|
|
|
| An evaluation of ureteral diameter ratio and vesicoureteral reflux index in the treatment of primary vesicoureteral reflux |
Yusuf Atakan Baltrak*( ),Nebil Akdoğan,Mutlu Değer,Volkan Izol,Ibrahim Atilla Aridoğan,Nihat Satar ),Nebil Akdoğan,Mutlu Değer,Volkan Izol,Ibrahim Atilla Aridoğan,Nihat Satar
|
| Division Pediatric Urology, Department of Urology, Medical Faculty, Cukurova University, Adana, Turkey |
|
|
|
|
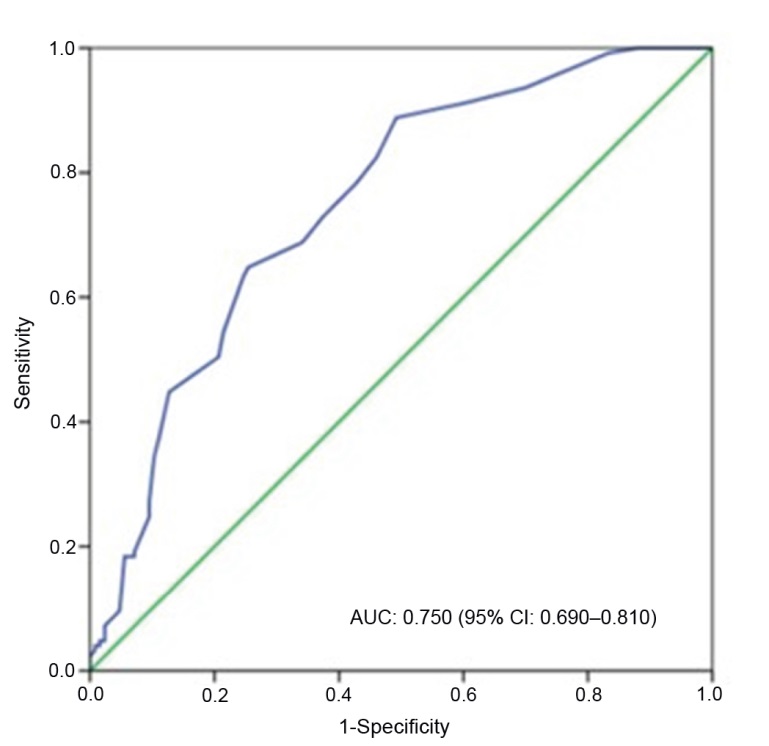
Abstract Objective: Vesicoureteral reflux (VUR) index is a simple, validated tool that reliably predicts significant improvement and spontaneous resolution of primary reflux in children. The aim of this study was to evaluate and compare the ureter diameter ratio (UDR) and VUR index (VURx) of patients treated with endoscopic injection (EI) and ureteroneocystostomy (UNC) methods in the pediatric age group due to primary VUR. Methods: Patients under the age of 18 years old who underwent EI and UNC with the diagnosis of primary VUR between January 2011 and September 2021 were determined as the participants. The UDR was assessed using voiding cystourethrography, and the VURx score was determined prior to treatment based on hospital records included in the study. Results: A total of 255 patients, 60 (23.5%) boys and 195 (76.5%) girls, with a mean age of 76.5 (range 13.0-204.0) months, were included in the study. EI was applied to 130 (51.0%) patients and UNC was applied to 125 (49.0%) patients due to primary VUR. The optimum cut-off for the distal UDR was obtained as 0.17 with sensitivity and specificity of 73.0% and 63.0%, respectively. The positive and negative predictive values were 66.0% and 70.0%, respectively. Conclusion: When the UDR and VURx score are evaluated together for the surgical treatment of primary VUR in the pediatric age group, it is thought that it may be useful in predicting the clinical course of the disease and evaluating surgical treatment options.
|
|
Received: 16 July 2022
Available online: 20 July 2024
|
|
Corresponding Authors:
*E-mail address: dratakanbaltrak@gmail.com (Y.A. Baltrak).
|
|
|

| Variable | Score | | Gender | | | Girl | 1 | | Boy | 0 | | VUR timing | | | Early-moderate filling | 3 | | Late filling | 2 | | Voiding phase | 1 | | Ureteral abnormality | | | Yes | 1 | | No | 0 | | VUR incidence | | | Grades I-III | 0 | | Grades IV-V | 1 |
|
|
The demographic information of the patients and VURx.
