|
|
|
| Defining the association between the prolonged operative time and 90-day complications in patients undergoing radical cystectomy |
Peter Hannaa,b,*( ),Joseph Zabella,Badrinath Konetyc,Christopher Warlicka ),Joseph Zabella,Badrinath Konetyc,Christopher Warlicka
|
aDepartment of Urology, University of Minnesota, Minneapolis, MN, USA
bDepartment of Urology, Aswan University, Aswan, Egypt
cDepartment of Urology, Rush University, Chicago, IL, USA |
|
|
|
|
Abstract Objective: Radical cystectomy is a complex lengthy procedure associated with postoperative morbidity. We aimed to assess the operative time (OT) in patients undergoing radical cystectomy and its impact on 90-day postoperative complications and readmission rates. Methods: The retrospective cohort study included 296 patients undergoing radical cystectomy and urinary diversion from May 2010 to December 2018 in our institution. The OT of 369 min was set as a cutoff value between short and long OT groups. The primary outcome was 90-day postoperative complication rates. Secondary outcomes were gastrointestinal recovery time, length of hospital stay, and 90-day readmission rates. Results: The overall incidence of 90-day postoperative complications was 79.7% where 43.2% representing low-grade complications according to the Clavien-Dindo classification (Grade 1 and Grade 2), and 36.5% representing high-grade complications (Grade≥3). Gastrointestinal tract and infectious complications are the most common complications in our data set (45.9% and 45.6%, respectively). On multivariable analysis, prolonged OT was significantly associated with odds of high-grade complications (odds ratio 2.340, 95% confidence interval 1.288-4.250, p=0.005). After propensity score-matched analysis, a higher incidence of major complications was identified in the long OT group 55 (51.4%) compared to 35 (32.7%) in the short OT group (p=0.006). A shorter gastrointestinal tract recovery time was noticed in the short OT group (p=0.009). Prolonged OT was associated with a higher 90-day readmission rate on univariate and multivariate analyses (p<0.001, p=0.001, respectively). Conclusion: Prolonged OT (>369 min) is associated with an increased risk of postoperative complications and readmission rates. The perception of potential postoperative complications requires careful monitoring of these patients which could translate into better operative outcomes.
|
|
Received: 13 November 2022
Available online: 20 July 2024
|
|
Corresponding Authors:
*Department of Urology, University of Minnesota, Minneapolis, MN, USA. E-mail address: phannah@umn.edu (P. Hanna).
|
|
|

| Variable | Value | | Age, year | 69 (62-76) | | Sex | | | Male | 236 (79.7) | | Female | 60 (20.3) | | Smoking | 63 (21.3) | | Weight, kg | 80.55 (70.20-93.15) | | Height, cm | 1.75 (1.70-1.80) | | BMI, kg/m2 | 26.76 (24.00-30.66) | | Charlson Comorbidity Index | | | Mild (Grades 1, 2) | 78 (26.4) | | Moderate (Grades 3, 4) | 128 (43.2) | | Severe (≥Grade 5) | 90 (30.4) | | ASA score | | | 1 | 0 (0.0) | | 2 | 50 (16.9) | | 3 | 241 (81.4) | | 4 | 5 (1.7) | | Operative approach | | | Open | 207 (69.9) | | Robotica | 89 (30.1) | | Previous abdominal surgeryb | 15 (5.1) | | History of radiotherapyb | 17 (5.8) | | Neoadjuvant chemotherapy | 122 (41.2) | | Disposition | | | Home | 203 (68.6) | | Home with nursing | 8 (2.7) | | Othersc | 85 (28.7) |
|
|
Demographic criteria for patients (n=296).
