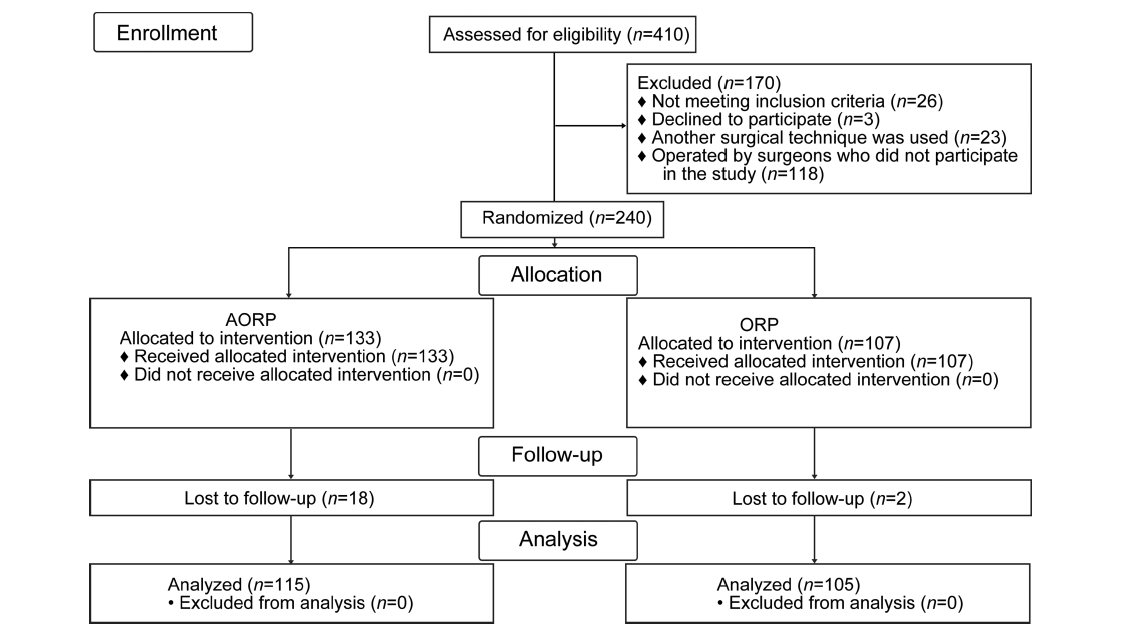
Objective: Radical prostatectomy is the recommended treatment for localized prostate cancer; however, it is an invasive procedure that can leave serious morbidity. Robot-assisted radical prostatectomy was introduced with the aim of reducing postoperative morbidity and facilitating rapid recovery compared to the traditional Walsh's open radical retropubic prostatectomy. Therefore, a protocol was developed to perform an open prostatectomy comparable to that performed by robotics, but without involving novel instrumentation. Methods: A total of 220 patients diagnosed with localized prostate cancer underwent radical prostatectomy. They were divided into two groups: anterograde technique (115 patients) and the retrograde method (105 patients). The study outcomes were observed 3 months after surgery. Results: No differences were found in terms of surgical time, hospital stay, and suction drainage. However, reduced bleeding was observed in the anterograde technique (p=0.0003), with rapid anastomosis duration (p=0.005). Among the patients, 60.9% undergoing the anterograde technique were continent 3 months after surgery compared to 42.9% treated by the retrograde method (p=0.007). Additionally, fewer complications in terms of the number (p=0.007) and severity (p=0.0006) were observed in the anterograde technique. Conclusion: The anterograde method displayed increased efficiency in reducing complications, compared to the retrograde technique.
. [J]. Asian Journal of Urology, 2023, 10(2): 151-157.
Fabricio B. Carrerette,Daniela B. Rodeiro,Rui T. F. Filho,Paulo A. Santos,Celso C. Lara,Ronaldo Damião. Randomized controlled trial comparing open anterograde anatomic radical retropubic prostatectomy with retrograde technique. Asian Journal of Urology, 2023, 10(2): 151-157.
