|
|
|
| Extramammary Paget's disease: Updates in the workup and management |
Reza Nabavizadeha,*( ),Khushali B. Vashia,Behnam Nabavizadehb,Vikram M. Narayana,Viraj A.Mastera,c ),Khushali B. Vashia,Behnam Nabavizadehb,Vikram M. Narayana,Viraj A.Mastera,c
|
aDepartment of Urology, Emory University School of Medicine, Atlanta, GA, USA
bDepartment of Urology, Weill Cornell Medicine, New York, NY, USA
cWinship Cancer Institute, Atlanta, GA, USA |
|
|
|
|
Abstract Objective: Extramammary Paget's disease (EMPD) is a rare cutaneous malignant disease. Due to its rarity, there is a paucity of data regarding best treatment strategy. EMPD primarily affects apocrine gland-bearing skin areas such as the vulva, scrotum, and penis. Our objective was to provide a present-day rationale for diagnosis, pathogenesis, and treatment of EMPD with a focus on recent progress in workup and management of the disease. Methods: Literature on EMPD until February 2022 was assessed through PubMed, MEDLINE databases, and Google scholar. A narrative review of the most relevant articles was provided. Results: EMPD usually presents with indolent growth while usually being diagnosed primarily as carcinoma in situ. The foundation of EMPD treatment centers around prompt and accurate diagnosis, wide local or Mohs micrographic surgical excision with proper management towards the margin status, and careful consideration for lymphadenectomy in patients with regionally positive disease. Conventional chemotherapies are alternative treatments modality for patients with distant metastases; however, they sometimes have suboptimal efficacy. At present, there is no agreement regarding adjuvant or systemic therapies, although recent studies have shown several insights into the molecular pathogenesis, tumor biology, and genomics of the development and advancement of EMPD, which may lead to novel and targeted treatment approaches for metastatic EMPD in the future. Conclusion: Patients with EMPD should seek care from physicians with expertise in disease management and patient counseling. These patients should be surveilled with close follow-up to evaluate them for disease recurrence or progression. Global collaborations with groups such as the Global Society for Rare Genitourinary Tumors, and especially patient support groups are crucial in designing clinical trials to help elucidate more robust data in this orphan disease.
|
|
Received: 19 March 2022
Available online: 20 October 2022
|
|
Corresponding Authors:
Reza Nabavizadeh
E-mail: rnabavi@emory.edu
|
|
|

|
|
Initial presentation of an ill-defined eczematous lesion in the apocrine gland-bearing penoscrotal area. The patient signed informed written consent to procedures and publication.
|

| Management | Modality | Summary | | Non-surgical management | Topical treatment: imiquimod | ?
Works [17,18] by innate immune pathway stimulation and inducing inflammatory cytokines such as IL-6, IFN-alpha, and TNF-alpha producing an antitumor effect
?
Advantage: small degree of clinical improvement observed
?
Disadvantage: no complete response | | Photodynamic therapy: photoreactive drugs, such as aminolaevulinic acid | ?
Exposure to appropriate wavelength of light and creating toxic-free radicals which destroy tumor cells
?
Advantage: non-invasive
?
Disadvantages: palliative treatment, pain, and photosensitivity | | Radiation therapy | ?
Radiation doses ranging from 10 Gy to 64 Gy; study [18] showed 97% patients showing CR with 50% achieving improvement
?
Advantage: primary or adjuvant therapy
?
Disadvantages: mucosal and dermatological toxicities, leukopenia, and variable degree of colitis, cystitis, and urethritis | | Laser ablation: Neodym:YAG, CO2, and holmium lasers | ?
Advantages: shorter operative time and less bleeding,
?
Disadvantage: longer healing period | | Surgical management | Surgical excision, punch biopsy, and Mohs micrographic surgery | ?
Advantages: fewer recurrences with wide local excision
?
Disadvantages: tumor border irregularities with unclear margins missing satellite lesions. | | Systemic therapy | Combination drug therapies: FP, FECOM, and PET therapy | ?
Advantage: ideal for metastatic cases
?