|
|
|
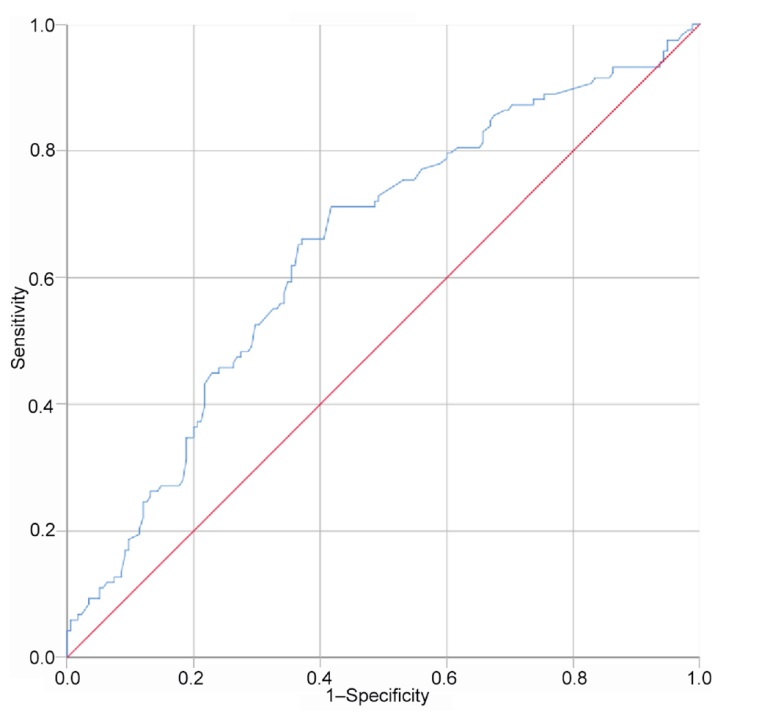
The receiver operating characteristic curve of operative time and postoperative complications to predict the cutoff value of the operative time yielding the highest area under the curve value associated with severe postoperative complications (369 min). Diagonal segments were produced by ties.
|
| Variable | Value | | Postoperative complication (Clavien-Dindo classification) | | 0 | 60 (20.3) | | Grade 1 | 7 (2.4) | | Grade 2 | 121 (40.9) | | Grade 3 | 45 (15.2) | | Grade 4 | 61 (20.6) | | Grade 5 | 2 (0.7) | | Different complicationa | | GIT | 136 (45.9) | | Ileus | 86 | | Clostridium difficile colitis | 21 | | GIT bleeding | 4 | | Gastroenteritis | 8 | | Esophagitis | 14 | | Enteric fistulas | 3 | | Infectious | 135 (45.6) | | FUO | 16 | | Abscess | 26 | | UTI | 55 | | Sepsis | 32 | | Pyelonephritis | 6 | | Surgical | 79 (26.7) | | Wound seroma | 15 | | Wound infection | 16 | | Wound dehiscence | 13 | | Abdominal fluid collection | 27 | | Re-exploratory laparotomy | 8 | | Genitourinary | 65 (22.0%) | | AKI | 52 | | Urinary leak | 7 | | Ureteral obstruction or stricture | 6 | | Cardiac | 58 (19.6) | | Arrythmia | 33 | | Myocardial infarction | 2 | | Hypotension | 13 | | Hypertension | 10 | | Pulmonary | 22 (7.4) | | Atelectasis | 4 | | Pneumonia | 11 | | Respiratory distress | 4 | | Pleural effusion | 2 | | Pneumothorax | 1 | | Bleeding | 75 (25.3) | | Anemia requiring blood transfusion | 71 | | Postoperative hematoma | 4 | | Thromboembolic | 20 (6.8) | | Deep venous thrombosis | 17 | | Pulmonary embolism | 3 | | Neurological | 33 (11.1) | | Delirium | 32 | | Transient ischemic attack | 1 | | Time to bowel movements, day | 3 (3-5) | | Length of hospital stay, day | 8 (6-11) | | 30-day readmission | 119 (40.2) | | 90-day readmission | 126 (42.6) |
|
|
Postoperative outcomes (n=296).
