. Risk of complications and urinary incontinence following cytoreductive prostatectomy: a multi-institutional study. Asian J Androl 2018; 20:9e14.
doi: 10.4103/1008-682X.196852
pmid: 28440262
[30]
Satkunasivam R, Kim AE, Desai M, Nguyen MM, Quinn DI, Ballas L, et al. Radical prostatectomy or external beam radiation therapy vs. no local therapy for survival benefit in metastatic prostate cancer: a SEER-medicare analysis. J Urol 2015; 194:378e85.
doi: 10.1016/j.juro.2015.02.084
pmid: 25711194
[31]
Sooriakumaran P, Karnes J, Stief C, Copsey B, Montorsi F, Hammerer P, et al. A multi-institutional analysis of perioperative outcomes in 106 men who underwent radical prostatectomy for distant metastatic prostate cancer at presentation. Eur Urol 2016; 69:788e94.
doi: 10.1016/j.eururo.2015.05.023
pmid: 26038098
[32]
Heidenreich A, Pfister D, Porres D. Cytoreductive radical prostatectomy in patients with prostate cancer and low volume skeletal metastases: results of a feasibility and casecontrol study. J Urol 2015; 193:832e8.
doi: 10.1016/j.juro.2014.09.089
pmid: 25254935
[33]
Heidenreich A, Fossati N, Pfister D, Suardi N, Montorsi F, Shariat S, et al. Cytoreductive radical prostatectomy in men with prostate cancer and skeletal metastases. Eur Urol Oncol 2018; 1:46e53.
doi: S2588-9311(18)30006-3
pmid: 31100228
[34]
Culp SH, Schellhammer PF, Williams MB. Might men diagnosed with metastatic prostate cancer benefit from definitive treatment of the primary tumor? A SEER-based study. Eur Urol 2014; 65:1058e66.
doi: 10.1016/j.eururo.2013.11.012
pmid: 24290503
[35]
Poelaert F, Verbaeys C, Rappe B, Kimpe B, Billiet I, Plancke H, et al. Cytoreductive prostatectomy for metastatic prostate cancer: first lessons learned from the multicentric prospective local treatment of metastatic prostate cancer (LoMP) trial. Urology 2017; 106:146e52.
doi: S0090-4295(17)30372-2
pmid: 28435034
[36]
Knipper S, Beyer B, Mandel P, Tennstedt P, Tilki D, Steuber T, et al. Outcome of patients with newly diagnosed prostate cancer with low metastatic burden treated with radical prostatectomy: a comparison to STAMPEDE arm H. World J Urol 2020; 38:1459e64.
doi: 10.1007/s00345-019-02950-0
pmid: 31511970
[37]
Fidler IJ. The pathogenesis of cancer metastasis: the “seed and soil” hypothesis revisited. Nat Rev Cancer 2003; 3:453e8.
doi: 10.1038/nrc1098
[38]
Kendal WS. Oligometastasis as a predictor for occult disease. Math Biosci 2014; 251:1e10.
doi: 10.1016/j.mbs.2014.02.006
pmid: 24560886
[39]
Zhang L, Wu B, Zha Z, Zhao H, Jiang Y, Yuan J. Positive surgical margin is associated with biochemical recurrence risk following radical prostatectomy: a meta-analysis from highquality retrospective cohort studies. World J Surg Oncol 2018; 16:124. https://doi.org/10.1186/s12957-018-1433-3.
doi: 10.1186/s12957-018-1433-3
[40]
Kv?le R, Myklebust T?, Foss? SD, Aas K, Ekanger C, Helle SI, et al. Impact of positive surgical margins on secondary treatment, palliative radiotherapy and prostate cancerspecific mortality. A population-based study of 13 198 patients. Prostate 2019;79: 1852e60.
[41]
Boevé LMS, Hulshof MCCM, Vis AN, Zwinderman AH, Twisk JWR, Witjes WPJ, et al. Effect on survival of androgen deprivation therapy alone compared to androgen deprivation therapy combined with concurrent radiation therapy to the prostate in patients with primary bone metastatic prostate cancer in a prospective randomised clinical trial. Eur Urol 2019; 75:410e8.
doi: 10.1016/j.eururo.2018.09.008
[42]
Fahmy O, Khairul-Asri MG, Hadi SHSM, Gakis G, Stenzl A. The role of radical prostatectomy and radiotherapy in treatment of locally advanced prostate cancer: a systematic review and meta-analysis. Urol Int 2017; 99:249e56.
doi: 10.1159/000478789
pmid: 28675891
[43]
Ranasinghe W, Chapin BF, Kim IY, Sooriakumaran P, Lawrentschuk N. The cytoreductive prostatectomy in metastatic prostate cancer: what the individual trials are hoping to answer. BJU Int 2020; 125:792e800.
doi: 10.1111/bju.15055
pmid: 32176456
[44]
Cheng B, Ye S, Bai P. The efficacy of cytoreductive surgery for oligometastatic prostate cancer: a meta-analysis. World J Surg Oncol 2021; 19:160. https://wjso.biomedcentral.com/articles/10.1186/s12957-021-02265-8.
doi: 10.1186/s12957-021-02265-8
pmid: 34051809
[45]
Becker JA, Berg KD, R?der MA, Brasso K, Iversen P. Cytoreductive prostatectomy in metastatic prostate cancer: a systematic review. Scand J Urol 2018 2; 52:1e7.
doi: 10.1080/21681805.2017.1363816
pmid: 28818014
[46]
Burdett S, Boevé LM, Ingleby FC, Fisher DJ, Rydzewska LH, Vale CL, et al. Prostate radiotherapy for metastatic hormonesensitive prostate cancer: a STOPCAP systematic review and meta-analysis. Eur Urol 2019; 76:115e24.
doi: S0302-2838(19)30111-3
pmid: 30826218
[47]
Reyes DK, Pienta KJ. The biology and treatment of oligometastatic cancer. Oncotarget 2015; 6:8491e524.
doi: 10.18632/oncotarget.3455
pmid: 25940699