Stone-scoring systems for predicting complications in percutaneous nephrolithotomy: A systematic review of the literature
Giorgio Mazzona*(),Simon Choongb,Antonio Celiaa
a Department of Urology, AULSS7 Pedemontana, San Bassiano Hospital, Bassano Del Grappa, Italy b Institute of Urology, University College Hospitals of London, London, UK
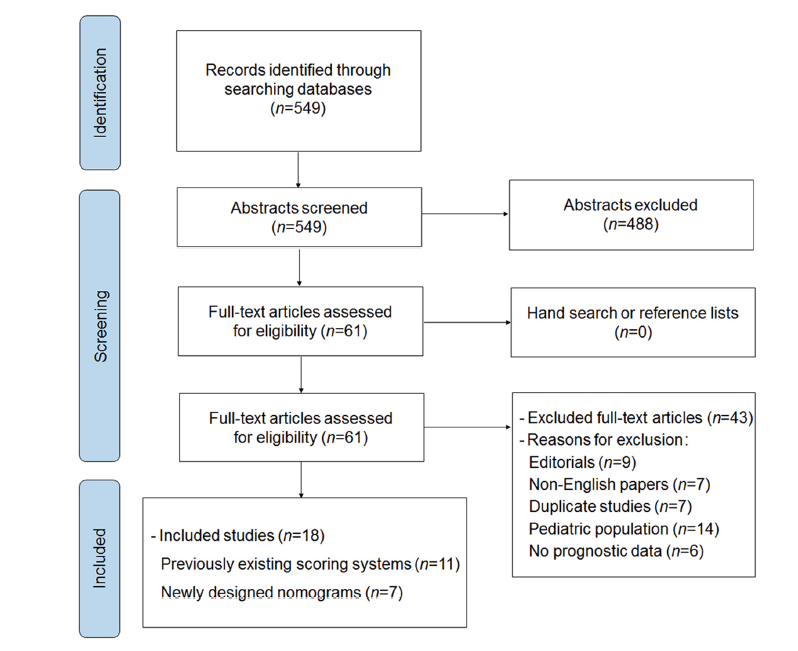
Objective Percutaneous nephrolithotomy is a treatment of choice for larger stones of the upper urinary tract. Currently, several nephrolithometric nomograms for prediction of post-operative surgical outcomes have been proposed, although uncertainties still exist regarding their roles in the estimation of complications. Methods We conducted a systematic review on PubMed and Web of Sciences databases including English studies with at least 100 cases and published between January 2010 and December 2021. We identified original articles evaluating correlations between the Guy's stone score, the stone size (S), tract length (T), obstruction (O), number of involved calices (N), and essence or stone density (E) (S.T.O.N.E.), Clinical Research Office of the Endourological Society (CROES), and Seoul National University Renal Stone Complexity (S-ReSC) scores and post-operative complications in adult patients. We also included newly designed nomograms for prediction of specific complications. Results After an initial search of 549 abstracts, we finally included a total of 18 papers. Of them, 11 investigated traditional nephrolithometric nomograms, while seven newly designed nomograms were used to predict specific complications. Overall, 7316 patients have been involved. In total, 14 out of 18 papers are derived from retrospective single-center studies. Guy's stone score obtained correlation with complications in five, S.T.O.N.E. nephrolithometry score in four, while CROES score and S-ReSC score in three and two, respectively. None of the studies investigated minimally invasive percutaneous nephrolithotomy (PCNL) and all cases have been conducted in prone position. Considering newly designed nomograms, none of them is currently externally validated; five of them predict post-operative infections; the remaining two have been designed for thromboembolic events and urinary leakage. Conclusion This review presents all nomograms currently available in the PCNL field and highlights a certain number of concerns. Published data have appeared contradictory; more recent tools for prediction of post-operative complications are frequently based on small retrospective cohorts and lack external validations. Heterogeneity among studies has also been noticed. More rigorous validations are advisable in the future, involving larger prospective patients’ series and with the comparison of different tools.
. [J]. Asian Journal of Urology, 2023, 10(3): 226-238.