|
| Variable | Postoperative complication (Clavien-Dindo classification) | 90-day readmission rate | | β | Odds ratio | 95% CI | p-Valuea | β | Odds ratio | 95% CI | p-Valuea | | Lower | Upper | Lower | Upper | | Age | 0.031 | 1.031 | 1.003 | 1.060 | 0.019 | 0.023 | 1.024 | 0.997 | 1.050 | 0.075 | | Sex | 0.060 | 1.081 | 0.554 | 2.034 | 0.858 | 0.543 | 1.722 | 0.911 | 3.254 | 0.094 | | Smoking | ?0.074 | 0.929 | 0.693 | 1.245 | 0.622 | ?0.102 | 1.026 | 0.772 | 1.361 | 0.862 | | BMI | 0.059 | 1.061 | 1.011 | 1.113 | 0.016 | 0.020 | 1.020 | 0.975 | 1.068 | 0.386 | | CCI | 0.190 | 1.209 | 1.026 | 1.425 | 0.023 | 0.091 | 1.095 | 0.935 | 1.282 | 0.260 | | Operative approach | 0.480 | 1.616 | 0.884 | 3.211 | 0.119 | 0.500 | 1.649 | 0.929 | 2.926 | 0.068 | | OTb | ?0.85 | 2.340 | 1.288 | 4.250 | 0.005 | 0.962 | 2.617 | 1.503 | 4.559 | 0.001 | | EBL | 0.001 | 1.000 | 0.999 | 1.000 | 0.657 | 0.001 | 1.000 | 1.000 | 1.001 | 0.670 | | Surgical experience | 0.080 | 1.143 | 0.667 | 1.734 | 0.739 | ?0.017 | 0.962 | 0.614 | 1.509 | 0.940 | | Diversion type | 0.120 | 1.209 | 0.570 | 2.253 | 0.721 | ?0.775 | 0.440 | 0.231 | 0.835 | 0.020 | | ERAS | 0.306 | 1.358 | 0.804 | 2.292 | 0.252 | 0.148 | 1.160 | 0.703 | 1.914 | 0.561 |
|
|
Multivariable logistic regression for postoperative complications (low grade or high grade) and the incidence of 90-day readmission rates.
|
|
|
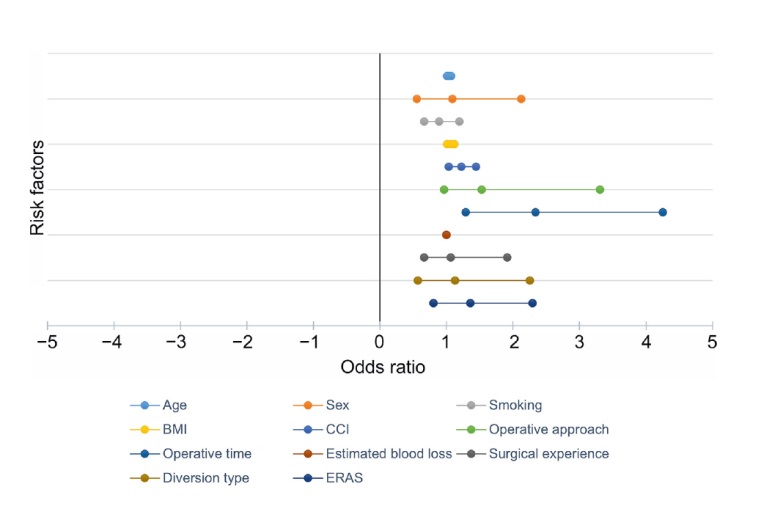
Forest plot showing multivariate analysis of potential risk factors of major postoperative complications. Odds ratios are shown with 95% confidence intervals for the age, sex, smoking, BMI, CCI, operative approach, operative time (369 min as the cutoff value), EBL, surgical experience, type of diversion, and ERAS as possible predictors for development of postoperative complications. BMI, body mass index; CCI, Charlson Comorbidity Index; EBL, estimated blood loss; ERAS, enhanced recovery after surgery protocol.
