Contemporary outcomes of patients undergoing robotic-assisted radical cystectomy: A comparative analysis between intracorporeal ileal conduit and neobladder urinary diversions
Jordan M. Richa,Shivaram Cumarasamya,Daniel Rantia,Etienne Lavalleea,Kyrollis Attallaa,John P. Sfakianosa,Nikhil Waingankara,Peter N. Wiklundab,Reza Mehrazina*()
aDepartment of Urology, Icahn School of Medicine at Mount Sinai, New York, NY, USA bDepartment of Urology, Karolinska University Hospital, Solna, Sweden
Objective: We aimed to compare perioperative and oncologic outcomes for patients undergoing robotic-assisted radical cystectomy (RARC) with intracorporeal ileal conduit (IC) and neobladder (NB) urinary diversion.
Methods: Patients undergoing RARC with intracorporeal urinary diversion between January 2017 and January 2022 at the Icahn School of Medicine at Mount Sinai, New York, NY, USA were indexed. Baseline demographics, clinical characteristics, perioperative, and oncologic outcomes were analyzed. Survival was estimated with Kaplan-Meier plots.
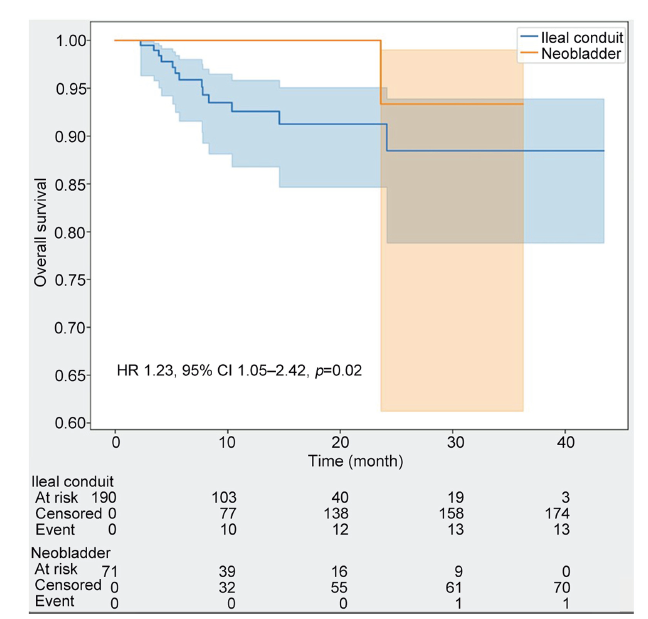
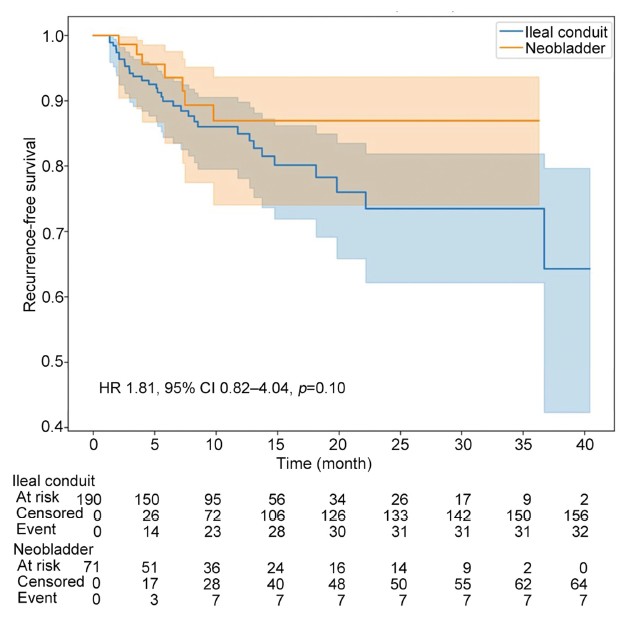
Results: Of 261 patients (206 [78.9%] male), 190 (72.8%) received IC while 71 (27.2%) received NB diversion. Median age was greater in the IC group (71 [interquartile range, IQR 65-78] years vs. 64 [IQR 59-67] years, p<0.001) and BMI was 26.6 (IQR 23.2-30.4) kg/m2. IC group was more likely to have prior abdominal or pelvic radiation (15.8% vs. 2.8%, p=0.014). American Association of Anesthesiologists scores were comparable between groups. The IC group had a higher proportion of patients with pathological tumor stage 2 (pT2) tumors (34 [17.9%] vs. 10 [14.1%], p=0.008) and pathological node stages pN2-N3 (28 [14.7%] vs. 3 [4.2%], p<0.001). The IC group had less median operative time (272 [IQR 246-306] min vs. 341 [IQR 303-378] min, p<0.001) and estimated blood loss (250 [150-500] mL vs. 325 [200-575] mL, p=0.002). Thirty- and 90-day complication rates were 44.4% and 50.2%, respectively, and comparable between groups. Clavien-Dindo grades 3-5 complications occurred in 27 (10.3%) and 34 (13.0%) patients within 30 and 90 days, respectively, with comparable rates between groups. Median follow-up was 324 (IQR 167-552) days, and comparable between groups. Kaplan-Meier estimate for overall survival at 24 months was 89% for the IC cohort and 93% for the NB cohort (hazard ratio 1.23, 95% confidence interval 1.05-2.42, p=0.02). Kaplan-Meier estimate for recurrence-free survival at 24 months was 74% for IC and 87% for NB (hazard ratio 1.81, 95% confidence interval 0.82-4.04, p=0.10).