|
| Variable | EI (n=130) | UNC (n=125) | p-Value | | Age, month | 68.0 (13.0-190.0) | 72.0 (25.0-204.0) | 0.835 | | Distribution age | | | 0.801 | | ≤24 months | 18 (13.8) | 0 | | | >24 months | 112 (86.2) | 125 (100.0) | | | Height, cm | 116.1±21.5 | 112.5±22.5 | 0.191 | | Weight, kg | 28.5±12.9 | 24.6±11.9 | 0.120 | | BMI, kg/m2 | 20.07 (11.11-21.67) | 16.64 (12.10-19.67) | 0.175 | | Gender | | | 0.110 | | Boy | 36 (27.7) | 24 (19.2) | | | Girl | 94 (72.3) | 101 (80.8) | | | Hemoglobin, g/dL | 11.9±1.3 | 12.2±1.5 | 0.139 | | Blood urea nitrogen, mg/dL | 12.9±8.1 | 14.2±8.2 | 0.160 | | Blood creatinine, mg/dL | 0.5±0.5 | 0.5±0.4 | 0.958 | | Renal scarring incidence | | | 0.428 | | No | 73 (56.2) | 64 (51.2) | | | Yes | 57 (43.8) | 61 (48.8) | | | Kidney function distribution, % | | | | | Right kidney | 51.6±20.1 | 49.6±21.3 | 0.610 | | Left kidney | 48.4±20.1 | 50.1±21.2 | 0.748 |
|
|
Findings of the patients who had EI and UNC because of primary vesicoureteral reflux.
|
| Variable | EI (n=130) | UNC (n=125) | p-Value | | Location | | | <0.001 | | Right | 36 (27.7) | 15 (12.0) | | | Left | 54 (41.5) | 26 (20.8) | | | Bilateral | 40 (30.8) | 84 (67.2) | | | Bilateral reflux | | | <0.001 | | No | 90 (69.2) | 41 (32.8) | | | Yes | 40 (30.8) | 84 (67.2) | | | Constipation | | | 0.093 | | No | 107 (82.3) | 92 (73.6) | | | Yes | 23 (17.7) | 33 (26.4) | | | Urinary incontinencea | | | <0.001 | | No | 96 (75.0) | 33 (26.8) | | | Yes | 32 (25.0) | 90 (73.2) | | | Reflux incidence | | | <0.001 | | Low-grade | 88 (67.7) | 57 (45.6) | | | High-grade | 42 (32.3) | 68 (54.4) | | | Reflux time | | | 0.138 | | Voiding phase | 73 (56.2) | 55 (44.0) | | | Filling phase | 57 (43.8) | 70 (56.0) | |
|
|
Comparative results of EI and UNC groups.
|
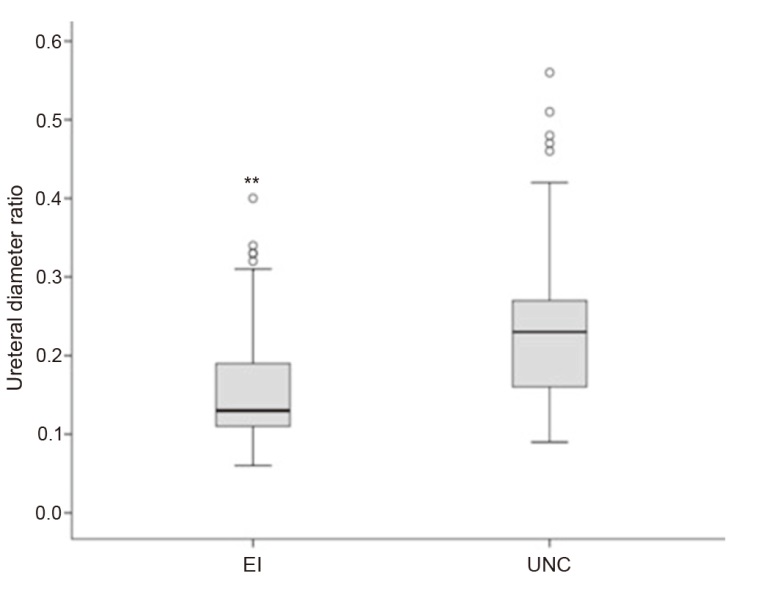
| Variable | EI | UNC | | Grades I-III | Grades IV-V | p-Value | Grades I-III | Grades IV-V | p-Value | | VURx score | 2.4±0.7 | 3.5±0.7 | <0.001 | 2.6±0.7 | 3.9±0.7 | <0.001 | | UDR | 0.14±0.06 | 0.21±0.09 | <0.001 | 0.19±0.09 | 0.26±0.08 | <0.001 | | UDR | | | <0.001 | | | <0.001 | | <0.17 | 67 (76.1) | 14 (33.3) | | 27 (47.4) | 7 (10.3) | | | ≥0.17 | 21 (23.9) | 28 (66.7) | | 30 (52.6) | 61 (89.7) | |
|
|
VURx score and UDR comparison between EI and UNC groups.
