Diagnostic value ultrasound signs of stones less than or equal to 10 mm and clinico-radiological variants of ureteric colic
Denis V. Krakhotkina*(),Volodymyr A. Chernylovskyib,Kemal Saricac,Arman Tsaturyand,Evangelos Liatsikosdef,Jurijus Makeviciusg,Nikolay Yu Iglovikovh,Dmitry N. Pikhovkini
a Central District Hospital, Outpatient Clinic, Sadovaya Lane 23, Kamenolomni, Rostov Region, Russia b Private Urological Practice, Dnipro, Ukraine c Department of Urology, Biruni University Hospital, Instanbul, Turkey d Department of Urology, University Hospital of Patras, Patras, Greece e Department of Urology, Medical University of Vienna, Vienna, Austria f Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia g Institute of Clinical Medicine, Faculty of Medicine, Vilnius University, Vilnius, Lithuania h Department and Clinic of Urology, S.M. Kirov Military Medical Academy of the Ministry of Defense of the Russian Federation, St. Petersburg, Russia i Central District Hospital, Department of Surgery, Lenina Avenue 28, Aksay, Rostov Region, Russia
Objective: To determine the diagnostic value of ultrasound signs of urinary stones less than or equal to 10 mm and to determine clinico-radiological variants of ureteric colic.
Methods: A total of 455 ultrasound investigations were performed in patients referring to emergency department with urolithiasis and symptoms suspected of ureteric colic between January 2021 and May 2021. In addition to microscopic evaluation of urine sediment to detect different crystals and non-contrast spiral computed tomography to detect stones, B-mode and color Doppler sonography was performed to assess the presence of acoustic shadow (AS) and twinkle artifacts (TA) as possible signs of stone(s) in ureter.
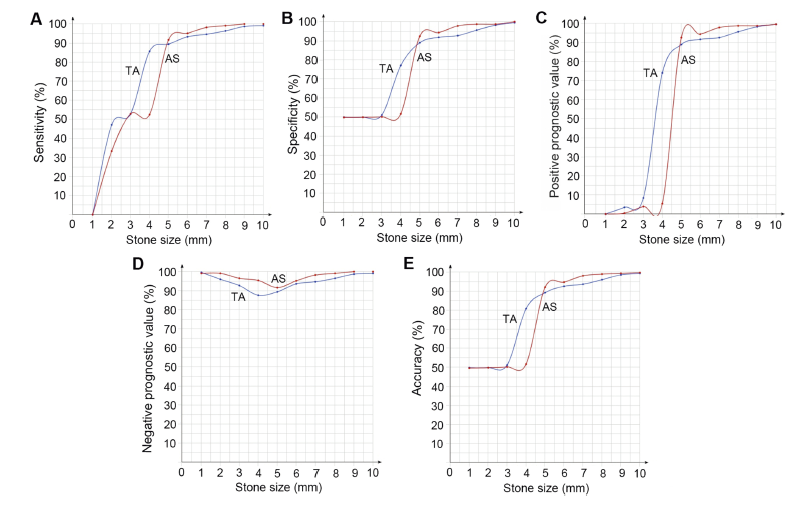
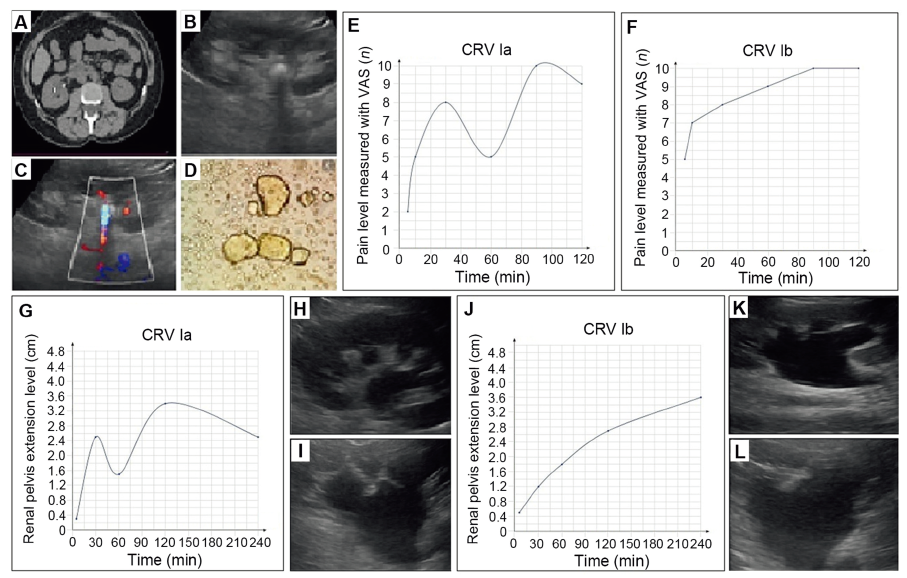
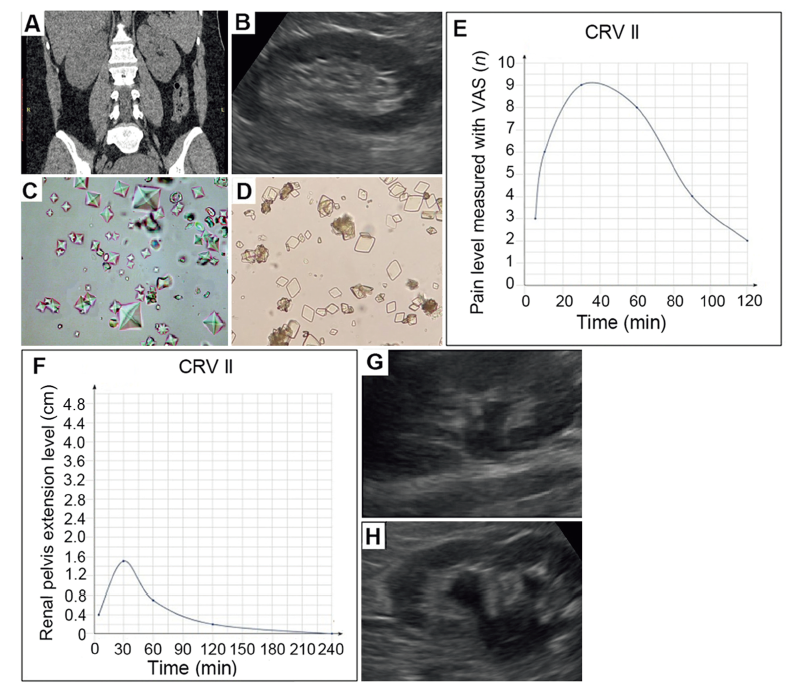
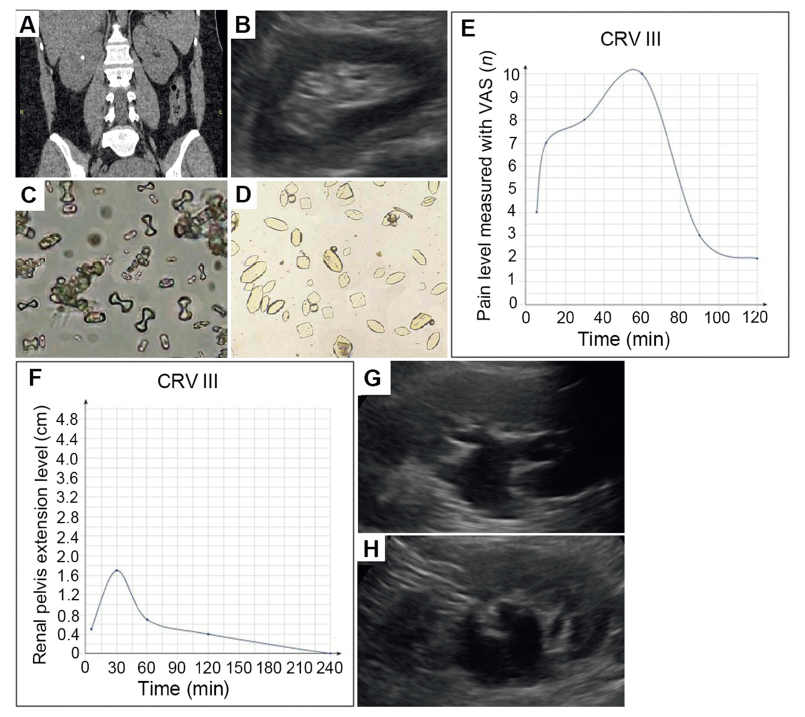
