|
|
|
| Daily activities and training experiences of urology residents during the coronavirus disease 2019 pandemic in Indonesia: A nationwide survey |
Ponco Birowoa,*( ),Nur Rasyida,Chaidir A. Mochtara,Bambang S. Noegrohob,H.R. Danartoc,Besut Daryantod,Lukman Hakime,Dyandra Parikesitf,Fakhri Rahmana,S. Cahyo Ariwicaksonoa ),Nur Rasyida,Chaidir A. Mochtara,Bambang S. Noegrohob,H.R. Danartoc,Besut Daryantod,Lukman Hakime,Dyandra Parikesitf,Fakhri Rahmana,S. Cahyo Ariwicaksonoa
|
aDepartment of Urology, Faculty of Medicine, Universitas Indonesia, Cipto Mangunkusumo Hospital, Jakarta, Indonesia
bDepartment of Urology, Faculty of Medicine, Padjadjaran University, Hasan Sadikin Hospital, Bandung, Indonesia
cDepartment of Urology, Faculty of Medicine, Gadjah Mada University, Sardjito Hospital, Yogyakarta, Indonesia
dDepartment of Urology, Faculty of Medicine, Universitas Brawijaya, Saiful Anwar Hospital, Malang, Indonesia
eDepartment of Urology, Faculty of Medicine, Airlangga University, Soetomo Hospital, Surabaya, Indonesia
fDepartment of Urology, Faculty of Medicine, Universitas Indonesia, Universitas Indonesia Hospital, Depok, Indonesia |
|
|
|
|
Abstract Objective: To explore the impact of the coronavirus disease 2019 (COVID-19) pandemic on the training experiences of urology residents in Indonesia.
Methods: A cross-sectional study using a web-based questionnaire (SurveyMonkey) involved all registered urology residents in Indonesia. The questionnaire was structured in Bahasa Indonesia, composed of 28 questions, and divided into three sections: demographic characteristics, current daily activities, and opinions regarding training experiences during the COVID-19 outbreak. The survey was distributed to all respondents via chief of residents in each urology center from May 26, 2020 to Jun 2, 2020.
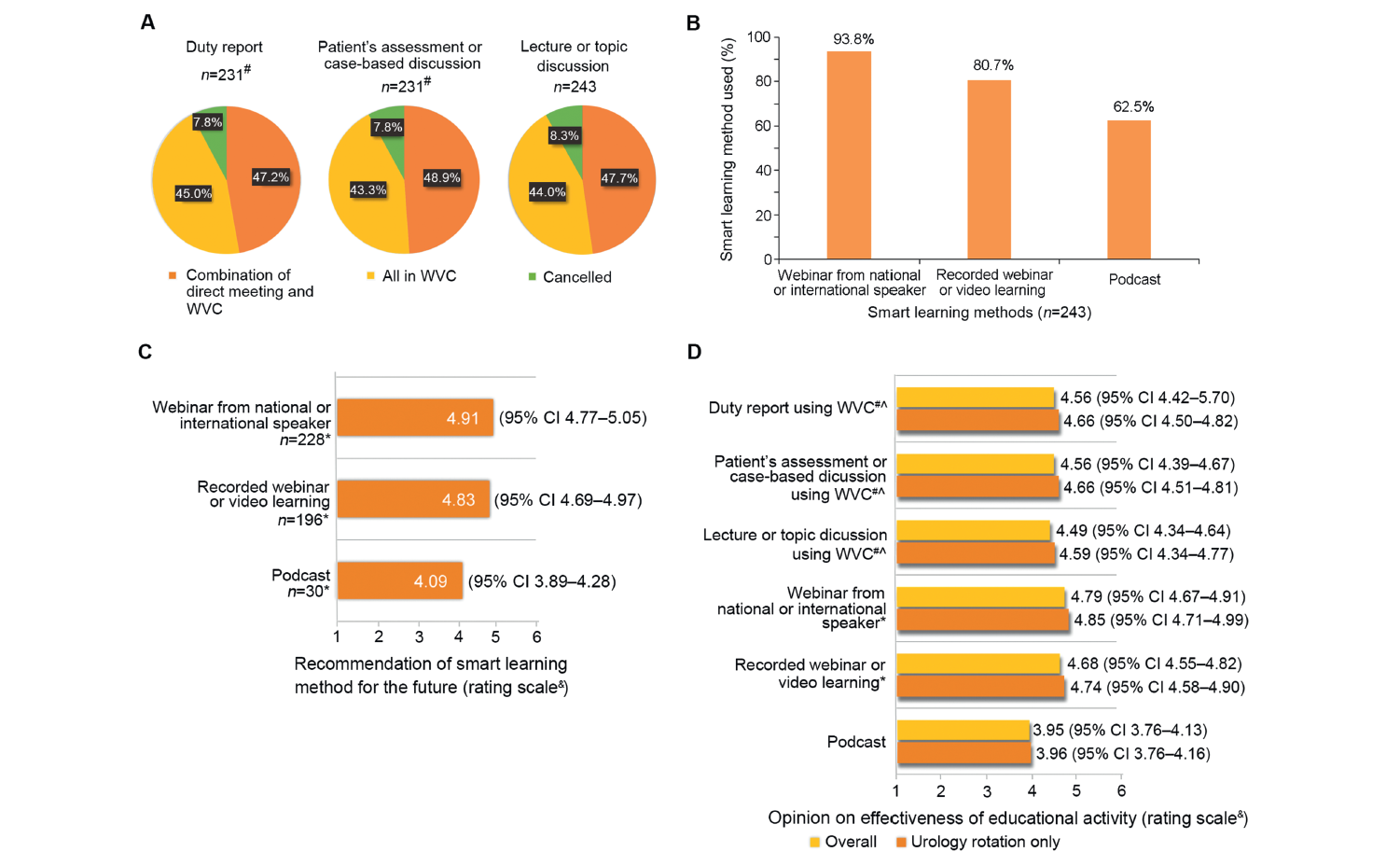