|
| Outcome | Operative time | p-Valuea | | ≤369 min (n=107) | >369 min (n=107) | | Postoperative complication (Clavien-Dindo classification) | | | 0.006 | | Low grade (≤2) | 72 (67.3) | 52 (48.6) | | | High grade (≥3) | 35 (32.7) | 55 (51.4) | | | Complication categoryb | | | | | Infectious | 25 (23.4) | 44 (41.1) | 0.005 | | GIT | 43 (40.2) | 46 (43.0) | 0.700 | | Surgical | 18 (16.8) | 32 (29.9) | 0.020 | | Genitourinary | 16 (15.0) | 34 (31.8) | 0.004 | | Cardiac | 18 (16.8) | 26 (24.3) | 0.200 | | Respiratory | 6 (5.6) | 7 (6.5) | 0.800 | | Bleeding | 27 (25.2) | 29 (27.1) | 0.800 | | Thromboembolic | 8 (7.5) | 6 (5.6) | 0.600 | | Neurological | 18 (16.8) | 10 (9.3) | 0.100 | | ERAS | 57 (53.3) | 48 (44.9) | 0.200 | | Length of hospital stay, day | 9 (6-12) | 8 (7-11) | 0.600 | | Time to bowel movements, day | 4 (3-6) | 5 (4-6) | 0.009 | | 30-day readmission | 33 (30.8) | 58 (54.2) | 0.001 | | 90-day readmission | 34 (31.8) | 60 (56.1) | <0.001 |
|
|
Postoperative outcomes between matched groups based on operative time after propensity score-matched analysis.
|
| [1] |
Cornellà N, Sancho J, Sitges-Serra A. Short and long-term outcomes after surgical procedures lasting for more than six hours. Sci Rep 2017; 7:9221. https://doi.org/10.1038/s41598-017-09833-7
doi: https://doi.org/10.1038/s41598-017-09833-7
pmid: 28835620
|
| [2] |
Shabsigh A, Korets R, Vora KC, Brooks CM, Cronin AM, Savage C, et al. Defining early morbidity of radical cystectomy for patients with bladder cancer using a standardized reporting methodology. Eur Urol 2009; 55:164-74.
|
| [3] |
Cookson MS, Chang SS, Wells N, Parekh DJ, Smith JA. Complications of radical cystectomy for nonmuscle invasive disease: comparison with muscle invasive disease. J Urol 2003; 169:101e4.
|
| [4] |
Frazier HA, Robertson JE, Paulson DF. Complications of radical cystectomy and urinary diversion: a retrospective review of 675 cases in 2 decades. J Urol 1992; 148:1401e5.
|
| [5] |
Hollenbeck BK, Miller DC, Taub D, Dunn RL, Khuri SF, Henderson WG, et al. Identifying risk factors for potentially avoidable complications following radical cystectomy. J Urol 2005; 174(4 Pt 1):1231e7. https://doi.org/10.1097/01.ju.-0000173923.35338.99
doi: https://doi.org/10.1097/01.ju.-0000173923.35338.99
|
| [6] |
Konety BR, Allareddy V, Herr H. Complications after radical cystectomy: analysis of population-based data. Urology 2006; 68:58-64.
|
| [7] |
Albersheim J, Sathianathen Niranjan J, Zabell J, Renier J, Bailey T, Hanna P, et al. Skeletal muscle and fat mass indexes predict discharge disposition after radical cystectomy. J Urol 2019; 202:1143e9.
|
| [8] |
Shah N, Hamilton M. Clinical review: can we predict which patients are at risk of complications following surgery? Crit Care 2013; 17:226. https://doi.org/10.1186/cc11904
doi: https://doi.org/10.1186/cc11904
|
| [9] |
Visser A, Geboers B, Gouma DJ, Goslings JC, Ubbink DT. Predictors of surgical complications: a systematic review. Surgery 2015:15858-65.
|
| [10] |
Tsuchida T, Takesue Y, Ichiki K, Uede T, Nakajima K, Ikeuchi H, et al. Influence of peri-operative hypothermia on surgical site infection in prolonged gastroenterological surgery. Surg Infect 2016; 17:570e6.
