Objective: To evaluate the predictive validity of IRIS™ (Intuitive Surgical®, Sunnyvale, CA, USA) as a planning tool for robot-assisted partial nephrectomy (RAPN) by assessing the degree of overlap with intraoperative execution.
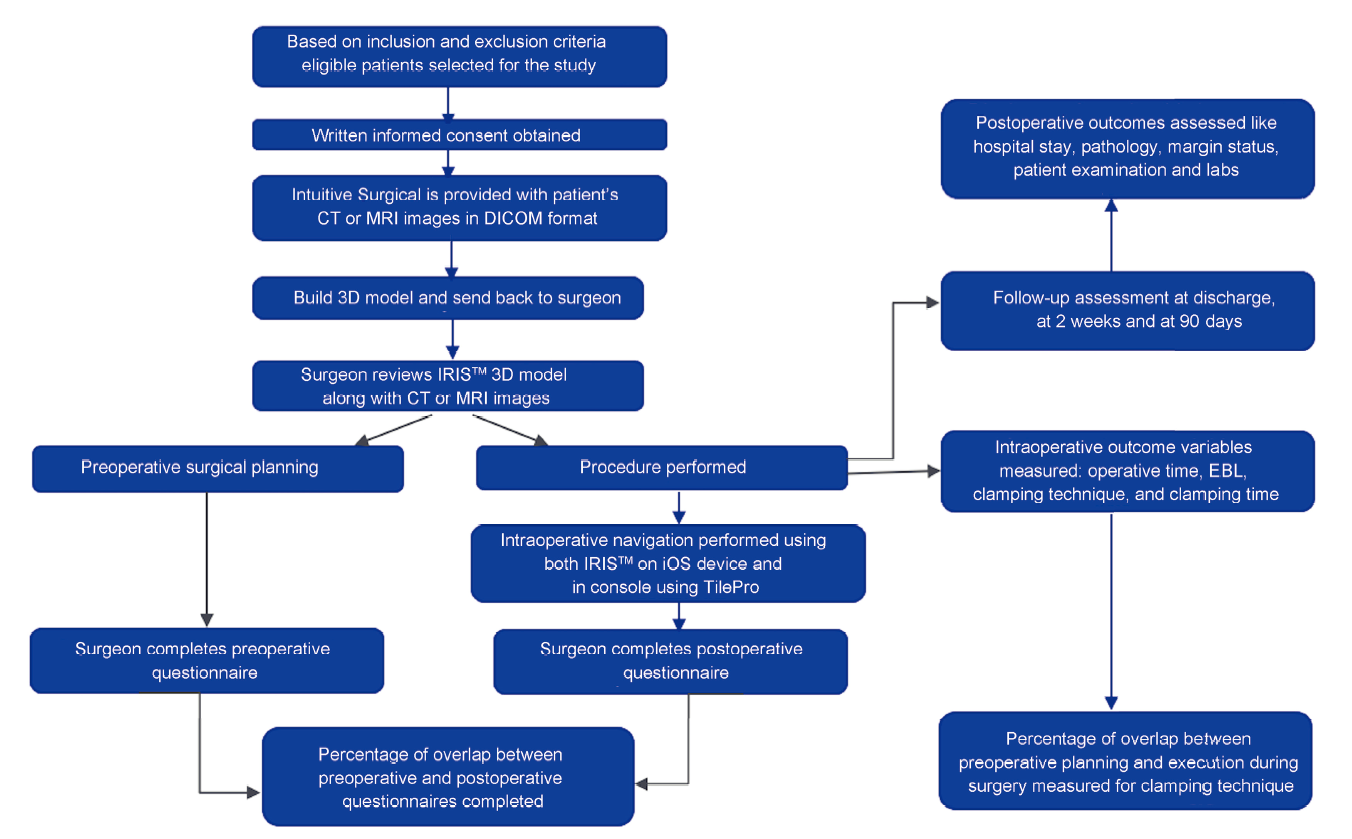
Methods: Thirty-one patients scheduled for RAPN by four experienced urologists were enrolled in a prospective study. Prior to surgery, urologists reviewed the IRIS™ three-dimensional model on an iphone Operating System (iOS) app and completed a questionnaire outlining their surgical plan including surgical approach, and ischemia technique as well as confidence in executing this plan. Postoperatively, questionnaires assessing the procedural approach, clinical utility, efficiency, and effectiveness of IRIS™ were completed. The degree of overlap between the preoperative and intraoperative questionnaires and between the planned approach and actual execution of the procedure was analyzed. Questionnaires were answered on a 5-point Likert scale and scores of 4 or greater were considered positive.