Results: Of the total 247 registered urology residents, 243 were eligible for the study. The response and completeness rate for this study were 243/243 (100%). The median age of respondents was 30 (range: 24-38) years old, and 92.2% of them were male. Among them, 6 (2.5%) respondents were confirmed as COVID-19 positive. A decrease in residents' involvement in clinical and surgical activities was distinguishable in endourological and open procedures. Most educational activities were switched to web-based video conferences, while others opted for the in-person method. Smart learning methods, such as joining a national or international speaker webinar or watching a recorded video, were used by 93.8% and 80.7% of the respondents, respectively. The respondents thought that educational activities using web-based video conferences and smart learning methods were effective methods of learning. Overall, the respondents felt unsure whether training experiences during the COVID-19 pandemic were comparable to the respective period before.
Conclusion: The COVID-19 pandemic negatively affected urology residents' training experiences. However, it also opened up new possibilities for incorporating new learning methodologies in the future.
|
|
Received: 07 September 2020
Available online: 20 April 2023
|
|
Corresponding Authors:
Ponco Birowo
E-mail: ponco.birowo@gmail.com
|
|
|

| Characteristic | Value | | Respondent, n | 243 | | Age, median (IQR), year | 30 (24-38) | | Gender, n (%) | | Male | 224 (92.2) | | Female | 19 (7.8) | | Urology center, n (%) | | Jakarta | 79 (32.5) | | Bandung | 50 (20.6) | | Yogyakarta | 27 (11.1) | | Malang | 29 (11.9) | | Surabaya | 58 (23.9) | | Year of study, n (%) | | First-year | 49 (20.2) | | Second-year | 53 (21.8) | | Third-year | 42 (17.3) | | Fourth-year | 45 (18.5) | | Fifth-year | 42 (17.3) | | Sixth-year and above | 12 (4.9) | | Current hospital placement, n (%) | | Center teaching hospital | 222 (91.4) | | Affiliated teaching hospital | 8 (3.3) | | Has not entered hospital rotation yet | 13 (5.3) | | COVID-19 status, n (%) | | Never infected or be appointed as a suspected case | 172 (70.8) | | Suspected case, but has not been further examined | 11 (4.5) | | Suspected case, but has been confirmed negative | 53 (21.8) | | Currently positive by rapid test | 1 (0.4) | | Currently positive by swab PCR test | 1 (0.4) | | Had been infected and was declared cured | 5 (2.1) |
|
|
Respondents' demographic characteristics.