|
| [11] |
Fogarty BJ, Khan K, Ashall G, Leonard AG. Complications of long operations: a prospective study of morbidity associated with prolonged operative time (> 6 h). Br J Plast Surg 1999; 52:33e6.
|
| [12] |
Harrison OJ, Smart NJ, White P, Brigic A, Carlisle ER, Allison AS, et al. Operative time and outcome of enhanced recovery after surgery after laparoscopic colorectal surgery. J Soc Laparoendosc Surg 2014; 18:265-72.
|
| [13] |
Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg 2009; 250:187-96.
|
| [14] |
Canet J, Gallart L, Gomar C, Paluzie G, Vallès J, Castillo J, et al. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology 2010; 113:1338-50.
|
| [15] |
Pessaux P, Msika S, Atalla D, Hay JM, Flamant Y, French Associations for Surgical Research. Risk factors for postoperative infectious complications in noncolorectal abdominal surgery: a multivariate analysis based on a prospective multicenter study of 4718 patients. Arch Surg 2003; 138:314-24.
|
| [16] |
Daley BJ, Cecil W, Clarke PC, Cofer JB, Guillamondegui OD. How slow is too slow? Correlation of operative time to complications: an analysis from the Tennessee surgical quality collaborative. J Am Coll Surg 2015; 220:550e8.
|
| [17] |
Bochner BH, Dalbagni G, Sjoberg DD, Silberstein J, Keren Paz GE, Donat SM, et al. Comparing open radical cystectomy and robot-assisted laparoscopic radical cystectomy: a randomized clinical trial. Eur Urol 2015; 67:1042-50.
|
| [18] |
Mastroianni R, Ferriero M, Tuderti G, Anceschi U, Bove AM, Brassetti A, et al. Open radical cystectomy versus robotassisted radical cystectomy with intracorporeal urinary diversion: early outcomes of a single-center randomized controlled trial. J Urol 2022; 207:982-92.
|
| [19] |
Mastroianni R, Arvizo MAO, Torregiani G, Simone G. Robotassisted vs. open radical cystectomy: randomized controlled trials lights and shadows. J Urol 2023; 209:460e1.
|
| [20] |
Boyd-Carson H, Gana T, Lockwood S, Murray D, Tierney GM. A review of surgical and peri-operative factors to consider in emergency laparotomy care. Anaesthesia 2020; 75(Supp.1):e75-82. https://doi.org/10.1111/anae.14821
doi: https://doi.org/10.1111/anae.14821
|
| [21] |
Jakobson T, Karjagin J, Vipp L, Padar M, Parik AH, Starkopf L, et al. Postoperative complications and mortality after major gastrointestinal surgery. Medicina 2014; 50:111e7.
|
| [22] |
Cheng H, Clymer JW, Po-Han Chen B, Sadeghirad B, Ferko NC, Cameron CG, et al. Prolonged operative duration is associated with complications: a systematic review and meta-analysis. J Surg Res 2018; 229:134-44.
|
| [23] |
Procter LD, Davenport DL, Bernard AC, Zwischenberger JB. General surgical operative duration is associated with increased risk-adjusted infectious complication rates and length of hospital stay. J Am Coll Surg 2010; 210:60-65.e1-2. https://doi.org/10.1016/j.jamcollsurg.2009.09.034
doi: https://doi.org/10.1016/j.jamcollsurg.2009.09.034
|
| [24] |
Liverani A, Chiarot M, Bezzi M, Angelini L. [Is surgery duration really a complication factor?]. Minerva Chir 1994;49 9:747-50. [Article in Italian].
|
| [25] |
Dexter SPL, Martin IG, Marton J, McMahon MJ. Long operation and the risk of complications from laparoscopic cholecystectomy. Br J Surg 1997; 84:464e6.