Results: Mean age was 65.1 years with a mean tumor size of 27.7 mm (interquartile range 17.5-44.0 mm). Hilar tumors consisted of 32.3%; 48.4% of patients had R.E.N.A.L. nephrometry scores of 7-9. On preoperative questionnaires, the surgeons reported that in 67.7% cases they were confident that they can perform the procedure successfully, and on intraoperative questionnaires, the surgeons reported that in 96.8% cases IRIS™ helped achieve good spatial sensation of the anatomy. There was a high degree of overlap between preoperative and intraoperative questionnaires for the surgical approach, interpreting anatomical details and clinical utility. When comparing plans for selective or off-clamp, the preoperative plan was executed in 90.0% of cases intraoperatively.
Conclusion: A high degree of overlap between the preoperative surgical approach and intraoperative RAPN execution was found using IRIS™. This is the first study to evaluate the predictive accuracy of IRIS™ during RAPN by comparing preoperative plan and intraoperative execution.
. [J]. Asian Journal of Urology, 2023, 10(4): 431-439.
Ahmed Ghazi, Nitin Sharma, Ahmed Radwan, Hani Rashid, Thomas Osinski, Thomas Frye, William Tabayoyong, Jonathan Bloom, Jean Joseph. Can preoperative planning using IRIS™ three-dimensional anatomical virtual models predict operative findings during robot-assisted partial nephrectomy?. Asian Journal of Urology, 2023, 10(4): 431-439.
6. Metastatic disease with life expectancy less than 1 year
7. Pregnant or suspected pregnancy
8. Mentally handicapped, underlying psychological disorder or severe systemic illness precluding compliance with study requirements
9. Patient belonging to other vulnerable population, e.g., prisoner or ward of the state
Patient demographic
All patients for IRIS? (n=31)
R.E.N.A.L. nephrometry score
4-6 (n=8)
7-9 (n=15)
10-12 (n=8)
Age, year
Mean±SD
65.1±14.9
55.5±21.4
70.1±7.4
65.4±14.9
Median (IQR)
67.0 (57.0-74.0)
57.0 (40.0-69.0)
71.0 (63.0-74.0)
66.5 (51.5-79.0)
Gender (male:female)
20:11
6:2
9:6
5:3
BMIa, kg/m2
30.6±6.5
27.7±3.3
32.1±7.7
30.9±6.0
ASA classification, n (%)
Class 1
2 (6.5)
2 (25.0)
0 (0)
0 (0)
Class 2
12 (38.7)
2 (25.0)
7 (46.7)
3 (37.5)
Class 3
17 (54.8)
4 (50.0)
8 (53.3)
5 (62.5)
Class 4
0 (0)
0 (0)
0 (0)
0 (0)
Major abdominal surgery, n
5
1
4
0
Laterality (left:right)
11:20
4:4
6:9
1:7
Tumor location (anterior:hilar:posterior:other)
11:10:9:1
5:0:3:0
5:4:5:1
1:6:1:0
Tumor sizea, mm
27.7±17.3
26.5±18.9
25.3±12.4
33.1±23.5
Estimated hilar dissection timea, min
12.5±8.5
12.5±8.5
11.7±9.0
25.0±20.6
Estimated tumor resection timea, min
8.6±4.5
6.9±2.8
7.6±4.4
12.3±4.2
Estimated renorrhaphy timea, min
12.8±7.3
10.3±3.9
14.7±13.7
16.5±8.5
LOSa, day
1.7±1.1
1.1±0.4
1.7±1.1
2.3±1.3
Preoperative questionnaires to surgeons' evaluating imaging using both IRIS? and CT scan
R.E.N.A.L. nephrometry score
All patients for IRIS? (n=31)
4-6 (n=8)
7-9 (n=15)
10-12 (n=8)
Which part of the renal anatomy was IRIS? with CT scan helpful to achieve good spatial sensation
Tumor location
7 (87.5)
15 (100.0)
8 (100.0)
30 (96.8)
Renal artery identification
7 (87.5)
15 (100.0)
8 (100.0)
30 (96.8)
Renal vein identification
8 (100.0)
15 (100.0)
8 (100.0)
31 (100.0)
Tumor depth identification
7 (87.5)
15 (100.0)
8 (100.0)
30 (96.8)
Relationship of tumor to surrounding structures
6 (75.0)
15 (100.0)
8 (100.0)
29 (93.5)
Which part of the operation were you satisfied with the information available using IRIS? and CT scan
Identification of ureter and vessels
