|
|
|
| Genitourinary manifestations of Lynch syndrome in the urological practice |
Chiara Lonatia,b,*( ),Claudio Simeonea,Nazareno Suardia,Philippe E. Spiessc,Andrea Necchid,e,Marco Moschinif ),Claudio Simeonea,Nazareno Suardia,Philippe E. Spiessc,Andrea Necchid,e,Marco Moschinif
|
aUrology Unit, ASST Spedali Civili di Brescia, Department of Medical and Surgical Specialties, Radiological Science and Public Health, University of Brescia, Brescia, Italy
bDepartment of Urology, Luzerner Kantonsspital, Lucerne, Switzerland
cDepartment of Genitourinary Oncology, H. Lee Moffitt Cancer Center and Research Institute, Tampla, FL, USA
dUniversity Vita-Salute San Raffaele, Milan, Italy
eDepartment of Medical Oncology, IRCCS San Raffaele Hospital and Scientific Institute, Milan, Italy
fDivision of Experimental Oncology/Unit of Urology, Urological Research Institute, IRCCS Ospedale San Raffaele, Milan, Italy |
|
|
|
|
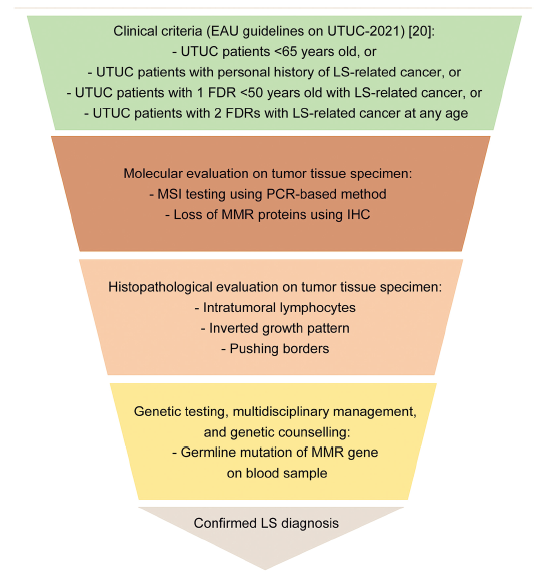
Abstract Objective: Lynch syndrome (LS) is an autosomal dominant hereditary disorder resulting from germline mutation in at least one of the four mismatch repair genes or in EPCAM gene. From a clinical perspective, LS patients exhibit an increased predisposition to multiple primary malignancies and early age of onset compared to general population. We aimed to provide a comprehensive overview of all the genitourinary manifestations of LS, focusing on incidence, diagnosis, clinical features, therapeutic strategies, and screening protocols. Methods: Previous literature was assessed through Medline, Scopus, and Google Scholar databases. A narrative review of the most relevant articles from January 1996 to June 2021 on urological manifestations of LS was provided. Results: In the LS tumor spectrum, upper tract urothelial carcinoma (UTUC) represents the third most frequent malignancy, and the first most common cancer in the urological field, with an approximately 14-fold increased risk of developing UTUC compared to general population. LS diagnosis among patients experiencing UTUC as first malignancy is a step-by-step process, including (i) clinical criteria, (ii) molecular testing, and (iii) genetic testing to confirm the hereditary disorder. The current European Association of Urology (EAU) guidelines recommend to perform molecular testing among UTUC patients under 65 years old, or UTUC patients with personal history of LS-related tumor, or UTUC patients with one first-degree relative under the age of 50 years with LS-related tumor, or UTUC patients with two first-degree relatives with LS-related tumor regardless of age of onset. Newly diagnosed LS patients should be referred to a multidisciplinary management, including gastroenterologists and gynecologists. Finally, considering the increased risk of metachronous recurrence, treatments other than radical nephroureterectomy may be a valuable therapeutic alternative. Whether urological malignancies other than UTUC should be included in the LS tumor spectrum is still controversial. Conclusion: Considering the strict association between UTUC and LS, we believe that the urologist should recognize patients at increased risk for hereditary disease according to current EAU clinical criteria and address them to a comprehensive diagnostic algorithm, including molecular evaluation and genetic testing. To date, literature lacks clear evidence regarding the role of LS in developing bladder cancer, prostate cancer, or renal cell carcinoma, and current data are still inconclusive, highlighting the urgent need for further studies.