|
| [26] |
Lorentz CA, Gilbert K, Alemozaffar M, Patil D, Filson CP. Risk of readmission after uncomplicated hospitalization after radical cystectomy. Clin Genitourin Cancer 2018; 16:e705-10. https://doi.org/10.1016/j.clgc.2018.01.004
doi: https://doi.org/10.1016/j.clgc.2018.01.004
|
| [27] |
Mastroianni R, Tuderti G, Anceschi U, Bove AM, Brassetti A, Ferriero M, et al. Comparison of patient-reported health-related quality of life between open radical cystectomy and robotassisted radical cystectomy with intracorporeal urinary diversion: interim analysis of a randomised controlled trial. Eur Urol Focus 2022; 8:465-71.
|
| [28] |
Giglio M, Biancofiore G, Corriero A, Romagnoli S, Tritapepe L, Brienza N, et al. Perioperative goal-directed therapy and postoperative complications in different kind of surgical procedures: an updated meta-analysis. J Anesth Analg Crit Care 2021; 1:26. https://doi.org/10.1186/s44158-021-00026-3
doi: https://doi.org/10.1186/s44158-021-00026-3
|
| [29] |
Lombardo R, Mastroianni R, Tuderti G, Ferriero M, Brassetti A, Anceschi U, et al. Benchmarking PASADENA consensus along the learning curve of robotic radical cystectomy with intracorporeal neobladder: CUSUM based assessment. J Clin Med 2021; 10:5969. https://doi.org/10.3390/jcm10245969
doi: https://doi.org/10.3390/jcm10245969
|
| [30] |
Tuderti G, Mastroianni R, Brassetti A, Bove AM, Misuraca L, Anceschi U, et al. Robot-assisted radical cystectomy with intracorporeal neobladder: impact of learning curve and longterm assessment of functional outcomes. Minerva Urol Nephrol 2021; 73:754-62.
|
| [1] |
Jonathan Rosenfeld, Devin Boehm, Aidan Raikar, Devyn Coskey, Matthew Lee, Emily Ji, Ziho Lee. A review of complications after ureteral reconstruction[J]. Asian Journal of Urology, 2024, 11(3): 348-356. |
| [2] |
Eric Edison, Giorgio Mazzon, Vimoshan Arumuham, Simon Choong. Prevention of complications in endourological management of stones: What are the basic measures needed before, during, and after interventions?[J]. Asian Journal of Urology, 2024, 11(2): 180-190. |
| [3] |
Ahmed M. Harraz, Ahmed Elkarta, Mohamed H. Zahran, Ahmed Mosbah, Atallah A. Shaaban, Hassan Abol-Enein. The impact of chemotherapy-naïve open radical cystectomy delay and perioperative transfusion on the recurrence-free survival: A perioperative parameters-based nomogram[J]. Asian Journal of Urology, 2024, 11(2): 294-303. |
| [4] |
Vanessa A. Lukas, Rahul Dutta, Ashok K. Hemal, Matvey Tsivian, Timothy E. Craven, Nicholas A. Deebel, David D. Thiel, Ram Anil Pathak. Impact of pre- and peri-operative risk factors on length of stay and hospital readmission following minimally-invasive partial nephrectomy[J]. Asian Journal of Urology, 2024, 11(1): 72-79. |
| [5] |
Praanjal Gupta, Ramanitharan Manikandan, Lalgudi Narayanan Dorairajan, Kodakattil Sreenivasan Sreerag, Sidhartha Kalra, Swapnil Singh Kushwaha. Can we predict the incidence of high-grade Clavien-Dindo complications in patients with forgotten encrusted stents undergoing endourologic management?[J]. Asian Journal of Urology, 2024, 11(1): 99-104. |
| [6] |