4 (50.0)
11 (73.3)
3 (37.5)
18 (58.1)
Identification of tumor location
6 (75.0)
15 (100.0)
8 (100.0)
29 (93.5)
Identification of tumor depth
6 (75.0)
14 (93.3)
8 (100.0)
28 (90.3)
Tumor resection for a complex tumor
2 (25.0)
8 (53.3)
7 (87.5)
17 (54.8)
Aided in planning of off-clamp or segmental clamping
3 (37.5)
7 (46.7)
4 (50.0)
14 (45.2)
Identification of feeding vessel to the tumor
2 (25.0)
11 (73.3)
7 (87.5)
20 (64.5)
Not useful in this procedure
1 (12.5)
0 (0)
0 (0)
1 (3.2)
You are confident that you will successfully complete the planned procedure
8 (100.0)
9 (60.0)
4 (50.0)
21 (67.7)
How long did it take to visualize, assess, and interpret the IRIS? 3D model with CT scan for the purpose of surgical planning
<1 min
4 (50.0)
4 (26.7)
1 (12.5)
9 (29.0)
2-5 min
3 (37.5)
9 (60.0)
7 (87.5)
19 (61.3)
>5 min
1 (12.5)
2 (13.3)
0 (0)
3 (9.7)
Which artery branch will you select for clamping based on IRIS? 3D model with CT scan
Primary renal artery
5 (62.5)
4 (26.7)
2 (25.0)
11 (35.5)
Secondary branch
1 (12.5)
4 (26.7)
5 (62.5)
10 (32.3)
Tertiary branch
0 (0)
3 (20.0)
1 (25.0)
4 (12.9)
Not applicable
2 (25.0)
4 (26.7)
0 (0)
6 (19.4)
You feel the extra time spent on IRIS? technology was valuable
Yes
7 (87.5)
15 (100.0)
8 (100.0)
30 (96.8)
Aspect of surgery
Questionnaire result
Overlap, %
Preoperative
Intraoperative
Interpretation of anatomy, n (%)
31 (100.0)
31 (100.0)
100.0
Tumor location
30 (96.8)
31 (100)
96.8
Renal artery
30 (96.8)
31 (100)
96.8
Renal vein
31 (100)
31 (100)
100.0
Tumor depth
30 (96.8)
31 (100)
96.8
Relationship to surrounding structures
29 (93.5)
30 (96.8)
96.7
The part of the operation or clinical situation where you were satisfied with the information available in the IRIS? 3D model with CT scan, n (%)
Identification of ureter and vessels
22 (71.0)
21 (67.7)
95.5
Identification of tumor location
29 (93.5)
30 (96.8)
96.7
Identification of tumor depth
28 (90.3)
30 (96.8)
93.3
Tumor resection for complex tumor
17 (54.8)
17 (54.8)
100.0
Aided in planning of off-clamping or segmental clamping
14 (45.2)
14 (45.2)
100.0
Identification of feeding vessel to the tumor
20 (64.5)
19 (61.3)
95.0
Clamping techniquea, n
Primary renal artery clamping
11
13
84.6
Off-clamp and selective clamping
20
18
90.0
No clamp
6
8
75.0
Secondary artery clamping
10
7
70.0
Tertiary artery clamping
4
3
75.0
Intraoperative questionnaires given to surgeons evaluating imaging using both IRIS? and CT scan
R.E.N.A.L. nephrometry score
All patients for IRIS? (n=31)
4-6 (n=8)
7-9 (n=15)
10-12 (n=8)
The IRIS? 3D model with CT scan visualization method made your procedure efficient
Agree and strongly agree
5 (62.5)
14 (93.3)
8 (100.0)
27 (87.1)
The IRIS? 3D model with CT scan visualization method allowed the identification of target anatomy for this procedure
Agree and strongly agree
7 (87.5)
15 (100.0)
8 (100.0)
30 (96.8)
Does use of IRIS? model lead to any alteration in intraoperative plan compared to preoperative plan
No
8 (100.0)
15 (100.0)
8 (100.0)
31 (100.0)
How easy is IRIS? technology to use intraoperatively
Very easy
4 (50.0)
11 (73.3)
7 (87.5)
22 (71.0)
Easy
4 (50.0)
4 (26.7)
1 (12.5)
9 (29.0)
Neutral, difficult, very difficult
0 (0.0)
0 (0.0)
0 (0)
0 (0.0)
How many times did you refer to the IRIS? model with CT scan during the procedure
1-2 times
6 (75.0)
4 (26.7)
1 (12.5)
11 (35.5)
3 times
2 (25.0)
8 (53.3)
3 (37.5)
13 (41.9)
4-10 times
0 (0)
3 (20.0)
2 (25.0)
5 (16.1)
>10 times
0 (0)
0 (0)
2 (25.0)
2 (6.5)
Did you use the IRIS? model on iOS device or TilePro