|
| Category | Residency year | | First | Second | Third | Fourth | Fifth | Sixth and above | | Resident rotation, n (%) | | Pre-hospital | 12 (4.9) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | | General surgery | 32 (13.2) | 13 (5.3) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | | Urology | 5 (2.1) | 40 (16.5) | 42 (17.3) | 45 (18.5) | 24 (9.9) | 2 (0.8) | | Board exam candidate | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 18 (7.4) | 10 (4.1) | | Competency level, n (%) | | Level I (red) | 49 (20.2) | 45 (18.5) | 8 (3.3) | 0 (0) | 0 (0) | 0 (0) | | Level II (yellow) | 0 (0) | 8 (3.3) | 34 (14.0) | 42 (17.3) | 2 (0.8) | 2 (0.8) | | Level III (green) | 0 (0) | 0 (0) | 0 (0) | 3 (1.2) | 40 (16.5) | 10 (4.1) |
|
|
The relation between residency year with their current rotation and competency level (n=243).
|

|
|
Residents' activities and opinions on educational activities during the COVID-19 pandemic. (A) The methods used in education activities; (B) Smart learning methods used; (C) Residents' opinions on the future use of smart learning methods; (D) Residents' opinions on the effectiveness of the current educational methods used during the COVID-19 pandemic. COVID-19, coronavirus disease 2019. WVC, web-based video conference; CI, confidence interval. # Excluded pre-hospital rotation respondents; ∧ Excluded respondents of whom this activity was cancelled; ? Only included respondents using this smart learning method. & Rating scale: 1 represents strongly disagree; 6 represents strongly agree.
|
| Statement and variable | Rating scale, mean (95% CI)a | p-Value | | Opinion on educational activity | | “I preferred duty report using WVC compared to direct meeting”b,c | | Overall | 3.66 (3.47-3.84) | N/A | | Urology rotation only | 3.76 (3.53-3.99) | | | “I preferred patient's assessment or case-based discussion using WVC compared to direct meeting”b,c | | Overall | 3.66 (3.48-3.84) | N/A | | Urology rotation only | 3.74 (3.53-3.96) | | | “I preferred lecture or topic discussion using WVC compared to direct meeting”c | | Overall | 3.60 (3.42-3.78) | N/A | | Urology rotation only | 3.71 (3.49-3.94) | | | “I am satisfied with theory learning during COVID-19 pandemic.” | | Overall | 4.19 (4.02-4.36) | N/A | | Urology rotation only | 4.32 (4.11-4.52) | | | Opinion on clinical and surgical activity | | “I am satisfied with the case exposure during COVID-19 pandemic”b | | Overall | 2.78 (2.60-2.96) | 0.250d | | General surgery rotation | 2.93 (2.55-3.32) | | | Urology rotation | 2.85 (2.64-3.07) | | | Board exam candidate | 2.43 (1.93-2.93) | | | Level I (red) | 3.08 (2.79-3.37) | 0.052d | | Level II (yellow) | 2.65 (2.37-2.93) | | | Level III (green) | 2.67 (2.31-3.04) | |
|
|
Residents' opinions on educational activities and clinical and surgical activities.