Giorgio Mazzon,Simon Choong,Antonio Celia. Stone-scoring systems for predicting complications in percutaneous nephrolithotomy: A systematic review of the literature. Asian Journal of Urology, 2023, 10(3): 226-238.
Nomogram name if available and investigated endpointsa
Included variable
Externally validated
Method for calculation
Thomas et al. [8]
Guy’s stone score; SFR
·? Grade I: a solitary stone in the mid-lower pole, or renal pelvis with simple anatomy ·? Grade II: a solitary stone in the upper pole with simple anatomy, multiple stones in a patient with simple anatomy, or any solitary stone in a patient with abnormal anatomy ·? Grade III: multiple stones in a patient with abnormal anatomy, stones in a calyceal diverticulum, or partial staghorn calculus ·? Grade IV: staghorn calculus or any stone in a patient with spina bifida or spinal injury
Yes
Computed tomography imaging
Okhunov et al. [9]
S.T.O.N.E. nephrolithometry score; SFR
·? S.T.O.N.E.
Yes
Graphic chart
Smith et al. [10]
CROES score; SFR
·? Stone burden, stone location, number of stones, and surgical volume
Yes
Graphic chart
Jeong et al. [11]
S-ReSC; SFR
·? Pelvi-caliceal system subdivided in nine separate locations, each location corresponding to 1 point ·? Total score: cumulative sum of involved locations
Yes
Computed tomography imaging
Xun et al. [24]
Urosepsis in general population
·? Albumin-globulin ratio, leukocytosis, positive urine culture, and female sex
No
Graphic chart
Jiang et al. [25]
Post-operative fever, SIRS, sepsis in general population
·? Post-operative fever: leukocyturia and urine nitrite ·? SIRS: positive urine culture, positive urine nitrite, and operation time ·? Sepsis: positive urine nitrites, urine pH, positive urine culture, serum calcium, and operation time
No
Computer software and graphic chart
Wang et al. [26]
Urosepsis in general population
·? Presence of staghorn stone, pre-operative urine culture, and pre-operative nephrostomy
No
Graphic chart
Gu et al. [28]
Urosepsis in general population
·? Presence of urine nitrite, positive urine culture, intra-operative hypotension, and staghorn stone
No
Graphic chart
Liu et al. [27]
Urosepsis in general population
·? White blood cell count, presence of urine nitrites, positive urine culture, staghorn stone, and complete stone clearance
Post-operative complications according to CD system
·? Complication rate was 29.2%, and CD 3 or higher was 3.4%
Farhan et al. [15]
Pakistan
Prospective, single-center study
2014
·? 107 patients with radio-opaque renal stones ·? Pre-operative imaging: CT ·? Patients with indwelled nephrostomy or ureteric stent, previous ipsilateral surgery for stones and radiolucent stones excluded ·? Investigated nomogram: S.T.O.N.E. nephrolithometry score
Single-tract standard prone PCNL (tract size not mentioned), dilatation carried out with Alken dilators, and stone fragmentation obtained with ultrasonic-ballistic device
Post-operative complications according to CD system
·? 22 (20.8%) patients had complications: one patient had CD 1, 11 had CD 2, seven had CD 3a, and three had CD 3b
Yarimoglu et al. [16]
Turkey
Retrospective, single-center study
2012-2015
·? 262 patients with renal stones ·? Pre-operative imaging: CT ·? Investigated nomograms: S.T.O.N.E. nephrolithometry score and CROES score
Prone PCNL, unspecified the track diameter: 14 Fr nephrostomy tube placed at completion of case
Post-operative complications according to CD system and EBL
·? 89 patients had post-operative complications: 41 (15.6%) patients had CD 1; 35 (13.4%) had CD 2; 5 (1.9%) had CD 3a; and 8 (3.1%) had CD 3b.