iOS device only
7 (87.5)
10 (66.7)
1 (12.5)
18 (58.1)
TilePro only
0 (0)
0 (0)
1 (12.5)
1 (3.2)
Both iOS and TilePro
1 (12.5)
5 (33.3)
6 (75.0)
12 (38.7)
Do you think that using IRIS? model during surgery caused disruption to the procedure
Yes
0 (0)
0 (0)
0 (0)
0 (0)
Which feature of IRIS? software was most valuable
Pan and rotate
5 (62.5)
14 (93.3)
8 (100.0)
27 (87.1)
Alternating component transparency
4 (50.0)
11 (73.3)
7 (87.5)
22 (71.0)
Slice display
2 (25.0)
1 (6.7)
0 (0)
3 (9.7)
Windowing
3 (37.5)
1 (6.7)
1 (12.5)
5 (16.1)
Do you think that interaction of the IRIS? software with CT scan was very intuitive
Agree and strongly agree
7 (87.5)
15 (100.0)
8 (100.0)
30 (96.8)
The IRIS? 3D model with CT scans could simplify the clinical case discussion with the patient
Agree and strongly agree
6 (75.0)
15 (100.0)
8 (100.0)
29 (93.5)
Was IRIS? a useful tool for discussion of the case with your trainees intraoperatively
Agree and strongly agree
7 (87.5)
15 (100.0)
8 (100.0)
30 (96.8)
The visual quality of the IRIS? is sufficient to support you preoperatively and intraoperatively
Agree and strongly agree
8 (100.0)
14 (93.3)
8 (100.0)
30 (96.8)
[1]
Tan HJ, Filson CP, Litwin MS. Contemporary, age-based trends in the incidence and management of patients with early-stage kidney cancer. Urol Oncol 2015; 33:21.e19-26. https://doi.org/10.1016/j.urolonc.2014.10.002.
doi: 10.1016/j.urolonc.2014.10.002
[2]
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin 2000; 70:7-30.
doi: 10.3322/caac.v70.1
[3]
Venkatramani V, Koru-Sengul T, Miao F, Nahar B, Prakash NS, Swain S, et al. A comparison of overall survival and perioperative outcomes between partial and radical nephrectomy for cT1b and cT 2 renal cell carcinomadanalysis of a national cancer registry. Urol Oncol 2018; 36:90.e9-14. https://doi.org/10.1016/j.urolonc.2017.11.008.
doi: 10.1016/j.urolonc.2017.11.008
pmid: 29254672
[4]
Mir MC, Derweesh I, Porpiglia F, Zargar H, Mottrie A, Autorino R. Partial nephrectomy versus radical nephrectomy for clinical T1b and T2 renal tumors: a systematic review and meta-analysis of comparative studies. Eur Urol 2017; 71:606-17.
doi: S0302-2838(16)30533-4
pmid: 27614693
[5]
Rogers C, Sukumar S, Gill IS. Robotic partial nephrectomy: the real benefit. Curr Opin Urol 2011; 21:60-4.
doi: 10.1097/MOU.0b013e3283402232
pmid: 20962648
[6]
Kutikov A, Uzzo RG, The RENAL. Nephrometry score: a comprehensive standardized system for quantitating renal tumor size, location, and depth. J Urol 2009; 182:844-53.
doi: 10.1016/j.juro.2009.05.035
[7]
Ficarra V, Novara G, Secco S, Macchi V, Porzionato A, De Caro R, et al. Preoperative aspects, and dimensions used for an anatomical (PADUA) classification of renal tumors in patients who are candidates for nephron-sparing surgery. Eur Urol 2009; 56:786-93.
doi: 10.1016/j.eururo.2009.07.040
Lasser MS, Doscher M, Keehn A, Chernyak V, Garfein E, Ghavamian R. Virtual surgical planning: a novel aid to robotassisted laparoscopic partial nephrectomy. J Endourol 2012; 26:1372-9.
doi: 10.1089/end.2012.0093
[10]
Shirk JD, Kwan L, Saigal C. The use of 3-dimensional, virtual reality models for surgical planning of robotic partial nephrectomy. Urology 2019; 125:92-7.
doi: S0090-4295(18)31351-7
pmid: 30597166
[11]
Shirk JD, Thiel DD, Wallen EM, Linehan JM, White WM, Badani KK, et al. Effect of 3-dimensional virtual reality models for surgical planning of robotic-assisted partial nephrectomy on surgical outcomes: a randomized clinical trial. JAMA Netw Open 2019; 4:2-11.
