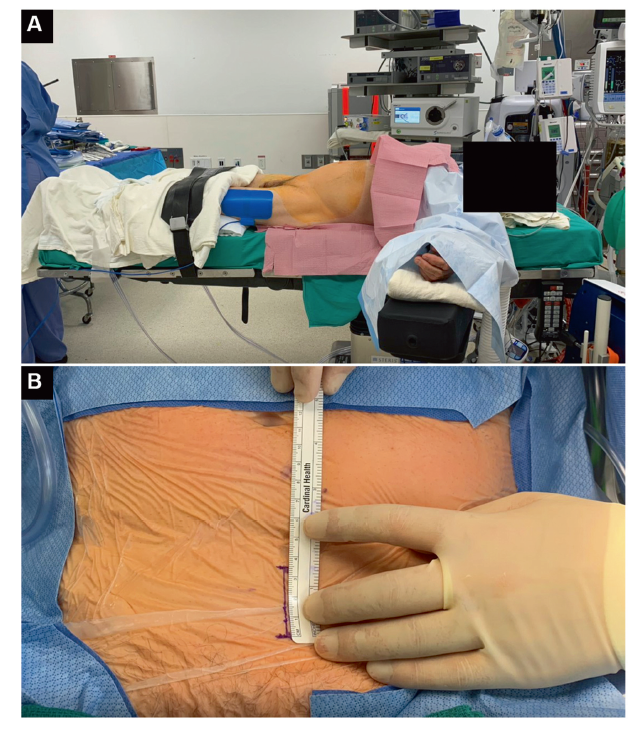
Objective: To describe the surgical technique and report the early outcomes of the transvesical (TV) approach to single-port (SP) robot-assisted radical prostatectomy.
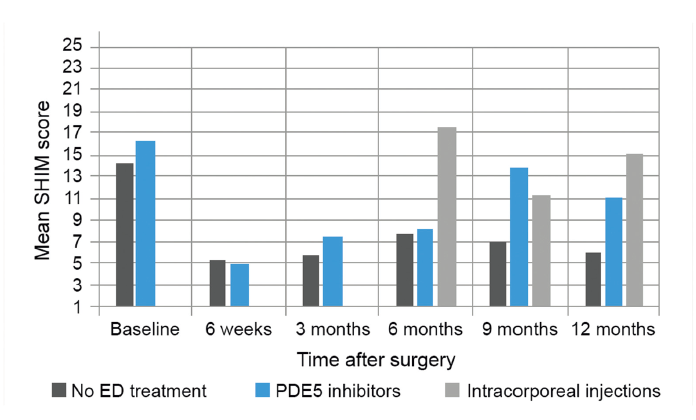
Methods: All procedures were performed at a single center by one surgeon. We identified the first 100 consecutive patients with clinically localized prostate cancer that underwent SP TV robot-assisted radical prostatectomy using the da Vinci SP robotic surgical system. Data were collected prospectively and analyzed with descriptive statistics. The primary outcomes assessed were postoperative urinary continence, rate of biochemical recurrence, and sexual function.
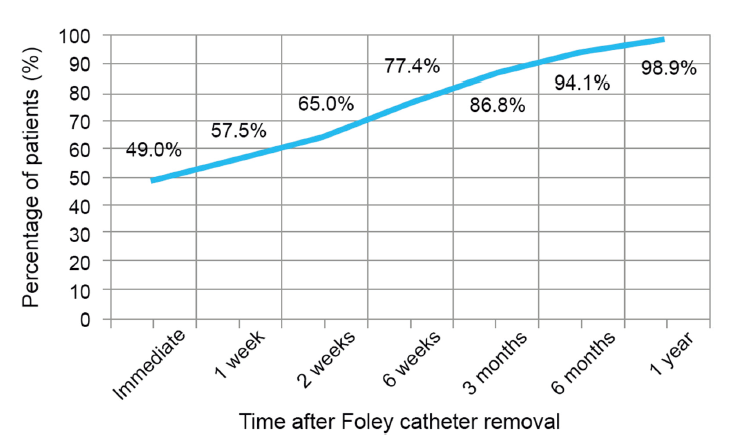
Results: All procedures were performed without extra ports or conversion. The median age was 62.1 years and 49.0% of the patients had abdominal surgery history. The preoperative median prostate-specific antigen value and prostate volume were 5.0 ng/mL and 33.0 mL, respectively. There were no intraoperative complications. The median operative time and estimated blood loss were 212.5 min and 100.0 mL, respectively. A total of 92.0% of patients were discharged within 24.0 h, with an overall median length of stay of 5.6 h. Only 4.0% of patients required opioid prescriptions at discharge. The median Foley catheter duration was 3 days. Positive margins were present in 15.0% of cases. Median follow-up was 10.4 months. Continence rate was immediate after Foley removal in 49.0% of cases, 65.0% at 2 weeks, 77.4% at 6 weeks, 94.1% at 6 months, and 98.9% at 1 year. One case of biochemical recurrence (1.0%) was noted 3 months after surgery.