|

|
|
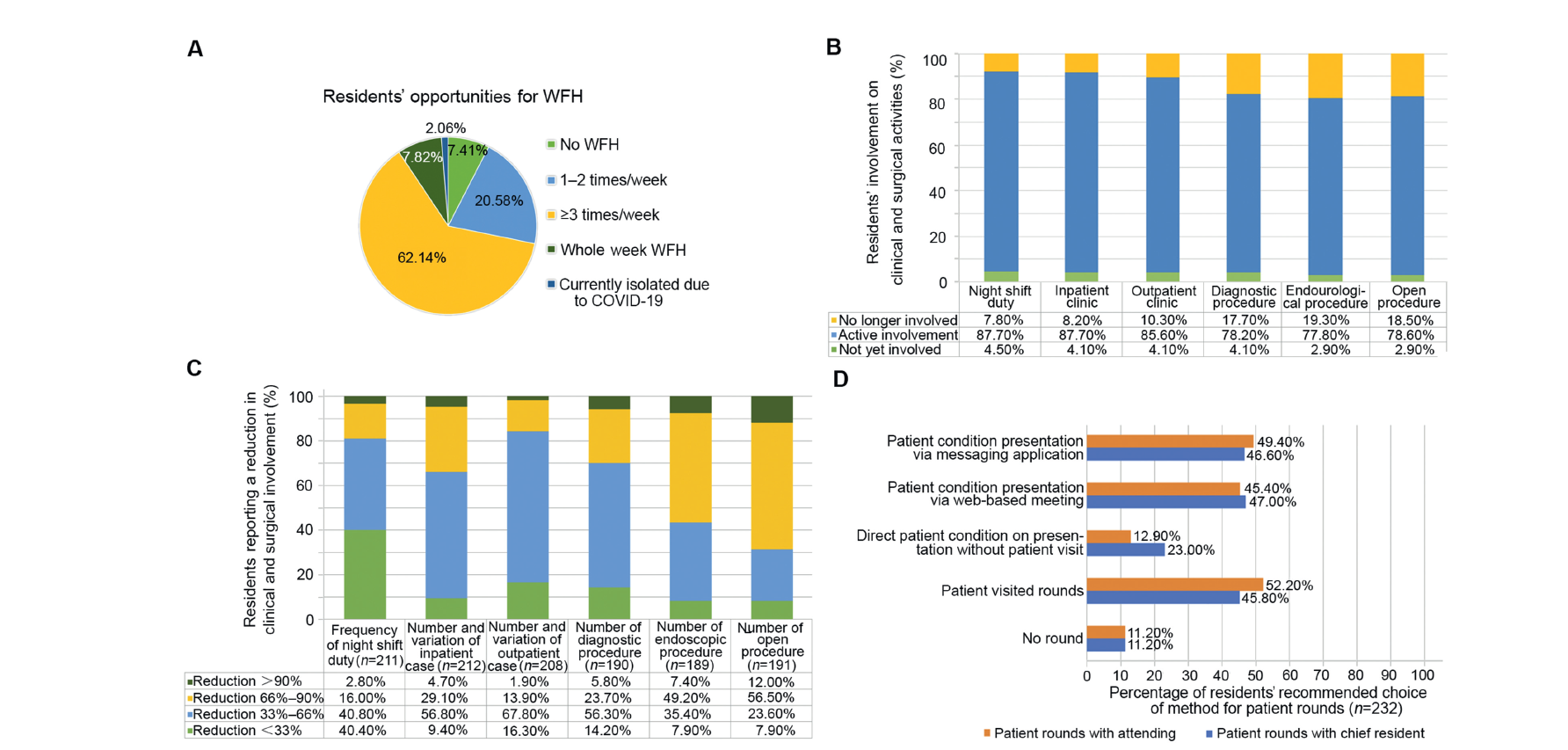
Residents' activities and opinions on clinical and surgical activities during the COVID-19 pandemic. (A) Residents' working from home opportunities; (B) Residents' involvement in clinical and surgical activities (n=243); (C) Reduction in residents' involvement in clinical and surgical activities; (D) Methods used in patient rounds (respondents could choose >1 method if applicated). COVID-19, coronavirus disease 2019; WFH, working from home.