Conclusion: Patients undergoing intracorporeal IC urinary diversion had higher postoperative cancer stage, increased nodal involvement, similar complications outcomes, decreased overall survival, and similar recurrence-free survival compared to patients undergoing RARC with intracorporeal NB urinary diversion.
. [J]. Asian Journal of Urology, 2023, 10(4): 446-452.
Jordan M. Rich, Shivaram Cumarasamy, Daniel Ranti, Etienne Lavallee, Kyrollis Attalla, John P. Sfakianos, Nikhil Waingankar, Peter N. Wiklund, Reza Mehrazin. Contemporary outcomes of patients undergoing robotic-assisted radical cystectomy: A comparative analysis between intracorporeal ileal conduit and neobladder urinary diversions. Asian Journal of Urology, 2023, 10(4): 446-452.
Lenis AT, Lec PM, Chamie K, Mshs M. Bladder cancer: a review. JAMA 2020; 324:1980-91.
doi: 10.1001/jama.2020.17598
pmid: 33201207
[2]
Witjes JA, Bruins HM, Cathomas R, Compérat EM, Cowan NC, Gakis G, et al. European Association of Urology guidelines on muscle-invasive and metastatic bladder cancer: summary of the 2020 guidelines. Eur Urol 2021;79:82-104.
[3]
Babjuk M, B?hle A, Burger M, Capoun O, Cohen D, Compérat EM, et al. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder: update 2016. Eur Urol 2017;71:447-61.
Zamboni S, Soria F, Mathieu R, Xylinas E, Abufaraj M, Andrea DD, et al. Differences in trends in the use of robotassisted and open radical cystectomy and changes over time in peri-operative outcomes among selected centres in North America and Europe: an international multicentre collaboration. BJU Int 2019; 124:656-64.
doi: 10.1111/bju.v124.4
[6]
Catto JWF, Khetrapal P, Ricciardi F, Ambler G, Williams NR, Al- Hammouri T, et al. Effect of robot-assisted radical cystectomy with intracorporeal urinary diversion vs. open radical cystectomy on 90-day morbidity and mortality among patients with bladder cancer: a randomized clinical trial. JAMA 2022; 327:2092-103.
doi: 10.1001/jama.2022.7393
pmid: 35569079
[7]
Parekh DJ, Reis IM, Castle EP, Gonzalgo ML, Woods ME, Svatek RS, et al. Robot-assisted radical cystectomy versus open radical cystectomy in patients with bladder cancer (RAZOR): an open-label, randomised, phase 3, non-inferiority trial. Lancet 2018; 391:2525-36.