Days with indwelling bladder catheter, median (IQR)
14 (14-15)
7 (7-7)
<0.0001a
Nerve sparing, n (%)
0.0009b
Absent
34 (32.4)
14 (12.2)
Unilateral
46 (43.8)
59 (51.3)
Bilateral
25 (23.8)
42 (36.5)
Surgical complication, n (%)
0.007b
Absent
76 (72.4)
100 (87.0)
Present
29 (27.6)
15 (13.0)
Clavien-Dindo classification, n (%)
0.0006b
Grade I
2 (1.9)
7 (6.1)
Grade II
18 (17.1)
3 (2.6)
Grade III
9 (8.6)
5 (4.3)
Gleason score, n (%)
0.11b
6
15 (14.3)
22 (19.1)
7
79 (75.2)
72 (62.6)
8 or 9
11 (10.5)
21 (18.3)
Pathologic stage, n (%)
0.22b
pT2a
4 (3.8)
11 (9.6)
pT2b
12 (11.4)
17 (14.8)
pT2c
68 (64.8)
60 (52.2)
pT3a
7 (6.7)
13 (11.3)
pT3b
14 (13.3)
14 (12.2)
Lymph node, n (%)
0.28b
Negative
65 (98.5)
82 (95.3)
Positive
1 (1.5)
4 (4.7)
Surgical margin, n (%)
T2 negative
64 (76.2)
66 (75.0)
0.85b
T2 positive
20 (23.8)
22 (25.0)
T3 negative
12 (57.1)
19 (70.4)
0.34b
T3 positive
9 (42.9)
8 (29.6)
Biochemical recurrence, n (%)
0.69b
Negative
94 (89.5)
101 (87.8)
Positive
11 (10.5)
14 (12.2)
Continence, n (%)
0.007b
Absent
60 (57.1)
45 (39.1)
Present
45 (42.9)
70 (60.9)
Sexual potency, n (%)
0.34b
Absent
94 (89.5)
98 (85.2)
Present
11 (10.5)
17 (14.8)
[1]
Cao L, Yang Z, Qi L, Chen M. Robot-assisted and laparoscopic vs. open radical prostatectomy in clinically localized prostate cancer: perioperative, functional, and oncological outcomes: a systematic review and meta-analysis. Medicine (Baltim) 2019; 98: e15770. https://doi.org/10.1097/MD.0000000000015770.
doi: 10.1097/MD.0000000000015770
[2]
Montorsi F, Wilson TG, Rosen RC, Ahlering TE, Artibani W, Carroll PR, et al. Best practices in robot-assisted radical prostatectomy: recommendations of the Pasadena Consensus Panel. Eur Urol 2012; 62:368-81.
doi: 10.1016/j.eururo.2012.05.057
pmid: 22763081
[3]
Walsh PC, Lepor H, Eggleston JC. Radical prostatectomy with preservation of sexual function: anatomical and pathological considerations. Prostate 1983; 4:473-85.
doi: 10.1002/pros.2990040506
pmid: 6889192
[4]
Guazzoni G, Cestari A, Naspro R, Riva M, Centemero A, Zanoni M, et al. Intra- and peri-operative outcomes comparing radical retropubic and laparoscopic radical prostatectomy: results from a prospective, randomised, single-surgeon study. Eur Urol 2006; 50:98-104.
pmid: 16563608
[5]
Ramsay C, Pickard R, Robertson C, Close A, Vale L, Armstrong N, et al. Systematic review and economic modelling of the relative clinical benefit and cost-effectiveness of laparoscopic surgery and robotic surgery for removal of the prostate in men with localised prostate cancer. Health Technol Assess 2012; 16:1-313.
doi: 10.3310/hta16410
pmid: 23127367
[6]
Campbell EW. Total prostatectomy with preliminary ligation of the vascular pedicles. J Urol 1959; 81:464-7.
doi: 10.1016/S0022-5347(17)66044-0
[7]
Ilic D, Evans SM, Allan CA, Jung JH, Murphy D, Frydenberg M. Laparoscopic and robotic-assisted versus open radical prostatectomy for the treatment of localised prostate cancer. Cochrane Database Syst Rev 2017; 9:CD009625. https://doi.org/10.1002/14651858.CD009625.pub2.
[8]
Yaxley JW, Coughlin GD, Chambers SK, Occhipinti S, Samaratunga H, Zajdlewicz L, et al. Robot-assisted laparoscopic prostatectomy versus open radical retropubic prostatectomy: early outcomes from a randomised controlled phase 3 study. Lancet 2016; 388:1057-66.
doi: S0140-6736(16)30592-X
pmid: 27474375
[9]
Ficarra V, Novara G, Fracalanza S, D’Elia C, Secco S, Iafrate M, et al. A prospective, non-randomized trial comparing robotassisted laparoscopic and retropubic radical prostatectomy in one European institution. BJU Int 2009; 104:534-9.
doi: 10.1111/bju.2009.104.issue-4
[10]
Carrerette FB, Dami?o R, da Silva EA, Figueiredo RT, Lara CC, Perroni F, et al. Description of the open anterograde anatomic radical retropubic prostatectomy technique. Surg Curr Res 2017; 7. https://doi.org/10.4172/2161-1076.1000304.