|
|
Received: 08 December 2021
Available online: 20 October 2022
|
|
Corresponding Authors:
Chiara Lonati
E-mail: chiara.lonati@libero.it
|
|
|
|
|
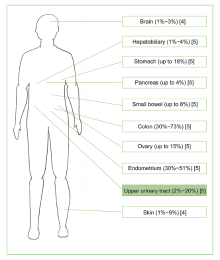
Sites at increased risk of developing primary malignancies among Lynch syndrome patients.
|

|
|
Flow chart for diagnosis of LS in patients experiencing UTUC without known DNA MMR gene mutation. EAU, European Association of Urology; UTUC, upper tract urothelial carcinoma; LS, Lynch syndrome; FDR, first-degree relative; MSI, microsatellite instability; PCR, polymerase chain reaction; MMR, mismatch repair; IHC, immunohistochemistry.
|

| Clinical criteria | Description | | Amsterdam I criteria (1991)[58] | All the following criteria:
1.At least three relatives with colorectal cancer
2.One should be a first-degree relative of the other two
3.At least two successive generations should be affected
4.At least one colorectal cancer should be diagnosed before the age of 50 years
5.Familial adenomatous polyposis should be excluded
6.Tumors should be verified by pathological examination | | Amsterdam II criteria (1999)[15] | All the following criteria:
1.At least three relatives with LS-related cancer
2.One should be a first-degree relative of the other two
3.At least two successive generations should be affected
4.At least one LS-related cancer (including colorectum, endometrium, small bowel, ureter, or renal pelvis) should be diagnosed <50 years
5.Familial adenomatous polyposis should be excluded
6.Tumors should be verified by pathological examination | | Revised Bethesda guidelines (2004)[16] | Any of the following criteria:
1.Colorectal cancer diagnosed <50 years
2.Presence of synchronous or metachronous colorectal cancer or other LS-related cancer (including colorectum, endometrium, stomach, ovary, pancreas, ureter, renal pelvis, biliary tract, brain [glioblastoma], small bowel, sebaceous gland adenomas, and keratoacanthomas) regardless of age
3.Colorectal cancer with high-frequency microsatellite instability pathologic-related features diagnosed <60 years (including presence of tumor infiltrating lymphocytes, Chron's-like lymphocytic reaction, mucinous or signet cell differentiation, or medullary growth pattern)
4.Colorectal cancer diagnosed in at least one first-degree relative with a LS-associated cancer (including colorectum, endometrium, stomach, ovary, pancreas, ureter, renal pelvis, biliary tract, brain [glioblastoma], small bowel, sebaceous gland adenomas, and keratoacanthomas), with one of the cancers being diagnosed <50 years
5.Colorectal cancer diagnosed in at least two first- or second-degree relatives with LS-associated cancer (including colorectum, endometrium, stomach, ovary, pancreas, ureter, renal pelvis, biliary tract, brain [glioblastoma], small bowel, sebaceous gland adenomas, and keratoacanthomas) regardless of age |
|
|
Clinical criteria for LS diagnosis.
|

|
|
Non-urological screening recommendations for Lynch syndrome patients in a multimodal screening approach. EGD, esophagogastroduodenoscopy; CRC, colorectal cancer.
|

|
|
Current urological screening recommendations for Lynch syndrome patients. CT, computed tomography.
|
| [1] |
Lynch HT, Shaw M, Magnuson CW. Hereditary factors in cancer. Study of two large midwestern kindreds. Arch Intern Med 1966; 117:206e12.