[8]
Mastroianni R, Ferriero M, Tuderti G, Anceschi U, Bove AM, Brassetti A, et al. Open radical cystectomy versus robotassisted radical cystectomy with intracorporeal urinary diversion: early outcomes of a single-center randomized controlled trial. J Urol 2022; 207:982-92.
doi: 10.1097/JU.0000000000002422
pmid: 34986007
[9]
Zhou N, Tian F, Feng Y, Zhao K, Chen L, Fan R, et al. Perioperative outcomes of intracorporeal robot-assisted radical cystectomy versus open radical cystectomy: a systematic review and meta-analysis of comparative studies. Int J Surg 2021; 94:106137. https://doi.org/10.1016/j.ijsu.2021.106137.
doi: 10.1016/j.ijsu.2021.106137
[10]
Tyritzis SI, Hosseini A, Collins J, Nyberg T, Jonsson MN, Laurin O, et al. Oncologic, functional, and complications outcomes of robot-assisted radical cystectomy with totally intracorporeal neobladder diversion. Eur Urol 2013; 64:734-41.
doi: 10.1016/j.eururo.2013.05.050
pmid: 23768634
[11]
Williams SB, Cumberbatch MGK, Kamat AM, Jubber I, Kerr PS, McGrath JS, et al. Reporting radical cystectomy outcomes following implementation of enhanced recovery after surgery protocols: a systematic review and individual patient data meta-analysis. Eur Urol 2020; 78:719-30.
doi: 10.1016/j.eururo.2020.06.039
pmid: 32624275
[12]
Pyrgidis N, Sokolakis I, Haltmair G, Hatzichristodoulou G. The effect of urinary diversion on renal function after cystectomy for bladder cancer: comparison between ileal conduit, orthotopic ileal neobladder, and heterotopic ileocecal pouch. World J Urol 2022; 40:3091-7.
doi: 10.1007/s00345-022-04211-z
pmid: 36348070
[13]
Lee RK, Abol-Enein H, Artibani W, Bochner B, Dalbagni G, Daneshmand S, et al. Urinary diversion after radical cystectomy for bladder cancer: options, patient selection, and outcomes. BJU Int 2014; 113:11-23.
doi: 10.1111/bju.12121
pmid: 24330062
[14]
Demaegd L, Albersen M, Muilwijk T, Milenkovic U, Moris L, Everaerts W, et al. Comparison of postoperative complications of ileal conduits versus orthotopic neobladders. Transl Androl Urol 2020; 9:2541-54.
doi: 10.21037/tau-20-713
pmid: 33457228
[15]
MinerviniA, Serni S, VittoriG, Masieri L, SienaG, LanciottiM, et al. Current indications and results of orthotopic ileal neobladder for bladder cancer. Expert Rev Anticancer Ther 2014; 14:419-30.
doi: 10.1586/14737140.2014.867235
[16]
Fasanella D, Marchioni M, Domanico L, Franzini C, Inferrera A, Schips L, et al. Neobladder “function”: tips and tricks for surgery and postoperative management. Life 2022; 12:1193. https://doi.org/10.3390/life12081193.
doi: 10.3390/life12081193
[17]
Dutta SC, Chang SC, Coffey CS, Smith JA, Jack G, Cookson MS. Health related quality of life assessment after radical cystectomy: comparison of ileal conduit with continent orthotopic neobladder. J Urol 2002; 168:164-7.
pmid: 12050514
[18]
Somani BK, Gimlin D, Fayers P, N’dow J. Quality of life and body image for bladder cancer patients undergoing radical cystectomy and urinary diversionda prospective cohort study with a systematic review of literature. Urology 2009; 74:1138-43.
doi: 10.1016/j.urology.2009.05.087
[19]
Philip J, Manikandan R, Venugopal S, Desouza J, Javlé PM. Orthotopic neobladder versus ileal conduit urinary diversion after cystectomyda quality-of-life based comparison. Ann R Coll Surg Engl 2009; 91:565-9.