Prone standard PCNL, unspecified the track diameter: 14 Fr nephrostomy tube placed at completion
Post-operative complications according to CD classification system and EBL
·? 159 patients had post-operative complications: 70 (13.8%) patients had CD 1; 57 (11.2%) had CD 2; 27 (5.3%) had CD 3a; and 5 (0.98%) had CD 3b
Biswas et al. [18]
India
Prospective, single-center study
2017-2019
·? 252 patients with renal stones ·? Pre-operative imaging: CT ·? Second stage PCNL excluded or with pre-operative percutaneous nephrostomy or double-J stent ·? Investigated nomograms: GSS, S.T.O.N.E. nephrolithometry score, and CROES score
Single stage more than 26 Fr prone PCNL, lithotripsy carried out with ultrasonic and ballistic device: routinely a 20 Fr percutaneous drainage placed at completion
Intra-operative complications, post-operative complications according to CD classification system and EBL
·? 120 (48%) patients had complications: CD 1 was 33% ·? Mean EBL was 1.4-2.0 g/dL in stone-free group while it was 2.0 g/dL in non-stone-free group
Labadie et al. [19]
The United States
Retrospective, multi-center study
2009-2012
·? 246 patients with unilateral renal stone ·? Pre-operative imaging: CT ·? Exclusion criteria: patients with history of prior surgery on same kidney and those with indwelled percutaneous nephrostomy or double-J stent ·? Investigated nomograms: GSS, S.T.O.N.E. nephrolithometry score, and CROES score
Standard PCNL
Intra-operative complications and post-operative complications within 30 days according to CD classification system and EBL
·? 42 (17%) patients had post-operative complications: CD 1 was 23; CD 2 was 8; CD 3a was 5; CD 3b was 3; and CD 4a was 3
Choi et al. [20]
The Republic of Korea
Retrospective, single-center study
2003-2014
·? 217 patients with staghorn stones and available CT imaging pre-operatively ·? Investigated nomograms: GSS, S.T.O.N.E. nephrolithometry score, and CROES score
24-30 Fr prone PCNL, lithotripsy with ultrasonic-ballistic device: 20 Fr nephrostomy tube and/or double-J stent at completion
Post-operative complications according to CD classification system
·? 71 patients had complications: 45 were minor (CD 1-2) and 26 were major (CD 3a-5)
Choi et al. [21]
The Republic of Korea
Retrospective, single-center study
2012-2015
·? 141 patients with unilateral renal stones ·? Pre-operative imaging: CT ·? Exclusion criteria: bilateral simultaneous PCNL, more than three tracks PCNL, and serious intra-operative bleeding or perforation of collecting system ·? Investigated nomograms: GSS, S.T.O.N.E. nephrolithometry score, and CROES score
24 Fr tubeless prone PCNL
Post-operative complications according to CD classification system
·? 36 (25.5%) complications registered in 24 (17.0%) patients: CD I was 9 (6.4%); CD 2 was 11 (7.8%); CD 3a was 8 (5.7%); CD 3b was 3 (2.1%); CD 4a was 1 (0.7%); CD 4b was 3 (2.1%); and CD 5 was 1 (0.7%)
Al Adl et al. [22]
Egypt
Prospective, single-center Study
2015-2018
·? 166 patients with renal stones ·? Pre-operative imaging: CT ·? Patients with preliminary percutaneous nephrostomy or double-J stent excluded ·? Investigated nomograms: GSS, S.T.O.N.E. nephrolithometry score, CROES score, and S-ReSC score
Single stage standard PCNL
Post-operative complications according to CD system
·? 14 (8.4%) patients had CD 1; 26 (15.7%) had CD 2; 5 (3.1%) had CD 3a; and 5 (3.0%) had CD 3b
Khan et al. [23]
Pakistan
Prospective, single-center study
2015-2017
·? 190 patients with unilateral radio-opaque renal stones ·? Exclusion criteria: radiolucent and bilateral stones, previous ipsilateral surgery for stones, blood clotting disorders, and urinary tract infections
Single tract 26 Fr prone PCNL: 24 Fr nephroscope, lithotripsy with ultrasonic-ballistic device
Post-operative complications according to CD system
·? 24 patients (12.6%) had post-operative complications: CD 1-2 were 16 ·? Six patients required blood-transfusion; ·? One patient had angioembolization
Study
Country
Study design