|
| [2] |
Giardiello FM, Allen JI, Axilbund JE, Boland CR, Burke CA, Burt RW, et al. Guidelines on genetic evaluation and management of lynch task force on colorectal cancer. Gastroenterology 2014; 147:502e26.
|
| [3] |
Pradere B, Lotan Y, Roupret M. Lynch syndrome in upper tract urothelial carcinoma: significance, screening, and surveillance. Curr Opin Urol 2017; 27:48e55.
|
| [4] |
Mork M, Rouprêt M, Margulis V, Raman J, Lotan Y, O’Brien T, et al. Lynch syndrome: a primer for urologists and panel recommendations. J Urol 2015; 194:21e9.
|
| [5] |
Stjepanovic N, Moreira L, Carneiro F, Balaguer F, Cervantes A, Balma?a J, et al. Hereditary gastrointestinal cancers: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2019; 30:1558e71.
|
| [6] |
Kamiza AB, Wang WC, You JF, Tang R, Chien HT, Lai CH, et al. Cumulative risks of colorectal cancer in Han Chinese patients with Lynch syndrome in Taiwan. Sci Rep 2021; 11:8899. https://doi.org/10.1038/s41598-021-88289-2.
doi: 10.1038/s41598-021-88289-2
pmid: 33903664
|
| [7] |
Goldberg H, Wallis CJD, Klaassen Z, Chandrasekar T, Fleshner N, Zlotta AR. Lynch syndrome in urologic malignanciesdwhat does the urologist need to know. Urology 2019; 134:24e31.
|
| [8] |
Sijmons RH, Kiemeney LALM, Witjes JA, Vasen HFA. Urinary tract cancer and hereditary nonpolyposis colorectal cancer: risks and screening options. J Urol 1998; 160:466e70.
|
| [9] |
Vasen HFA, Wijnen JT, Menko FH, Kleibeuker JH, Taal BG, Griffioen G, et al. Cancer risk in families with hereditary nonpolyposis colorectal cancer diagnosed by mutation analysis. Gastroenterology 1996; 110:1020e7.
|
| [10] |
Watson P, Vasen HFA, Mecklin JP, Bernstein I, Aarnio M, J?rvinen HJ, et al. The risk of extra-colonic, extra-endometrial cancer in the Lynch syndrome. Int J Cancer 2008; 123: 444e9.
|
| [11] |
Engel C, Loeffler M, Steinke V, Rahner N, Holinski-Feder E, Dietmaier W, et al. Risks of less common cancers in proven mutation carriers with Lynch syndrome. J Clin Oncol 2012; 30: 4409e15.
|
| [12] |
Barrow PJ, Ingham S, O’Hara C, Green K, McIntyre I, Lalloo F, et al. The spectrum of urological malignancy in Lynch syndrome. Fam Cancer 2013; 12:57e63.
|
| [13] |
Joost P, Therkildsen C, Dominguez-Valentin M, J?nsson M, Nilbert M. Urinary tract cancer in lynch syndrome; increased risk in carriers of MSH2 mutations. Urology 2015; 86:1212e7.
|
| [14] |
Lonati C, Moschini M, Simeone C. Lynch syndrome in urological practice: diagnosis, therapeutic strategies, and screening for upper tract urothelial carcinoma. Curr Opin Urol 2022; 32: 40e7.
|
| [15] |
Vasen HF, Watson P, Mecklin JP, Lynch TH. New clinical criteria for hereditary nonpolyposis colorectal cancer (HNPCC, Lynch syndrome) proposed by the International Collaborative group on HNPCC. Gastroenterology 1999; 116:1453e6.
|
| [16] |
Umar A, Boland C. Revised Bethesda guidelines for hereditary nonpolyposis colorectal cancer (Lynch syndrome) and microsatellite instability. J Natl Cancer Inst 2004; 96:261e8.