Jordan M. Rich, Shivaram Cumarasamy, Daniel Ranti, Etienne Lavallee, Kyrollis Attalla, John P. Sfakianos, Nikhil Waingankar, Peter N. Wiklund, Reza Mehrazin. Contemporary outcomes of patients undergoing robotic-assisted radical cystectomy: A comparative analysis between intracorporeal ileal conduit and neobladder urinary diversions[J]. Asian Journal of Urology, 2023, 10(4): 446-452. |
| [7] |
Brianna Ruch, Deki Tsering, Chandra Bhati, Dhiren Kumar, Muhammad Saeed, Seung Duk Lee, Aamir Khan, Daisuke Imai, David Bruno, Marlon Levy, Adrian Cotterell, Amit Sharma. Right versus left fully robotic live donor nephrectomy and open kidney transplantation: Does the laterality of the donor kidney really matter?[J]. Asian Journal of Urology, 2023, 10(4): 453-460. |
| [8] |
Angelo Territo, Alessandro Uleri, Andrea Gallioli, Josep Maria Gaya, Paolo Verri, Giuseppe Basile, Alba Farré, Alejandra Bravo, Alessandro Tedde, Óscar Rodríguez Faba, Joan Palou, Alberto Breda. Robot-assisted oncologic pelvic surgery with Hugo™ robot-assisted surgery system: A single-center experience[J]. Asian Journal of Urology, 2023, 10(4): 461-466. |
| [9] |
Giorgio Mazzon,Simon Choong,Antonio Celia. Stone-scoring systems for predicting complications in percutaneous nephrolithotomy: A systematic review of the literature[J]. Asian Journal of Urology, 2023, 10(3): 226-238. |
| [10] |
Stefano Alba,Deborah Fimognari,Fabio Crocerossa,Luigi Ascalone,Carmine Pullano,Fernando Chiaravalloti,Francesco Chiaradia,Umberto Carbonara,Matteo Ferro,Ottavio de Cobelli,Vincenzo Pagliarulo,Giuseppe Lucarelli,Michele Battaglia,Rocco Damiano,Francesco Cantiello. Neuraxial anesthesia versus general anesthesia in patients undergoing three-dimensional laparoscopic radical prostatectomy: Preliminary results of a prospective comparative study[J]. Asian Journal of Urology, 2023, 10(3): 329-336. |
| [11] |
Erhan Demirelli,Ercan Öğreden,Cemil Bayraktar,Alptekin Tosun,Ural Oğuz. The effect of perirenal fat stranding on infectious complications after ureterorenoscopy in patients with ureteral calculi[J]. Asian Journal of Urology, 2022, 9(3): 307-312. |
| [12] |
Athanasios Tsitsiflis,Yiannis Kiouvrekis,Georgios Chasiotis,Georgios Perifanos,Stavros Gravas,Ioannis Stefanidis,Vassilios Tzortzis,Anastasios Karatzas. The use of an artificial neural network in the evaluation of the extracorporeal shockwave lithotripsy as a treatment of choice for urinary lithiasis[J]. Asian Journal of Urology, 2022, 9(2): 132-138. |
| [13] |
Christa Babst,Thomas Amiel,Tobias Maurer,Sophie Knipper,Lukas Lunger,Robert Tauber,Margitta Retz,Kathleen Herkommer,Matthias Eiber,Gunhild von Amsberg,Markus Graefen,Juergen Gschwend,Thomas Steuber,Matthias Heck. Cytoreductive radical prostatectomy after chemohormonal therapy in patients with primary metastatic prostate cancer[J]. Asian Journal of Urology, 2022, 9(1): 69-74. |
| [14] |
Marcio Covas Moschovas,Kulthe Ramesh Seetharam Bhat,Cathy Jenson,Vipul R. Patel,Gabriel Ogaya-Pinies. Robtic-assisted radical cystectomy: Literature review[J]. Asian Journal of Urology, 2021, 8(1): 14-19. |
| [15] |
Hugo Otaola-Arca,Rafael Coelho,Vipul R. Patel,Marcelo Orvieto. Totally intracorporeal robot-assisted urinary diversion for bladder cancer (Part 1). Review and detailed characterization of ileal conduit and modified Indiana pouch[J]. Asian Journal of Urology, 2021, 8(1): 50-62. |
|
|
|
|