|
| Variable | OR (95% CI) | p-Value | | Age (>24 months) | 0.99 (0.37-2.64) | 0.981 | | Gender (girl) | 2.09 (0.87-5.03) | 0.099 | | Bilateral reflux | 4.90 (2.45-9.79) | <0.001 | | Urinary incontinence | 8.88 (4.45-17.76) | <0.001 | | UDR (≥0.17) | 5.53 (2.62-11.66) | <0.001 | | VUR (high-grade) | 1.67 (0.73-3.81) | 0.223 | | Constipation | 1.06 (0.46-2.45) | 0.888 | | Reflux time (filling) | 0.51 (0.23-1.14) | 0.100 |
|
|
Multivariate logistic regression analysis results of the patients who had UNC after EI (n=21).
|

|
|
The box plot of ureteral diameter ratio in UNC and EI groups. UNC, ureteroneocystostomy; EI, endoscopic injection. ?? p<0.001.
|
|
|
The receiver operating characteristic curve analysis of ureter diameter ratio predicts ureteroneocystostomy AUC. AUC, area under the curve; CI, confidence interval.
|
| [1] |
Stull TL, LiPuma JJ. Epidemiology and natural history of urinary tract infections in children. Med Clin 1991; 75:287-97.
|
| [2] |
Stephens FD, Lenaghan D. The anatomical basis and dynamics of vesicoureteral reflux. J Urol 1962; 87:669-80.
|
| [3] |
Cooper CS, Birusingh KK, Austin JC, Knudson MJ, Brophy PD. Distal ureteral diameter measurement objectively predicts vesicoureteral reflux outcome. J Pediatr Urol 2013; 9:99-103.
|
| [4] |
Swanton AR, Arlen AM, Alexander SE, Kieran K, Storm DW, Cooper CS. Inter-rater reliability of distal ureteral diameter ratio compared to grade of VUR. J Pediatr Urol 2017; 13:207. e1e5. https://doi.org/10.1016/j.jpurol.2016.10.021
doi: https://doi.org/10.1016/j.jpurol.2016.10.021
|
| [5] |
Bio?i? M, Todori? J, Budimir D, Cvitkovi? Roi? A, Pogoreli? Z, Juri? I, et al. Endoscopic treatment of vesicoureteral reflux in children with subureteral dextranomer/hyaluronic acid injection: a single-centre, 7-year experience. Can J Surg 2012; 55:301e6.
|
| [6] |
Cooper CS, Birusingh KK, Austin JC, Knudson MJ, Brophy PD. Distal ureteral diameter measurement objectively predicts vesicoureteral reflux outcome. J Pediatr Urol 2013; 9:99-103.
|
| [7] |
Estrada CR Jr, Passerotti CC, Graham DA, Peters CA, Bauer SB, Diamond DA, et al. Nomograms for predicting annual resolution rate of primary vesicoureteral reflux: results from 2462 children. J Urol 2009; 182:1535-41.
|
| [8] |
Arlen AM, Alexander SE, Wald M, Cooper CS. Computer model predicting break through febrile urinary tract infection in children with primary vesicoureteral reflux. J Pediatr Urol 2016; 12:e1e5. https://doi.org/10.1016/j.jpurol.2016.03.005
doi: https://doi.org/10.1016/j.jpurol.2016.03.005
|
| [9] |
Helmy T, Sharaf D, AbdelHalim A, Hafez A, Dawaba M. Can distal ureteral diameter predict reflux resolution after endoscopic injection? Urology 2015; 85:896e9.
|
| [10] |
Arlen AM, Kirsch AJ, Leong T, Cooper CS. Validation of the ureteral diameter ratio for predicting early spontaneous resolution of primary vesicoureteral reflux. J Pediatr Urol 2017; 13:e1-6. https://doi.org/10.1016/j.jpurol.2017.01.012
doi: https://doi.org/10.1016/j.jpurol.2017.01.012
|
| [11] |
Mendez R, Somoza I, Tellado MG, Liras J, Sanchez A, Pais E, et al. Predictive value of clinical factors for successful endoscopic correction of primary vesicoureteral reflux grades IIIeIV. J Pediatr Urol 2006; 2:545-50.