[12]
Wake N, Nussbaum JE, Elias MI, Nikas CV, Bjurlin MA. 3D printing, augmented reality, and virtual reality for the assessment and management of kidney and prostate cancer: a systematic review. Urology 2020; 143:20-32.
doi: S0090-4295(20)30663-4
pmid: 32535076
[13]
Gurung PMS, Melnyk R, Holler T, Oppenhimer D, Witthaus M, Hani HH, et al. Application of IRIS three-dimensional anatomical models as preoperative surgical planning tools in the management of localized renal masses. J Endourol 2021; 35: 383-9.
doi: 10.1089/end.2020.0405
pmid: 33451273
[14]
Giavarina D. Understanding Bland Altman analysis. Biochem Med (Zagreb) 2015; 25:141-51.
doi: 10.11613/issn.1846-7482
[15]
Porpiglia F, Fiori C, Checcucci E, Amparore D, Bertolo R. Hyperaccuracy three-dimensional reconstruction is able to maximize the efficacy of selective clamping during robotassisted partial nephrectomy for complex renal masses. Eur Urol 2018; 74:651-60.
doi: 10.1016/j.eururo.2017.12.027
[16]
Checcucci F, Amparore D, Fiori C, Manfredi M, Ivano M, Di Dio M, et al. 3D imaging applications for robotic urologic surgery: an ESUT YAUWP review. World J Urol 2020; 38:869-81.
doi: 10.1007/s00345-019-02922-4
pmid: 31456017
[17]
Hung AJ, Shah SH, Dalag L, Shin D, Gill IS. Development and validation of a novel robotic procedure specific simulation platform: partial nephrectomy. J Urol 2015; 194:520-6.
doi: 10.1016/j.juro.2015.02.2949
pmid: 25801765
[18]
Kobayashi S, Cho B, Huaulmé A, Tatsugami K, Honda H, Jannin P, et al. Assessment of surgical skills by using surgical navigation in robot-assisted partial nephrectomy. Int J Comput Assist Radiol Surg 2019; 14:1449-59.
doi: 10.1007/s11548-019-01980-8
pmid: 31119486
[19]
Kobayashi S, Cho B, Mutaguchi J, Inokuchi J, Tatsugami K, Hashizume M, et al. Surgical navigation improves renal parenchyma volume preservation in robot-assisted partial nephrectomy: a propensity score matched comparative analysis. J Urol 2020; 204:149-56.
doi: 10.1097/JU.0000000000000709
pmid: 31859597
[20]
Ukimura O, Nakamoto M, Gill IS. Three-dimensional reconstruction of renovascular-tumor anatomy to facilitate zeroischemia partial nephrectomy. Eur Urol 2012; 61:211-7.
doi: 10.1016/j.eururo.2011.07.068
pmid: 21937162
[21]
Porpiglia F, Amparore D, Checcucci E, Maanfredi M, Stura I, Migliaretti G, et al. Three-dimensional virtual imaging of renal tumours: a new tool to improve the accuracy of nephrometry scores. BJU Int 2019; 124:945-54.
doi: 10.1111/bju.14894
pmid: 31390140
[22]
Hyde ER, Berger LU, Ramachandran N, Hughes-Hallett A, Pavithran NP, Tran MGB, et al. Interactive virtual 3D models of renal cancer patient anatomies alter partial nephrectomy surgical planning decisions and increase surgeon confidence compared to volume-rendered images. Int J Comput Assist Radiol Surg 2019; 14:723-32.
doi: 10.1007/s11548-019-01913-5
pmid: 30680601
[23]
Antonelli A, Veccia A, Palumbo C, Peroni A, Mirabella G, Cozzoli A, et al. Holographic reconstructions for preoperative planning before partial nephrectomy: a head-to-head comparison with standard CT scan. Urol Int 2019; 102:212-7.
doi: 10.1159/000495618
pmid: 30540991
[24]
Checcucci E, Amparore D, Pecoraro A, Peretti D, Aimar R, De Cillis S, et al. Mixed reality holograms for preoperative surgical planning of nephron-sparing surgery: evaluation of surgeons’ perception. Minerva Urol Nephrol 2021; 73:367-75.
doi: 10.23736/S2724-6051.19.03610-5
pmid: 31486325