|
| [17] |
Rouprêt M, Catto J, Coulet F, Azzouzi AR, Amira N, Karmouni T, et al. Microsatellite instability as indicator of MSH 2 gene mutation in patients with upper urinary tract transitional cell carcinoma. J Med Genet 2004; 41:e91. https://doi.org/10.1136/jmg.2003.017871.
|
| [18] |
Mork M, Hubosky SG, Rouprêt M, Margulis V, Raman J, Lotan Y, et al. Lynch syndrome: a primer for urologists and panel recommendations. J Urol 2015; 194:21e9.
|
| [19] |
Audenet F, Colin P, Yates DR, Ouzzane A, Pignot G, Long J-A, et al. A proportion of hereditary upper urinary tract urothelial carcinomas are misclassified as sporadic according to a multiinstitutional database analysis: proposal of patient-specific risk identification tool. BJU Int 2012; 110:E583e9. https://doi.org/10.1111/j.1464-410X.2012.11298.x.
|
| [20] |
Rouprêt M, Babjuk M, Burger M, Capoun O, Cohen D, Roupre M, et al. European Association of Urology guidelines on upper urinary tract urothelial carcinoma: 2020 update. Eur Urol 2021; 9:80e1.
|
| [21] |
Boland CR, Thibodeau SN, Hamilton SR, Sidransky D, Burr RW, Meltzer AJ, et al. A National Cancer Institute Workshop on microsatellite instability for cancer detection and familial predisposition: development of international criteria for the determination of microsatellite instability in colorectal cancer. Cancer Res 1998; 59:249e56.
|
| [22] |
Buhard O, Suraweera N, Lectard A, Duval A, Hamelin R. Quasimonomorphic mononucleotide repeats for high-level microsatellite instability analysis. Dis Markers 2004; 20:251e7.
|
| [23] |
Vasen HFA, Blanco I, Aktan-Collan K, Gopie JP, Alonso A, Aretz S, et al. Revised guidelines for the clinical management of Lynch syndrome (HNPCC): recommendations by a group of European experts. Gut 2013; 62:812e823. 6.
|
| [24] |
Rouprêt M, Yates DR, Comperat E, Cussenot O. Upper urinary tract urothelial cell carcinomas and other urological malignancies involved in the hereditary nonpolyposis colorectal cancer (Lynch syndrome) tumor spectrum. Eur Urol 2008; 54: 1226e36.
|
| [25] |
Rouprêt M, Azzouzi A-R, Cussenot O. Microsatellite instability and transitional cell carcinoma of the upper urinary tract. BJU Int 2005; 96:489e92.
|
| [26] |
Snowsill T, Coelho H, Huxley N, Jones-Hughes T, Briscoe S, Frayling IM, et al. Molecular testing for Lynch syndrome in people with colorectal cancer: systematic reviews and economic evaluation. Health Technol Assess 2017; 21:1e238.
|
| [27] |
Hartmann A, Zanardo L, Bocker-Edmonston T, Blaszyk H, Dietmaier W, Stoehr R, et al. Frequent microsatellite instability in sporadic tumors of the upper urinary tract. Cancer Res 2002; 62:6796e802.
|
| [28] |
Urakami S, Inoshita N, Oka S, Miyama Y, Nomura S, Arai M, et al. Clinicopathological characteristics of patients with upper urinary tract urothelial cancer with loss of immunohistochemical expression of the DNA mismatch repair proteins in universal screening. Int J Urol 2018; 25:151e6.
|
| [29] |
Catto JW, Azzouzi AR, Amira N, Rehman I, Feeley KM, Cross SS, et al. Distinct patterns of microsatellite instability are seen in tumours of the urinary tract. Oncogene 2003; 22: 8699e706.
|
| [30] |
Lonati C, Necchi A, Gómez Rivas J, Afferi L, Laukhtina E, Martini A, et al. Upper tract urothelial carcinoma in the Lynch syndrome tumour spectrum: a comprehensive overview from the European Association of Urology-Young Academic Urologists and the Global Society of Rare Genitourinary Tumors. Eur Urol Oncol 2022; 5:30e41.