doi: 10.1308/003588409X432293
pmid: 19558757
[20]
Siracusano S, D’Elia C, Cerruto MA, Gacci M, Ciciliato S, Simonato A, et al. Quality of life following urinary diversion: orthotopic ileal neobladder versus ileal conduit. A multicentre study among long-term, female bladder cancer survivors. Eur J Surg Oncol 2019; 45:477-81.
doi: S0748-7983(18)31464-1
pmid: 30385155
[21]
Mastroianni R, Tuderti G, Anceschi U, Bove AM, Brassetti A, Ferriero M, et al. Comparison of patient-reported healthrelated quality of life between open radical cystectomy and robot-assisted radical cystectomy with intracorporeal urinary diversion: interim analysis of a randomised controlled trial. Eur Urol Focus 2022; 8:465-71.
[22]
Almassi N, Bochner BH. Ileal conduit or orthotopic neobladder: selection and contemporary patterns of use. Curr Opin Urol 2020; 30:415-20.
doi: 10.1097/MOU.0000000000000738
pmid: 32141937
[23]
Lavallee E, Sfakianos J, Mehrazin R, Wiklund P. Detailed description of the Karolinska technique for intracorporeal studer neobladder reconstruction. J Endourol 2022; 36: S67 e72. https://doi.org/10.1089/end.2022.0248.
doi: 10.1089/end.2022.0248
pmid: 36154454
[24]
Pfail JL, Garden EB, Gul Z, Katims AB, Rosenzweig SJ, Razdan S, et al. Implementation of a nonopioid protocol following robot-assisted radical cystectomy with intracorporeal urinary diversion. Urol Oncol 2021; 39:436. e9-16 https://doi.org/10.1016/j.urolonc.2021.01.002.
[25]
Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg 2009; 250: 187-96.
doi: 10.1097/SLA.0b013e3181b13ca2
pmid: 19638912
[26]
Su X, Wu K, Wang S, Su W, Li C, Li B, et al. The impact of orthotopic neobladder vs. ileal conduit urinary diversion after cystectomy on the survival outcomes in patients with bladder cancer: a propensity score matched analysis. Cancer Med 2020; 9:7590-600.
doi: 10.1002/cam4.v9.20
[27]
Nieuwenhuijzen JA, de Vries RR, Bex A, van der Poel HG, Meinhardt W, Antonini N, et al. Urinary diversions after cystectomy: the association of clinical factors, complications and functional results of four different diversions. Eur Urol 2008; 53:834-42; discussion 842e4.
doi: 10.1016/j.eururo.2007.09.008
pmid: 17904276
[28]
Abe T, Takada N, Shinohara N, Matsumoto R, Murai S, Sazawa A, et al. Comparison of 90-day complications between ileal conduit and neobladder reconstruction after radical cystectomy: a retrospective multi-institutional study in Japan. Int J Urol 2014; 21:554-9.
doi: 10.1111/iju.12357
pmid: 24304154
[29]
Yossepowitch O, Dalbagni G, Golijanin D, Donat SM, Bochner BH, Herr HW, et al. Orthotopic urinary diversion after cystectomy for bladder cancer: implications for cancer control and patterns of disease recurrence. J Urol 2003; 169: 177-81.
doi: 10.1097/01.ju.0000041411.03266.14
pmid: 12478130
[30]
Tuderti G, Mastroianni R, Brassetti A, Bove AM, Misuraca L, Anceschi U, et al. Robot-assisted radical cystectomy with intracorporeal neobladder: impact of learning curve and longterm assessment of functional outcomes. Minerva Urol Nephrol 2021; 73:754-62.
[31]
Ranti D, Pfail J, Garcia M, Razdan S, Bieber C, Rosenzweig S, et al. Neobladder creation in patients with chronic kidney disease: a viable diversion strategy. Urol Oncol 2022; 40: 168.e21-7. https://doi.org/10.1016/j.urolonc.2021.11.023.
doi: 10.1016/j.urolonc.2021.11.023
[32]
Stein JP, Lieskovsky G, Cote R, Groshen S, Feng AC, Boyd S, et al. Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1054 patients. J Clin Oncol 2001; 19:666-75.
doi: 10.1200/JCO.2001.19.3.666
pmid: 11157016