Study period
Participant variable
Used technique
Analyzed complication
Key result
Xun et al. [24]
China
Retrospective, single-center study
2012-2018
·? 745 patients treated for unilateral solitary ureteric stone larger than 10 mm in diameter ·? Patients with abnormal anatomy excluded ·? Pre-operative imaging: NCCT
·? Not clarified
·? Sepsis defined according to 2001 International Sepsis Definitions Conference
·? 969 patients treated for renal stones ·? Patients with pre-operative fever excluded ·? Not mentioned other inclusion or exclusion criteria ·? Pre-operative imaging: unclear whether all patients received CT imaging ·? Inflammatory markers not included as well as whether patients were pre-stented
·? 18-24 Fr PCNL, not specified the patients’ position ·? High-power Ho:YAG laser lithotripsy in all cases
·? Post-operative fever defined as temperature over 38°C ·? Post-operative SIRS defined according to Society of Critical Care Medicine in 2001 ·? Sepsis defined using qSOFA criteria
·? 216 (22.3%) patients had fever; 166 (17.1%) had SIRS; and 25 (2.6%) had urosepsis ·? Unclear whether internally validated
Wang et al. [26]
China
Retrospective, single-center study
2017-2019
·? 246 patients included with either renal or upper ureteric stones ·? Unclear how staghorn stones have been defined ·? Exclusion criteria: pre-existing neoplasms, urinary tract tuberculosis, incomplete medical records ·? Unclear pre-operative imaging ·? Pre-operative inflammatory markers not presented
·? 22-24 Fr prone PCNL, 17-22 Fr nephroscope, lithotripsy carried out with either high-power Ho-YAG laser or ultrasonic lithotripsy ·? All patients had percutaneous nephrostomy and a 5 Fr double-J stent at completion
·? Post-operative sepsis defined according to qSOFA criteria
·? 15 (6.1%) patients developed post-operative sepsis ·? Internally validated
Gu et al. [28]
China
Retrospective, single-center study
2010-2020
·? 366 diabetic patients (diagnosed with 2-h 75 g post-load plasma glucose level, oral glucose tolerance test, or fasting plasma glucose) with renal stones ·? Urosepsis defined using SIRS criteria (two or more criteria)
·? One-stage 24 Fr prone PCNL ·? All patients had both double-J stent and percutaneous nephrostomy inserted
·? Urosepsis within 24 h from surgery
·? 71 out of 366 (19.4%) patients had post-operative urosepsis ·? Unclear if internally validated
Liu et al. [27]
China
Retrospective, single-center study
2012-2019
·? 241 diabetic patients (diagnosed with 2-h 75 g postload plasma glucose level, oral glucose tolerance test, or fasting plasma glucose) with renal stones ·? Infectious events diagnosed using SIRS criteria
·? One-stage 24 Fr prone PCNL under spinal anesthesia
·? Urosepsis within 24 h from surgery
·? Urosepsis occurred in 41 (17.0%) patients, all within 24 h from surgery ·? Internally validated
Zeng et al. [29]
China
Retrospective, single-center study
2018-2020
·? 896 adult patients ·? Patients with tachycardia or chest pain were suspected for PE and undergone CT angiogram of the chest or ventilation-perfusion lung scan ·? Patients with increased D-dimer or Caprini RAM score received a lower limb Doppler scan
·? Not clarified
·? Cumulative risk of DVT and PE
·? Overall risk was 2.8% (25 patients) ·? 1 out of 25 patients experienced PE while the others had DVT only ·? Unclear if internally validated
Sahan et al. [30]
Turkey
Retrospective, single-center study
2011-2020
·? 932 patients included ·? Urine leakage if persisting for more than 24 h post-operatively ·? Patient stented post-operatively excluded
·? 26 Fr prone PCNL, 14 Fr percutaneous nephrostomy tube placed in all cases
·? Urinary leakage
·? Risk of urine leakage was 9.9% ·? Patients stratified in low-, moderate- and high-risk of complication ·? Internally validated
[1]
Zeng G, Zhong W, Mazzon G, Choong S, Pearle M, Agrawal M, et al. International Alliance of Urolithiasis (IAU) guideline on percutaneous nephrolithotomy. Minerva Urol Nephrol 2022; 74: 653-68.