Disadvantages: insufficient data due to sample size |
|
|
A summary of different management strategies for EMPD.
|
|
|
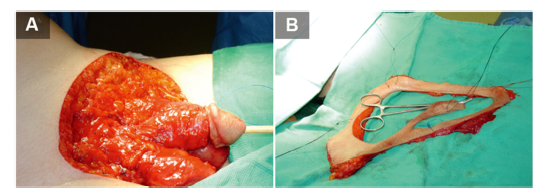
Surgical management of extramammary Paget's disease. (A) Grossly involved skin is resected first; (B) The margin is marked and resected separately for pathologic assessment. The patient signed informed written consent to procedures and publication.
|
|
|
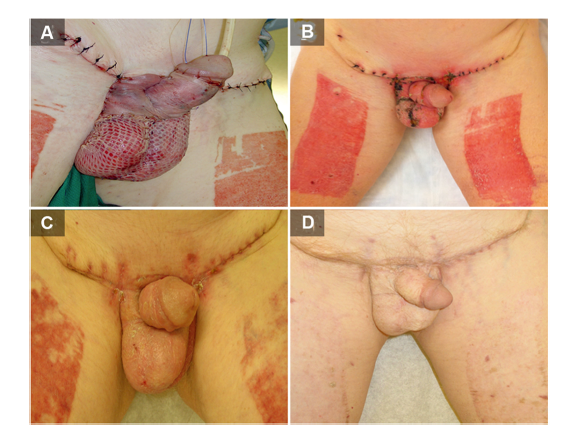
Post-operative wound healing following resection and skin graft for extramammary Paget's disease. (A) Immediate; (B) 1-month; (C) 2-month; (D) 1-year. The patient signed informed written consent to procedures and publication.
|
| Management | Modality | Study | Case, n | Outcome | Best clinical use | | Non-surgical management | Imiquimod | Snast et al., 2020 [18] | 110 | ?
CR in 54% (95% CI 40%-67%)
?
Clinical regression of greater than 50% in 85% of patients (95% CI 74%-90%)
?
40% of patients had recurrence | | | 5-FU | Molina et al., 2019 [19] | 3 (recurrent refractory EMPD cases) product used: 5% 5-FU cream with 0.005% calcipotriene | ?
No patient was found to have a CR; however, they had minimal degree of clinical improvement | | | PDT | Ishizuki and Nakamura, 2021 [5] | NA | ?
Multiple cases have shown antitumor response with PDT
?
PDT can only be used as palliative treatment to reduce symptoms | ?
EMPD lesions of <4 cm | | Radiation doses ranged from 10 Gy to 64 Gy delivered in 1-57 fractions | Snast et al., 2020 [18] | 67 | ?
97% of patients attained CR
?
Patients achieved at least a 50% improvement
?
34% of patients (95% CI 23%-47%) who reached CR had disease recurrence | ?
Primary or adjuvant setting | | Holmium laser | Li et al., 2014 [22] | 61 | ?
Shorter operative time, less bleeding, but with longer wound healing period. | ?
Disease limited to the dermis and epidermis areas | | Carbon dioxide laser | Choi et al., 2001 [23] and Louis-Sylvestre et al., 2004 [24] | 3 | ?
Higher recurrence rates of 67%-100%;
?
Conclusion: use of laser ablation after wide local surgical excision | ?
Primary or adjuvant setting | | Surgical management | Wide excision (1 cm incision margins) | Murata et al., 2005 [26] | 46 | ?
Clinically determined border of well-defined lesions of EMPD corresponded well to the histopathologic border
?
No local recurrence was observed in 24-115 months of follow-up | ?
Well-defined EMPD lesions only | | Mohs micrographic surgery | Long et al., 2017 [30] | 154 | ?
10-fold reduction in the risk of positive margins
?
Recurrence risk was 3.5 (95% CI 1.7-7.2, p<0.001) times more in those with positive pathologic margins compared to those with negative margins | ?
1st line: primary excision or for recurrences from wide local excision | | Punch biopsy | Adashek et al., 2019 [27] | 41 | ?
Cases with carcinoma in situ showed nodular growth patterns and glandular formations | | | Sentinel lymph node biopsy | Fujisawa et al., 2015 [31] | 151 | ?
Multivariate analysis revealed that dermal invasion (odds ratio 5.8, p=0.04) and lympho-vascular invasion (odds ratio 18.0, p=0.0023) were independent factors
?