|
| [12] |
Cooper CS, Alexander SE, Kieran K, Storm DW. Utility of the distal ureteral diameter on VCUG for grading VUR. J Pediatr Urol 2015; 11:183. e1-6. https://doi.org/10.1016/j.jpurol.2015.04.009
doi: https://doi.org/10.1016/j.jpurol.2015.04.009
|
| [13] |
Arlen AM, Broderick KM, Huen KH, Leong T, Scherz HC, Kirsch AJ. Temporal pattern of vesicoureteral reflux on voiding cysto urethrogram correlates with dynamic endoscopic hydro distention grade of the ureteral orifice. J Urol 2014; 192:1503e7.
|
| [14] |
Kirsch AJ, Arlen AM, Leong T, Merriman LS, Herrel LA, Scherz HC, et al. Vesicoureteral reflux index (VURx): a novel tool to predict primary reflux improvement and resolution in children less than 2 years of age. J Pediatr Urol 2014; 10:1249-54.
|
| [15] |
Han DS, Cambareri G, Alagiri M, Chiang G. Reflux timing is a predictor of successful endoscopic treatment of vesicoureteral reflux. Urology 2019; 124:237-40.
|
| [16] |
Lee JN, Lee SM, Ha YS, Kim BS, Kim HT, Kim TH, et al. VUR timing on VCUG as a predictive factor of VUR resolution after endoscopic therapy. J Pediatr Urol 2016; 12:e16. https://doi.org/10.1016/j.jpurol.2016.04.002
doi: https://doi.org/10.1016/j.jpurol.2016.04.002
|
| [17] |
Garcia-Roig M, Ridley DE, Mc CrackenC, Arlen AM, Cooper CS, Kirsch AJ. Vesicoureteral reflux index: predicting primary vesicoureteral reflux resolution in clinic diagnosed after age 24 months. J Urol 2017; 197:1150e7.
|
| [18] |
Vaz GT, Vasconcelos MM, Oliveira EA, Ferreira AL, Magalh?es PG, Silva FM, et al. Prevalence of lower urinary tract symptoms in school-age children. Pediatr Nephrol 2012; 27:597-603.
|
| [19] |
Conway PH, Cnaan A, Zaoutis T, Henry BV, Grundmeier RW, Keren R. Recurrent urinary tract infections in children: risk factors and association with prophylactic antimicrobials. JAMA 2007; 298:179-86.
|
| [20] |
Van Gool JD, Hj?lma°s K, Tamminen-M?bius T, Olbing H. Historical clues to the complex of dysfunctional voiding, urinary tract infection and vesicoureteral reflux. The ?nternational reflux study in children. J Urol 1992; 148:1699-702.
|
| [21] |
Yang S, Chua ME, Bauer S, Wright A, Brandstr?m P, Hoebeke P, et al. Diagnosis and management of bladder bowel dysfunction in children with urinary tract infections: a position statement from the International Children’s Continence Society. Pediatr Nephrol 2018; 33:2207-19.
|
| [22] |
Mattoo TK, Chesney RW, Greenfield SP, Hoberman A, Keren R, Mathews R, et al. RIVUR trial investigators. Renal scarring in the randomized intervention for children with vesicoureteral reflux (RIVUR) trial. Clin J Am Soc Nephrol 2016; 11:54-61.
|
| [23] |
L?ckgren G, Cooper CS, Neveus T, Kirsch AJ. Management of vesicoureteral reflux: what have we learned over the last 20 years? Front Pediatr 2021; 9:650326. https://doi.org/10.3389/fped.2021.650326
doi: https://doi.org/10.3389/fped.2021.650326
|
| [24] |
RIVUR trial investigators; Hoberman A, Greenfield SP, Mattoo TK, Keren R, Mathews R, Pohl HG, et al. Antimicrobial prophylaxis for children with vesicoureteral reflux. N Engl J Med 2014; 370:2367-76.
|
| [1] |
Seyed Alaeddin Asgari,Afshin Safaei-Asl,Mandana Mansour-Ghanaie,Seyed Mohammad Asgari,Asghar Faryabi,Mohammadreza Bazli,Faezeh Emami Sigaroudi,Seyed Ahmad Naseri Alavi. Modified unilateral periureteral injection technique in the treatment of patients with high-grade vesicoureteral reflux: A study of primary findings[J]. Asian Journal of Urology, 2023, 10(1): 96-100. |
| [2] |
Brian D. Duty, John M. Barry. Diagnosis and management of ureteral complications following renal transplantation[J]. Asian Journal of Urology, 2015, 2(4): 202-207. |
|
|
|
|