doi: 10.23736/S2724-6051.22.04752-8
pmid: 35099162
Pietropaolo A, Proietti S, Geraghty R, Skolarikos A, Papatsoris A, Liatsikos E, et al. Trends of urolithiasis: interventions, simulation, and laser technology' over the last 16 years (2000-2015) as published in the literature (PubMed): a systematic review from European section of Uro-technology (ESUT). World J Urol 2017;35:1651-8.
[4]
Pietropaolo A, Proietti S, Jones P, Rangarajan K, Aboumarzouk O, Giusti G, et al. Trends of intervention for paediatric stone disease over the last two decades (2000-2015): a systematic review of literature. Arab J Urol 2017; 15:306-11.
doi: 10.1016/j.aju.2017.10.006
[5]
Michel MS, Trojan L, Rassweiler JJ. Complications in percutaneous nephrolithotomy. Eur Urol 2007; 51:899-906.
doi: 10.1016/j.eururo.2006.10.020
[6]
Kamphuis GM, Baard J, Westendarp M, de la Rosette JJ. Lessons learned from the CROES percutaneous nephrolithotomy global study. World J Urol 2015; 33:223-33.
doi: 10.1007/s00345-014-1367-5
pmid: 25100624
[7]
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Rev Esp Cardiol 2021; 74:790-9.
doi: 10.1016/j.recesp.2021.06.016
[8]
Thomas K, Smith NC, Hegarty N, Glass JM. The Guy's stone scoredgrading the complexity of percutaneous nephrolithotomy procedures. Urology 2011; 78:277-81.
doi: 10.1016/j.urology.2010.12.026
pmid: 21333334
[9]
Okhunov Z, Friedlander JI, George AK, Duty BD, Moreira DM, Srinivasan AK, et al. S.T.O.N.E. nephrolithometry novel surgical classification system for kidney calculi. Urology 2013; 81: 1154-9.
doi: 10.1016/j.urology.2012.10.083
[10]
Smith A, Averch TD, Shahrour K, Opondo D, Daels FP, Labate G, et al. A nephrolithometric nomogram to predict treatment success of percutaneous nephrolithotomy. J Urol 2013; 190:149-56.
doi: 10.1016/j.juro.2013.01.047
pmid: 23353048
[11]
Jeong CW, Jung JW, Cha WH, Lee BK, Lee S, Jeong SJ, et al. Seoul National University renal stone complexity score for predicting stone-free rate after percutaneous nephrolithotomy. PLoS One 2013; 8:e65888. https://doi.org/10.1371/journal.pone.0065888.
doi: 10.1371/journal.pone.0065888
[12]
Ozgor F, Yanaral F, Savun M, Ozdemir H, Sarilar O, Binbay M. Comparison of STONE, CROES and Guy's nephrolithometry scoring systems for predicting stone-free status and complication rates after percutaneous nephrolithotomy in obese patients. Urolithiasis 2018; 46:471-7.
doi: 10.1007/s00240-017-1003-0
pmid: 28756459
[13]
de la Rosette JJ, Opondo D, Daels FP, Giusti G, Serrano A, Kandasami SV, et al. Categorisation of complications and validation of the Clavien score for percutaneous nephrolithotomy. Eur Urol 2012; 62:246-55.
doi: 10.1016/j.eururo.2012.03.055
pmid: 22487016
[14]
Tailly TO, Okhunov Z, Nadeau BR, Huynh MJ, Labadie K, Akhavein A, et al. Multicenter external validation and comparison of stone scoring systems in predicting outcomes after percutaneous nephrolithotomy. J Endourol 2016; 30: 594-601.
doi: 10.1089/end.2015.0700
pmid: 26728427
[15]
Farhan M, Nazim SM, Salam B, Ather MH. Prospective evaluation of outcome of percutaneous nephrolithotomy using the ‘STONE' nephrolithometry score: a single-centre experience. Arab J Urol 2015; 13:264-9.
doi: 10.1016/j.aju.2015.07.006
[16]
Yarimoglu S, Polat S, Bozkurt IH, Yonguc T, Aydogdu O, Aydin E, et al. Comparison of S.T.O.N.E and CROES nephrolithometry scoring systems for predicting stone-free status and complication rates after percutaneous nephrolithotomy: a single center study with 262 cases. Urolithiasis 2017; 45:489-94.