No difference in survival between patients with or without sentinel lymph node metastasis (p=0.71) | ?
In cases where regional metastasis is present | | Systemic therapy | FECOM therapy | Oashi et al., 2014 [33] | 7 | ?
Partial response found in four patients
?
Median overall survival was 9.4 (range: 7.6-17.3) months
?
Median progression-free survival was 6.5 (range: 2.6-7.9) months
?
1-year survival rate was 43% | ?
Metastatic EMPD | | HER2 | Tanaka et al., 2013 [34] | 104 | ?
HER2 protein was overexpressed in 16 cases (15%) in total | ?
Deep invasion and lymph-node metastasis
?
Aggressive EMPD cases | | Combination chemotherapy of low-dose FP | Tokuda et al., 2015 [36] | 22 | ?
The overall survival ranges were 5-51 (median: 12) months in all 22 patients, 6-51 (median: 13) months in the 13 patients showing CR or PR, and 5-12 (median: 11) months in the 6 SD patients. | ?
Advanced EMPD cases | | Trastuzumab | Fukuda and Funakoshi, 2018 [37] | 3 | ?
Two cases achieved PR
?
One case showed CR | ?
Metastatic EMPD | | Trastuzumab+paclitaxel | Fukuda and Funakoshi, 2018 [37] | 3 | ?
Three cases showed PR | ?
Metastatic EMPD | | Docetaxel+S-1 | Fukuda and Funakoshi, 2018 [37] | 4 | ?
Three cases achieved PR; one case achieved CR. | ?
Metastatic EMPD |
|
|
A summary of studies included in this review article.
|
| [1] |
Crocker HR. Paget’s disease affecting scrotum and penis. Trans Path Soc Lond 1889; 40:187e91.
|
| [2] |
Yao H, Xie M, Fu S, Guo J, Peng Y, Cai Z, et al. Survival analysis of patients with invasive extramammary Paget disease: implications of anatomic sites. BMC Cancer 2018; 18:403. https://doi.org/10.1186/s12885-018-4257-1.
doi: 10.1186/s12885-018-4257-1
pmid: 29636019
|
| [3] |
Yin S, Xu L, Wang S, Feng J, Liu L, Liu G, et al. Prevalence of extramammary Paget’s disease in urban China: a populationbased study. Orphanet J Rare Dis 2021; 16:134. https://doi.org/10.1186/s13023-021-01715-6.
doi: 10.1186/s13023-021-01715-6
|
| [4] |
van der Zwan JM, Siesling S, Blokx WA, Pierie JP, Capocaccia R. Invasive extramammary Paget’s disease and the risk for secondary tumours in Europe. Eur J Surg Oncol 2012; 38:214e21.
|
| [5] |
Ishizuki S, Nakamura Y. Extramammary Paget’s disease: diagnosis, pathogenesis, and treatment with focus on recent developments. Curr Oncol 2021; 28:2969e86.
|
| [6] |
Narayan VM, Master VA. Extramammary Paget’s disease of genitourinary origin. Curr Opin Urol 2022; 32:211e5.
|
| [7] |
Leong JY, Chung PH. A primer on extramammary Paget’s disease for the urologist. Transl Androl Urol 2020; 9:93e105.
|
| [8] |
Ghazawi FM, Iga N, Tanaka R, Fujisawa Y, Yoshino K, Yamashita C, et al. Demographic and clinical characteristics of extramammary Paget’s disease patients in Japan from 2000 to 2019. J Eur Acad Dermatol Venereol 2021; 35:e133e5. https://doi.org/10.1111/jdv.16868.
|
| [9] |
Cheng PS, Lu CL, Cheng CL, Lai FJ. Significant male predisposition in extramammary Paget disease: a nationwide populationbased study in Taiwan. Br J Dermatol 2014; 171:191e3.
|
| [10] |
Wilkinson EJ, Brown HM. Vulvar Paget disease of urothelial origin:a report of three cases and a proposed classification of vulvar Paget disease. Hum Pathol 2002; 33:549e54.
|
| [11] |
Hegarty PK, Suh J, Fisher MB, Taylor J, Nguyen TH, Ivan D, et al. Penoscrotal extramammary Paget’s disease: the University of Texas M. D. Anderson Cancer Center contemporary experience. J Urol 2011; 186:97e102.