|
| Statement and variable | Rating scale, mean (95% CI)a | p-Valueb | | “I am more productive in doing research during COVID-19 pandemic”c | | Overall | 4.03 (3.87-4.20) | 0.156 | | Pre-hospital rotation | 4.58 (3.84-5.32) | | | General surgery rotation | 3.93 (3.59-4.28) | | | Urology rotation | 4.11 (3.91-4.32) | | | Level I (red) | 4.05 (3.80-4.30) | 0.490 | | Level II (yellow) | 4.24 (3.99-4.49) | | | Level III (green) | 3.85 (3.21-4.49) | | | “I feel that training experience during COVID-19 pandemic is not different or even better compared to before.” | | Overall | 3.03 (2.85-3.21) | 0.433 | | Pre-hospital rotation | 3.50 (2.40-4.60) | | | General surgery rotation | 3.09 (2.69-3.49) | | | Urology rotation | 3.02 (2.79-3.24) | | | Board exam candidate | 2.79 (2.33-3.24) | | | Level I (red) | 3.17 (2.88-3.46) | 0.330 | | Level II (yellow) | 2.93 (2.63-3.23) | | | Level III (green) | 2.93 (2.57-3.28) | | | “I feel a heavier workload during COVID-19 pandemic compared to before.” | | Overall | 2.68 (2.53-2.83) | 0.004d | | Pre-hospital rotation | 3.00 (2.19-3.81) | | | General surgery rotation | 3.02 (2.72-3.33) | | | Urology rotation | 2.63 (2.44-2.82) | | | Board exam candidate | 2.18 (1.76-2.60) | | | Level I (red) | 2.89 (2.64-3.14) | 0.018d | | Level II (yellow) | 2.59 (2.37-2.81) | | | Level III (green) | 2.40 (2.08-2.72) | | | “I feel a greater mental burden or stress during COVID-19 pandemic compared to before.” | | Overall | 3.43 (3.25-3.60) | 0.724 | | Pre-hospital rotation | 3.75 (3.08-4.42) | | | General surgery rotation | 3.52 (3.15-3.89) | | | Urology rotation | 3.36 (3.14-3.59) | | | Board examination candidate | 3.36 (2.75-3.97) | | | Level I (red) | 3.52 (3.25-3.79) | 0.422 | | Level II (yellow) | 3.26 (2.99-3.53) | | | Level III (green) | 3.45 (3.03-3.88) | |
|
|
Residents' opinions on research and overall activities.
|

|
|
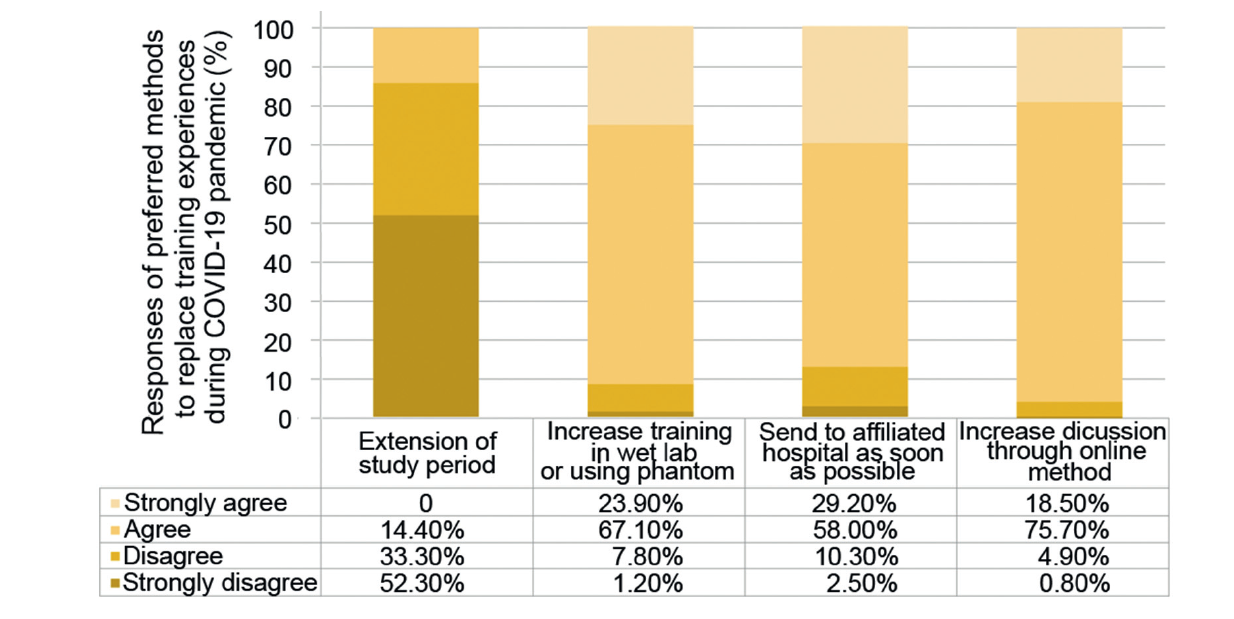
Residents' suggestions of preferred methods to overcome lack of experiences during COVID-19 pandemic. COVID-19, coronavirus disease 2019.