[17]
Yarimoglu S, Bozkurt IH, Aydogdu O, Yonguc T, Gunlusoy B, Degirmenci T.External validation and comparisons of the scoring systems for predicting percutaneous nephrolithotomy outcomes: a single center experience with 506 cases. J Laparoendosc Adv Surg Tech 2017; 27:1284-9.
[18]
Biswas K, Gupta SK, Tak GR, Ganpule AP, Sabnis RB, Desai MR. Comparison of STONE score, Guy's stone score and Clinical Research Office of the Endourological Society (CROES) score as predictive tools for percutaneous nephrolithotomy outcome: a prospective study. BJU Int 2020; 126: 494-501.
doi: 10.1111/bju.v126.4
[19]
Labadie K, Okhunov Z, Akhavein A, Moreira DM, Moreno-Palacios J, Del Junco M, et al. Evaluation and comparison of urolithiasis scoring systems used in percutaneous kidney stone surgery. J Urol 2015; 193:154-9.
doi: 10.1016/j.juro.2014.07.104
pmid: 25088952
[20]
Choi SW, Bae WJ, Ha US, Hong SH, Lee JY, Kim SW, et al. Prognostic impact of stone-scoring systems after percutaneous nephrolithotomy for staghorn calculi: a single center's experience over 10 years J Endourol. 2016; 30:975e81.
[21]
Choi SW, Bae WJ, Ha US, Hong SH, Lee JY, Kim SW, et al. Prediction of stone-free status and complication rates after tubeless percutaneous nephrolithotomy: a comparative and retrospective study using three stone-scoring systems and preoperative parameters. World J Urol 2017; 35:449-57.
[22]
Al Adl AM, Mohey A, Abdel Aal A, Abu-Elnasr HAF, El Karamany T, Noureldin YA. Percutaneous nephrolithotomy outcomes based on S.T.O.N.E., GUY, CROES, and S-ReSC scoring systems: the first prospective study. J Endourol 2020; 34:1223-8.
doi: 10.1089/end.2019.0856
[23]
Khan N, Nazim SM, Farhan M, Salam B, Ather MH. Validation of S.T.O.N. E nephrolithometry and Guy's stone score for predicting surgical outcome after percutaneous nephrolithotomy. Urol Ann 2020; 12:324-30.
doi: 10.4103/UA.UA_136_19
[24]
Xun Y, Yang Y, Yu X, Li C, Lu J, Wang S. A preoperative nomogram for sepsis in percutaneous nephrolithotomy treating solitary, unilateral and proximal ureteral stones. PeerJ 2020; 8:e9435. https://doi.org/10.7717/peerj.9435.
doi: 10.7717/peerj.9435
[25]
Jiang E, Guo H, Yang B, Li P, Mishra P, Yang T, et al. Predicting and comparing postoperative infections in different stratification following PCNL based on nomograms. Sci Rep 2020; 10: 11337. https://doi.org/10.1038/s41598-020-68430-3.
doi: 10.1038/s41598-020-68430-3
pmid: 32647305
[26]
Wang J, Mi Y, Wu S, Shao H, Zhu L, Dai F. Impact factors and an efficient nomogram for predicting the occurrence of sepsis after percutaneous nephrolithotomy. BioMed Res Int 2020; 2020:6081768. https://doi.org/10.1155/2020/6081768.