Conclusion: The SP TV approach for radical prostatectomy cases is a safe and feasible technique for patients with clinically localized prostate cancer. This technique offers advantages of short hospital stay, minimal narcotic use postoperatively, and promising early return of urinary continence, without compromising oncologic outcomes.
. [J]. Asian Journal of Urology, 2023, 10(4): 416-422.
Roxana Ramos-Carpinteyro, Ethan L. Ferguson, Jaya S. Chavali, Albert Geskin, Jihad Kaouk. First 100 cases of transvesical single-port robotic radical prostatectomy. Asian Journal of Urology, 2023, 10(4): 416-422.
Hamdy FC, Donovan JL, Lane JA, Mason M, Metcalfe C, Holding P, et al. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med 2016; 375:1415. https://doi.org/10.1056/NEJMoa1606220.
doi: 10.1056/NEJMoa1606220
[2]
Eastham JA, Auffenberg GB, Barocas DA, Chou R, Crispino T, Davis JW, et al. AUA/ASTRO guideline on clinically localized prostate cancerdpart I: introduction, risk assessment, staging, and risk-based management. J Urol 2022. https://doi.org/10.1097/JU.0000000000002757.
[3]
Schaeffer EM, Srinivas S, An Y, Armstrong AJ, Barocas D, Chapin B, et al. Version 4.2022 of the NCCN guidelines for prostate cancer. NCCN 2022. https://www.nccn.org/guidelines/guidelinesdetail?categoryZ1&idZ1459. [Accessed 25 August 2022].
[4]
Bekelman JE, Rumble RB, Chen RC, Pisansky TM, Finelli A, Feifer A, et al. Clinically localized prostate cancer: ASCO clinical practice guideline endorsement of an American Urological Association/American Society for Radiation Oncology/ Society of Urologic Oncology guideline. J Clin Oncol 2018; 36:3251. https://doi.org/10.1200/JCO.18.00606.
doi: 10.1200/JCO.18.00606
pmid: 30183466
[5]
Sooriakumaran P, Srivastava A, Shariat SF, Stricker PD, Ahlering T, Eden CG, et al. A multinational, multi-institutional study comparing positive surgical margin rates among 22 393 open, laparoscopic, and robot-assisted radical prostatectomy patients. Eur Urol 2014; 66:450-6.
doi: 10.1016/j.eururo.2013.11.018
pmid: 24290695
[6]
Kaouk J, Garisto J, Sagalovich D, Dagenais J, Bertolo R, Klein E. Robotic single-port partial prostatectomy for anterior tumors: transvesical approach. Urology 2018; 118:242. https://doi.org/10.1016/j.urology.2018.03.034.
doi: S0090-4295(18)30291-7
pmid: 29704582
[7]
Kaouk J, Sawczyn G, Wilson C, Aminsharifi A, Fareed K, Garisto J, et al. Single-port percutaneous transvesical simple prostatectomy using the SP robotic system: initial clinical experience. Urology 2020; 141:173-7.
doi: S0090-4295(20)30261-2
pmid: 32171697
[8]
Kaouk J, Beksac AT, Abou Zeinab M, Duncan A, Schwen ZR, Eltemamy M. Single port transvesical robotic radical prostatectomy: initial clinical experience and description of technique. Urology 2021; 155:130-7.
doi: 10.1016/j.urology.2021.05.022
pmid: 34038749
[9]
Ng CF, Teoh JY, Chiu PK, Yee CH, Chan CK, Hou SS, et al. Robot-assisted single-port radical prostatectomy: a phase 1 clinical study. Int J Urol 2019; 26:878-83.
doi: 10.1111/iju.14044
pmid: 31257704
[10]
Gandaglia G, Martini A, Ploussard G, Fossati N, Stabile A, De Visschere P, et al. External validation of the 2019 Briganti nomogram for the identification of prostate cancer patients who should be considered for an extended pelvic lymph node dissection. Eur Urol 2020; 78:138-42.
doi: S0302-2838(20)30198-6
pmid: 32268944
[11]
Woodall WH, Rakovich G, Steiner SH. An overview and critique of the use of cumulative sum methods with surgical learning curve data. Stat Med 2021; 40:1400-13.
doi: 10.1002/sim.8847
pmid: 33316849
[12]
Lenfant L, Sawczyn G, Aminsharifi A, Kim S, Wilson CA, Beksac AT, et al. Pure single-site robot-assisted radical prostatectomy using single-port versus multiport robotic radical prostatectomy: a single-institution comparative study. Eur Urol Focus 2020; 7:964-72.
[13]
Rosenberg JE, Jung JH, Edgerton Z, Lee H, Lee S, Bakker CJ, et al. Retzius-sparing versus standard robotic-assisted laparoscopic prostatectomy for the treatment of clinically localized prostate cancer. Cochrane Database Syst Rev 2020; 8:CD013641. https://doi.org/10.1002/14651858.CD013641.pub2.