|
| [1] |
Nicola M, Alsafi Z, Sohrabi C, Kerwan A, Al-Jabir A, Iosifidis C, et al. The socioeconomic implications of the coronavirus and COVID-19 pandemic: a review. Int J Surg 2020; 78:185-93.
doi: S1743-9191(20)30316-2
pmid: 32305533
|
| [2] |
Haleem A, Javaid M, Vaishya R. Effects of COVID-19 pandemic in daily life. Curr Med Res Pract 2020; 10:78-9.
doi: 10.1016/j.cmrp.2020.03.011
|
| [3] |
WHO. WHO coronavirus disease (COVID-19) dashboard. https://covid19.who.int. [Accessed 24 May 2020].
|
| [4] |
Teoh J, Ong WL, Gonzalez-Padilla D, Castellani D, Dubin J, Esperto F, et al. A global survey on the impact of COVID-19 on urological services. Eur Urol 2020; 78:265-75.
doi: 10.1016/j.eururo.2020.05.025
|
| [5] |
Rasyid N, Birowo P, Parikesit D, Rahman F. Impact of the COVID-19 pandemic on urology practice in Indonesia: a nationwide survey. Urol J 2020; 17:129-31.
|
| [6] |
Abdessater M, Rouprêt M, Misrai V, Matillon X, Tellier BG, Freton L, et al. COVID-19 pandemic impact on anxiety of French urologists in training: outcomes from a national survey. Prog Urol 2020; 30:448-55.
doi: S1166-7087(20)30137-8
pmid: 32376208
|
| [7] |
Amparore D, Claps F, Cacciamani GE, Esperto F, Fiori C, Liguori G, et al. Impact of the COVID-19 pandemic on urology residency training in Italy. Minerva Urol Nefrol 2020; 72:505-9.
doi: 10.23736/S0393-2249.20.03868-0
pmid: 32253371
|
| [8] |
Porpiglia F, Checcucci E, Amparore D, Verri P, Campi R, Claps F, et al. Slowdown of urology residents’ learning curve during COVID-19 emergency. BJU Int 2020:3-5.
|
| [9] |
Kwon YS, Tabakin AL, Patel HV, Backstrand JR, Jang TL, Kim IY, et al. Adapting urology residency training in the COVID-19 era. Urology 2020; 141:15-9.
doi: S0090-4295(20)30452-0
pmid: 32339555
|
| [10] |
Malhotra R, Gautam D, George J. Orthopaedic resident management during the COVID-19 pandemicdAIIMS model. J Clin Orthop Trauma 2020; 11:S307-8. https://doi.org/10.1016/j.jcot.2020.05.001.
doi: 10.1016/j.jcot.2020.05.001
|
| [11] |
Ehrlich H, McKenney M, Elkbuli A. Protecting our healthcare workers during the COVID-19 pandemic. Am J Emerg Med 2020; 38:1527-8.
doi: S0735-6757(20)30252-7
pmid: 32336585
|
| [12] |
Agarwal S, Sabadia S, Abou-Fayssal N, Kurzweil A, Balcer LJ, Galetta SL. Training in neurology: flexibility and adaptability of a neurology training program at the epicenter of COVID-19. Neurology 2020; 94:e2608-14. https://doi.org/10.1212/WNL.0000000000009675.
doi: 10.1212/WNL.0000000000009675
|
| [13] |
Giao H, Le An P, Thi Ngoc Han N, Van Khanh T, Kim Ngan V, Van Tam V. Knowledge and attitude toward COVID-19 among healthcare workers at district 2 hospital, Ho Chi Minh City. Asian Pac J Trop Med 2020; 13:6-11.