|
| [12] |
Stasenko M, Jayakumaran G, Cowan R, Broach V, Chi DS, Rossi A, et al. Genomic alterations as potential therapeutic targets in extramammary Paget’s disease of the vulva. JCO Precis Oncol 2020; 4:1054e60.
|
| [13] |
Kang Z, Xu F, Zhang QA, Wu Z, Zhang X, Xu J, et al. Oncogenic mutations in extramammary Paget’s disease and their clinical relevance. Int J Cancer 2013; 132:824e31.
|
| [14] |
Phyo AK, Mun KS, Kwan KC, Ann CC, Kuppusamy S. Genitourinary extramammary Paget’s disease: review and outcome in a multidisciplinary setting. Int J Clin Exp Pathol 2020; 13:2369e76.
|
| [15] |
Ohnishi T, Watanabe S. The use of cytokeratins 7 and 20 in the diagnosis of primary and secondary extramammary Paget’s disease. Br J Dermatol 2000; 142:243e7.
|
| [16] |
Shu B, Shen XX, Chen P, Fang XZ, Guo YL, Kong YY. Primary invasive extramammary Paget disease on penoscrotum: a clinicopathological analysis of 41 cases. Hum Pathol 2016; 47:70e7.
|
| [17] |
Bubna AK. Imiquimoddits role in the treatment of cutaneous malignancies. Indian J Pharmacol 2015; 47:354e9.
|
| [18] |
Snast I, Sharon E, Kaftory R, Noyman Y, Oren-Shabtai M, Lapidoth M, et al. Nonsurgical treatments for extramammary Paget disease: a systematic review and meta-analysis. Dermatology 2020; 236:493e9.
|
| [19] |
Molina GE, Khalifian S, Mull JL, Chen L, Rosman IS, Faulkner- Jones BE, et al. Topical combination of fluorouracil and calcipotriene as a palliative therapy for refractory extramammary Paget disease. JAMA Dermatol 2019; 155:599e603.
|
| [20] |
Wang D, Wang P, Li C, Zhou Z, Zhang L, Zhang G, et al. Efficacy and safety of HpD-PDT for extramammary Paget’s disease refractory to conventional therapy: a prospective, open-label and single arm pilot study. Photodiagnosis Photodyn Ther 2022; 37:102670. https://doi.org/10.1016/j.pdpdt.2021.102670.
|
| [21] |
Hata M, Koike I, Wada H, Miyagi E, Kasuya T, Kaizu H, et al. Radiation therapy for extramammary Paget’s disease: treatment outcomes and prognostic factors. Ann Oncol 2014; 25:291e7.
|
| [22] |
Li Z, Yang D, Che X, Zong H, Adnan H, Wang J, et al. Clinical research of holmium laser therapy in extramammary Paget’s disease. Laser Med Sci 2014; 29:1907e12.
|
| [23] |
Choi JB, Yoon ES, Yoon DK, Kim DS, Kim JJ, Cho JH. Failure of carbon dioxide laser treatment in three patients with penoscrotal extramammary Paget’s disease. BJU Int 2001; 88:297e8.
|
| [24] |
Louis-Sylvestre C, Haddad B, Paniel BJ. Paget’s disease of the vulva: results of different conservative treatments. Eur J Obstet Gynecol Reprod Biol 2001; 99:253e5.
|
| [25] |
Christodoulidou M, Alnajjar HM, Parnham A, Khetrapal P, Freeman A, Haider A, et al. Multidisciplinary approach for the management of penoscrotal extramammary Paget’s diseasedan eUROGEN study. Urol Oncol 2021; 39:501.e1_10. https://doi.org/10.1016/j.urolonc.2021.05.018.
|
| [26] |
Murata Y, Kumano K. Extramammary Paget’s disease of the genitalia with clinically clear margins can be adequately resected with 1 cm margin. Eur J Dermatol 2005; 15:168e70.
|
| [27] |
Adashek JJ, Leonard A, Nealon SW, Krishnan A, Mosiello GC, Dhillon J, et al. Extramammary Paget’s disease: what do we know and how do we treat. Can J Urol 2019; 26:10012e21.