|
| [31] |
Zachhau P, Walter S. Urinary tract cancer in patients with hereditary non-polyposis colorectal cancer. Scand J Urol Nephrol 2012; 46:5e7.
|
| [32] |
Monahan KJ, Bradshaw N, Dolwani S, Desouza B, Dunlop MG, East JE, et al. Guidelines for the management of hereditary colorectal cancer from the British Society of Gastroenterology (BSG)/Association of Coloproctology of Great Britain and Ireland (ACPGBI)/United Kingdom Cancer Genetics Group (UKCGG). Gut 2020; 69:411e44.
|
| [33] |
van Leerdam ME, Roos VH, van Hooft JE, Balaguer F, Dekker E, Kaminski MF, et al. Endoscopic management of Lynch syndrome and of familial risk of colorectal cancer: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy 2019; 51:1082e93.
|
| [34] |
Crockett DG, Wagner DG, Holmng S, Johansson SL, Lynch HT. Upper urinary tract carcinoma in Lynch syndrome cases. J Urol 2011; 185:1627e30.
|
| [35] |
Aarnio M, S?ily M, Juhola M, Gylling A, Peltom?ki P, J?rvinen HJ, et al. Uroepithelial and kidney carcinoma in Lynch syndrome. Fam Cancer 2012; 11:395e401.
|
| [36] |
Bai ST, Nunez AL, Wei S, Ziober A, Yao Y, Tomaszewski JE, et al. Microsatellite instability and TARBP2 mutation study in upper urinary tract urothelial carcinoma. Am J Clin Pathol 2013; 139:765e70.
|
| [37] |
Skeldon SC, Semotiuk K, Aronson M, Holter S, Gallinger S, Pollett A, et al. Patients with Lynch syndrome mismatch repair gene mutations are at higher risk for not only upper tract urothelial cancer but also bladder cancer. Eur Urol 2013; 63: 379e85.
|
| [38] |
Hubosky SG, Boman BM, Charles S, Bibbo M, Bagley DH. Ureteroscopic management of upper tract urothelial carcinoma (UTUC) in patients with Lynch syndrome (hereditary nonpolyposis colorectal cancer syndrome). BJU Int 2013; 112: 813e9.
|
| [39] |
Therkildsen C, Eriksson P, H?glund M, J?nsson M, Sj?dahl G, Nilbert M, et al. Molecular subtype classification of urothelial carcinoma in Lynch syndrome. Mol Oncol 2018; 12:1286e95.
|
| [40] |
Donahue TF, Clendenning M, Templeton AS, Walsh MF. Genomic characterization of upper-tract urothelial carcinoma in patients with Lynch syndrome abstract. JCO Precis Oncol 2018;2018:PO. 17. https://doi.org/10.1200/PO.17.00143.
|
| [41] |
Metcalfe MJ, Petros FG, Rao P, Mork ME, Xiao LC, Broaddus RR, et al. Universal point of care testing for Lynch syndrome in patients with upper tract urothelial carcinoma. J Urol 2018; 199:60e5.
|
| [42] |
Ito T, Kono K, Eguchi H, Okazaki Y, Yamamoto G, Tachikawa T, et al. Prevalence of Lynch syndrome among patients with upper urinary tract carcinoma in a Japanese hospital-based population. Jpn J Clin Oncol 2019; 50:80e8.
|
| [43] |
Myrh?j T, Andersen MB, Bernstein I. Screening for urinary tract cancer with urine cytology in Lynch syndrome and familial colorectal cancer. Fam Cancer 2008; 7:303e7.
|
| [44] |
Koornstra JJ, Mourits MJ, Sijmons RH, Leliveld AM, Hollema H, Kleibeuker JH. Management of extracolonic tumours in patients with Lynch syndrome. Lancet Oncol 2009; 10:400e8.