[27]
Liu J, Yang Q, Lan J, Hong Y, Huang X, Yang B. Risk factors and prediction model of urosepsis in patients with diabetes after percutaneous nephrolithotomy. BMC Urol 2021; 21:74. https://doi.org/10.1186/s12894-021-00799-3.
doi: 10.1186/s12894-021-00799-3
pmid: 33910537
[28]
Gu J, Liu J, Hong Y, Feng Y, Huang X. Nomogram for predicting risk factor of urosepsis in patients with diabetes after percutaneous nephrolithotomy. BMC Anesthesiol 2022; 22:87. https://doi.org/10.1186/s12871-022-01629-1.
doi: 10.1186/s12871-022-01629-1
pmid: 35361116
[29]
Zeng H, Gao M, Chen J, Cui Y, Huang F, Zeng F, et al. Incidence and risk factors of venous thromboembolism after percutaneous nephrolithotomy: a single-center experience. World J Urol 2021; 39:3571-7.
doi: 10.1007/s00345-021-03658-w
pmid: 33725149
[30]
Sahan M, Yarimoglu S, Polat S, Nart B, Koras O, Bozkurt IH, et al. A novel nomogram and a simple scoring system for urinary leakage after percutaneous nephrolithotomy. Int Braz J Urol 2022; 48:817-27.
doi: 10.1590/S1677-5538.IBJU.2022.0091
pmid: 35839435
[31]
Jones P, Pietropaolo A, Chew BH, Somani BK. Atlas of scoring systems, grading tools, and nomograms in endourology: a comprehensive overview from the TOWER endourological society research group. J Endourol 2021; 35:1863-82.
doi: 10.1089/end.2021.0124
[32]
Elkoushy MA, Metwally AH, Noureldin YA. Implications of different nephrolithometry scoring systems on clinical practice of endourologists: an international web-based survey. Arab J Urol 2016; 14:216-22.
doi: 10.1016/j.aju.2016.04.005
[33]
Zeng G, Cai C, Duan X, Xu X, Mao H, Li X, et al. Mini percutaneous nephrolithotomy is a noninferior modality to standard percutaneous nephrolithotomy for the management of 20 mme40 mm renal calculi: a multicenter randomized controlled trial. Eur Urol 2021;79:114-21.
[34]
Abdullatif VA, Sur RL, Abdullatif ZA, Szabo SR, Abbott JE. The safety and efficacy of endoscopic combined intrarenal surgery (ECIRS) versus percutaneous nephrolithotomy (PCNL): a systematic review and meta-analysis. Adv Urol 2022; 2022: 1716554. https://doi.org/10.1155/2022/1716554.
[35]
Jiang K, Sun F, Zhu J, Luo G, Zhang P, Ban Y, et al. Evaluation of three stone-scoring systems for predicting SFR and complications after percutaneous nephrolithotomy: a systematic review and meta-analysis. BMC Urol 2019; 19:57. https://doi.org/10.1186/s12894-019-0488-y.
doi: 10.1186/s12894-019-0488-y
pmid: 31262284
[36]
Rashid AO, Fakhulddin SS. Risk factors for fever and sepsis after percutaneous nephrolithotomy. Asian J Urol 2016; 3:82-7.
doi: 10.1016/j.ajur.2016.03.001
pmid: 29264169
[37]
Sharma K, Sankhwar SN, Goel A, Singh V, Sharma P, Garg Y. Factors predicting infectious complications following percutaneous nephrolithotomy. Urol Ann 2016; 8:434-8.
doi: 10.4103/0974-7796.192105
pmid: 28057987
[38]
Kailavasan M, Berridge C, Yuan Y, Turner A, Donaldson J, Biyani CS. A systematic review of nomograms used in urolithiasis practice to predict clinical outcomes in paediatric patients. J Pediatr Urol 2022; 18:448-62.
doi: 10.1016/j.jpurol.2022.05.013
pmid: 35676182
[39]
Brown G, Juliebo-Jones P, Keller EX, De Coninck V, Beisland C, Somani BK. Current status of nomograms and scoring systems in paediatric endourology: a systematic review of literature. J Pediatr Urol 2022; 18:572-84.
doi: 10.1016/j.jpurol.2022.08.021
pmid: 36096999