|
| [28] |
Kaku-Ito Y, Ito T, Tsuji G, Nakahara T, Hagihara A, Furue M, et al. Evaluation of mapping biopsies for extramammary Paget disease: a retrospective study. J Am Acad Dermatol 2018; 78: 1171e1177.e4. https://doi.org/10.1016/j.jaad.2017.12.040.
|
| [29] |
Wollina U, Goldman A, Bieneck A, Abdel-Naser MB, Petersen S. Surgical treatment for extramammary Paget’s disease. Curr Treat Options Oncol 2018; 19:27. https://doi.org/10.1007/s11864-018-0545-x.
doi: 10.1007/s11864-018-0545-x
|
| [30] |
Long B, Schmitt AR, Weaver AL, McGree M, Bakkum-Gamez JN, Brewer J, et al. A matter of margins: surgical and pathologic risk factors for recurrence in extramammary Paget’s disease. Gynecol Oncol 2017; 147:358e63.
|
| [31] |
Fujisawa Y, Yoshino K, Kiyohara Y, Kadono T, Murata Y, Uhara H, et al. The role of sentinel lymph node biopsy in the management of invasive extramammary Paget’s disease: multi-center, retrospective study of 151 patients. J Dermatol Sci 2015; 79:38e42.
|
| [32] |
Guercio BJ, Iyer G, Kidwai WZ, Lacouture ME, Ghafoor S, Rossi AM, et al. Treatment of metastatic extramammary Paget disease with combination ipilimumab and nivolumab: a case report. Case Rep Oncol 2021; 14:430e8.
|
| [33] |
Oashi K, Tsutsumida A, Namikawa K, Tanaka R, Omata W, Yamamoto Y, et al. Combination chemotherapy for metastatic extramammary Paget disease. Br J Dermatol 2014; 170: 1354e7.
|
| [34] |
Tanaka R, Sasajima Y, Tsuda H, Namikawa K, Tsutsumida A, Otsuka F, et al. Human epidermal growth factor receptor 2 protein overexpression and gene amplification in extramammary Paget disease. Br J Dermatol 2013; 168:1259e66.
|
| [35] |
Tanese K, Nakamura Y, Hirai I, Funakoshi T. Updates on the systemic treatment of advanced non-melanoma skin cancer. Front Med 2019; 6:160. https://doi.org/10.3389/fmed.2019.00160.
doi: 10.3389/fmed.2019.00160
|
| [36] |
Tokuda Y, Arakura F, Uhara H. Combination chemotherapy of low-dose 5-fluorouracil and cisplatin for advanced extramammary Paget’s disease. Int J Clin Oncol 2015; 20:194e7.
|
| [37] |
Fukuda K, Funakoshi T. Metastatic extramammary Paget’s disease: pathogenesis and novel therapeutic approach. Front Oncol 2018; 8:38. https://doi.org/10.3389/fonc.2018.00038.
doi: 10.3389/fonc.2018.00038
|
| [38] |
Liegl B, Horn LC, Moinfar F. Androgen receptors are frequently expressed in mammary and extramammary Paget’s disease. Mod Pathol 2005; 18:1283e8.
|
| [39] |
Yoneyama K, Kamada N, Kinoshita K, Kawashima T, Otani M, Endo H, et al. Androgen-deprivation regimen for multiple bone metastases of extramammary Paget disease. Br J Dermatol 2005; 153:853e5.
|
| [40] |
Karpathiou G, Chauleur C, Hathroubi S, Habougit C, Peoc’h M. Expression of CD3, PD-L1 and CTLA-4 in mammary and extramammary Paget disease. Cancer Immunol Immunother 2018; 67:1297e303.
|
| [41] |
Goto H, Sugita K, Yamamoto O. Expression of programmed death-ligand 1 and programmed death-1 in patients with extramammary Paget’s disease. Indian J Dermatol 2021; 66: 169e73.
|
| [42] |
Fujimura T, Kambayashi Y, Kakizaki A, Furudate S, Aiba S. RANKL expression is a useful marker for differentiation of pagetoid squamous cell carcinoma in situ from extramammary Paget disease. J Cutan Pathol 2016; 43:772e5.
|
| No related articles found! |
|
|
|
|