|
| [14] |
Zhang M, Zhou M, Tang F, Wang Y, Nie H, Zhang L, et al. Knowledge, attitude, and practice regarding COVID-19 among healthcare workers in Henan, China. J Hosp Infect 2020; 105:183-7.
doi: S0195-6701(20)30187-0
pmid: 32278701
|
| [15] |
Zingaretti N, Negrini F, Tel A, Tresoldi M, Bresadola V, Parodi P. The impact of COVID-19 on plastic surgery residency training. Aesth Plast Surg 2020; 44:1381-5.
doi: 10.1007/s00266-020-01789-w
|
| [16] |
Busetto GM, Del Giudice F, Mari A, Sperduti I, Longo N, Antonelli A, et al. How can the COVID-19 pandemic lead to positive changes in urology residency? Front Surg 2020; 7:1-10.
doi: 10.3389/fsurg.2020.00001
|
| [17] |
Hameed BZ, Tanidir Y, Naik N, Teoh JYC, Shah M, Wroclawski ML, et al. Will “hybrid” meetings replace face-toface meetings post COVID-19 era? Perceptions and views from the urological community. Urology 2021:1-6.
|
| [18] |
Chick RC, Clifton GT, Peace KM, Propper BW, Hale DF, Alseidi AA, et al. Using technology to maintain the education of residents during the COVID-19 pandemic. J Surg Educ 2020; 77:729-32.
doi: S1931-7204(20)30084-2
pmid: 32253133
|
| [19] |
Coe TM, Jogerst KM, Sell NM, Cassidy DJ, Eurboonyanun C, Gee D, et al. Practical techniques to adapt surgical resident education to the COVID-19 era. Ann Surg 2020:e139-41.
|
| [1] |
Youssef Kharbach,Abdelhak Khallouk. Male genital damage in COVID-19 patients: Are available data relevant?[J]. Asian Journal of Urology, 2021, 8(3): 324-326. |
| [2] |
Fubo Wang,Chao Zhang,Fei Guo,Xia Sheng,Jin Ji,Yalong Xu,Zhi Cao,Ji Lyu,Xiaoying Lu,Bo Yang. The application of virtual reality training for anastomosis during robot-assisted radical prostatectomy[J]. Asian Journal of Urology, 2021, 8(2): 204-208. |
| [3] |
Bohdan Baralo,Patrick Samson,David Hoenig,Arthur Smith. Percutaneous kidney stone surgery and radiation exposure: A review[J]. Asian Journal of Urology, 2020, 7(1): 10-17. |
| [4] |
Dominique Thomas,Kevin C. Zorn,Nadir Zaidi,Stephanie Ashley Chen,Yiye Zhang,Alexis Te,Bilal Chughtai. Does urodynamics predict voiding after benign prostatic hyperplasia surgery in patients with detrusor underactivity?[J]. Asian Journal of Urology, 2019, 6(3): 264-269. |
| [5] |
Qixiang Song,Paul Abrams,Yinghao Sun. Beyond prostate, beyond surgery and beyond urology: The “3Bs” of managing non-neurogenic male lower urinary tract symptoms[J]. Asian Journal of Urology, 2019, 6(2): 169-173. |
| [6] |
Allert M.de Vries*,John P.F.A.Heesakkers. Contemporary diagnostics and treatment options for female stress urinary incontinence[J]. Asian Journal of Urology, 2018, 5(3): 141-148. |
| [7] |
Aldamanhori Reem,I.Osman Nadir,R.Chapple Christopher. Underactive bladder: Pathophysiology and clinical significance[J]. Asian Journal of Urology, 2018, 5(1): 17-21. |
| [8] |
Kok Bin Lim. Epidemiology of clinical benign prostatic hyperplasia[J]. Asian Journal of Urology, 2017, 4(3): 148-151. |
| [9] |
Linhui Wang, Cunzhou Wang, Chuangyu Qu, Lei Yin, Danfeng Xu, Xingang Cui, Bing Liu. Relationship between urodynamic patterns and lower urinary tract symptoms in Chinese women with a non-neurogenic bladder[J]. Asian Journal of Urology, 2016, 3(1): 10-19. |
|
|
|
|