|
| [45] |
Acher P, Kiela G, Thomas K, O’Brien T. Towards a rational strategy for the surveillance of patients with Lynch syndrome (hereditary non-polyposis colon cancer) for upper tract transitional cell carcinoma. BJU Int 2010; 106:300e2.
|
| [46] |
Lindor N, Petersen GM, Hadley DW, Kinney AY, Miesfeldt S, Lu KH, et al. Recommendations for the care predisposition to lynch syndrome. JAMA 2014; 296:1507e17.
|
| [47] |
Vasen HFA, Johan G, Offerhaus A, Den Hartog Jager FCA, Menko FH, Nagengast FM, et al. The tumour spectrum in hereditary non-polyposis colorectal cancer: a study of 24 kindreds in The Netherlands. Int J Cancer 1990; 46:31e4.
|
| [48] |
Van der Post RS, Kiemeney LA, Ligtenberg MJL, Witjes JA, Hulsbergen-van de Kaa CA, Bodmer D, et al. Risk of urothelial bladder cancer in Lynch syndrome is increased, in particular among MSH2 mutation carriers. J Med Genet 2010; 47: 464e70.
|
| [49] |
Geary J, Sasieni P, Houlston R, Izatt L, Eeles R, Payne SJ, et al. Gene-related cancer spectrum in families with hereditary non-polyposis colorectal cancer (HNPCC). Fam Cancer 2008; 7: 163e72.
|
| [50] |
Raymond VM, Mukherjee B, Wang F, Huang SC, Stoffel EM, Kastrinos F, et al. Elevated risk of prostate cancer among men with Lynch syndrome. J Clin Oncol 2013; 31:1713e8.
|
| [51] |
Haraldsdottir S, Hampei H, Wei L. Prostate cancer incidence in males with Lynch syndrome. Genet Med 2014; 16:553e7.
|
| [52] |
Win AK, Young JP, Lindor NM, Tucker KM, Ahnen DJ, Young GP, et al. Colorectal and other cancer risks for carriers and noncarriers from families with a DNA mismatch repair gene mutation: a prospective cohort study. J Clin Oncol 2012; 30: 958e64.
|
| [53] |
Aarnio M, Sankila R, Pukkala E. Cancer risk in mutation carriers of DNA-mismatch-repair genes. Int J Cancer 1999; 81: 214e8.
|
| [54] |
Ryan S, Jenkins MA, Win AK. Risk of prostate cancer in Lynch syndrome: a systematic review and meta-analysis. Cancer Epidemiol Biomarkers Prev 2014; 23:437e49.
|
| [55] |
Lim A, Rao P, Matin SF. Lynch syndrome and urologic malignancies: a contemporary review. Curr Opin Urol 2019:357e63.
|
| [56] |
Cárcano FM, Lengert AH, Vidal DO, Scapulatempo Neto C, Queiroz L, Marques H, et al. Absence of microsatellite instability and BRAF (V600E) mutation in testicular germ cell tumors. Andrology 2016; 4: 866e72.
|
| [57] |
Mayer F, Wermann H, Albers P, Stoop H, Gillis AJM, Hartmann JT, et al. Histopathological and molecular features of late relapses in non-seminomas. BJU Int 2011; 107: 936e43.
|
| [58] |
Vasen HFA, Mecklin JP, Meera Khan P, Lynch HT. The International Collaborative Group on Hereditary Non-Polyposis Colorectal Cancer (ICG-HNPCC). Dis Colon Rectum 1991; 34: 424e5.
|
| [1] |
Belinda Nghiem, Xiaotun Zhang, Hung-Ming Lam, Lawrence D. True, Ilsa Coleman, Celestia S. Higano, Peter S. Nelson, Colin C. Pritchard, Colm Morrissey. Mismatch repair enzyme expression in primary and castrate resistant prostate cancer[J]. Asian Journal of Urology, 2016, 3(4): 223-228. |
|
|
|
|