[11]
Carrerette FB, Carvalho E, Machado H, Freire FC, Dami?o R. Open anterograde anatomic radical retropubic prostatectomy technique: description of the first fifty-five procedures. Int Braz J Urol 2019; 45:1071-2.
doi: 10.1590/S1677-5538.IBJU.2018.0421
pmid: 30901175
[12]
Sciarra A, Cristini C, Von Heland M, Salciccia S, Gentile V. Randomized trial comparing an anterograde versus a retrograde approach to open radical prostatectomy: results in terms of positive margin rate. Can Urol Assoc J 2010; 4: 192-8.
doi: 10.5489/cuaj.851
[13]
Sciarra A, Gentile V, De Matteis A, Dattilo C, Autran Gomez AM, Salciccia S, et al. Long-term experience with an anatomical anterograde approach to radical prostatectomy: results in terms of positive margin rate. Urol Int 2008; 80:151-6.
doi: 10.1159/000112605
pmid: 18362484
[14]
Kwon SY, Lee JN, Ha YS, Choi SH, Kim TH, Kwon TG. Open radical prostatectomy reproducing robot-assisted radical prostatectomy: involving antegrade nerve sparing and continuous anastomosis. IBJU 2017; 43:1043-51.
[15]
Frota R, Turna B, Barros R, Gill IS. Comparison of radical prostatectomy techniques: open, laparoscopic and robotic assisted. Int Braz J Urol 2008; 34:259-69.
doi: 10.1590/s1677-55382008000300002
pmid: 18601755
[16]
Lowrance WT, Tarin TV, Shariat SF. Evidence-based comparison of robotic and open radical prostatectomy. ScientificWorldJournal 2010; 10:2228-37.
doi: 10.1100/tsw.2010.218
[17]
Tewari A, Takenaka A, Mtui E, Horninger W, Peschel R, Bartsch G, et al. The proximal neurovascular plate and the trizonal neural architecture around the prostate gland: importance in the athermal robotic technique of nerve-sparing prostatectomy. BJU Int 2006; 98:314-23.
doi: 10.1111/bju.2006.98.issue-2
[18]
Brunocilla E, Pultrone C, Pernetti R, Schiavina R, Martorana G. Preservation of the smooth muscular internal (vesical) sphincter and of the proximal urethra during retropubic radical prostatectomy: description of the technique. Int J Urol 2012; 19:783-5.
doi: 10.1111/j.1442-2042.2012.03028.x
pmid: 22515514
[19]
Van Velthoven RF, Ahlering TE, Peltier A, Skarecky DW, Clayman RV. Technique for laparoscopic running urethrovesical anastomosis: the single knot method. Urology 2003; 61:699-702.
doi: 10.1016/s0090-4295(02)02543-8
pmid: 12670546
[20]
Ozu C, Hagiuda J, Nakagami Y, Hamada R, Horiguchi Y, Yoshioka K, et al. Radical retropubic prostatectomy with running vesicourethral anastomosis and early catheter removal: our experience. Int J Urol 2009; 16:487-92.
doi: 10.1111/j.1442-2042.2009.02281.x
pmid: 19302506
[21]
Matsuyama H, Matsumoto H, Nagao K, Harada N, Hara T, Sakano S. Running suture versus interrupted suture for vesicourethral anastomosis in retropubic radical prostatectomy: a randomized study. Int J Urol 2015; 22:271-7.
doi: 10.1111/iju.12667
pmid: 25400263
[22]
Lim JH, Park CM, Kim HK, Park JY. Comparison of perioperative outcomes between running versus interrupted vesicourethral anastomosis in open radical prostatectomy: a single-surgeon experience. Kor J Urol 2015; 56:443-8.
[23]
Sridhar AN, Abozaid M, Rajan P, Sooriakumaran P, Shaw G, Nathan S, et al. Surgical techniques to optimize early urinary continence recovery post robot assisted radical prostatectomy for prostate cancer. Curr Urol Rep 2017; 18:71. https://doi.org/10.1007/s11934-017-0717-4.
doi: 10.1007/s11934-017-0717-4
pmid: 28718165
[24]
Tewari A, Sooriakumaran P, Bloch DA, Seshadri-Kreaden U, Hebert AE, Wiklund P. Positive surgical margin and perioperative complication rates of primary surgical treatments for prostate cancer: a systematic review and meta-analysis comparing retropubic, laparoscopic, and robotic prostatectomy. Eur Urol 2012; 62:1-15.
doi: 10.1016/j.eururo.2012.02.029
pmid: 22405509