Results: While the sensitivity and specificity of AS and TA were higher than 90% in patients with stones greater than 5 mm; positive prognostic values of these parameters were found to be extremely low for stones with sizes of 1-3 mm with specificity and sensitivity values not exceeding 53%. The sensitivity and specificity of AS and TA in the upper and lower ureters were higher for stones greater than or equal to 5 than for compared to those less than 5 mm. At the same time, the diagnostic values of TA and AS for middle ureter stones were very limited. The most prevalent clinico-radiological variants of ureteric colic were types I, III, and V being observed in 39%, 28% and 21% cases, respectively.
Conclusion: Our results demonstrate that TA and AS parameters seem to have a very low sensitivity and specificity in the diagnosis of urinary stones less than 5 mm. The diagnostic value of TA and AS increase significantly in stones greater than or equal to 5 mm. Therefore, clinicians need to be very careful for overestimating the diagnostic values of TA and AS for stones less than 5 mm and non-contrast spiral computed tomography must be the method of choice for patients presenting to emergency department with ureteric colic.
. [J]. Asian Journal of Urology, 2023, 10(1): 39-49.
Denis V. Krakhotkin,Volodymyr A. Chernylovskyi,Kemal Sarica,Arman Tsaturyan,Evangelos Liatsikos,Jurijus Makevicius,Nikolay Yu Iglovikov,Dmitry N. Pikhovkin. Diagnostic value ultrasound signs of stones less than or equal to 10 mm and clinico-radiological variants of ureteric colic. Asian Journal of Urology, 2023, 10(1): 39-49.
Corbo J, Wang J. Kidney and ureteral stones. Emerg Med Clin 2009; 37:637e48.
[2]
Curhan GC. Epidemiology of stone disease. Urol Clin 2007; 34: 287e93.
[3]
Moore CL, Carpenter CR, Heilbrun ML, Klauer K, Krambeck AC, Moreno C, et al. Imaging in suspected renal colic: systematic review of the literature and multispecialty consensus. J Urol 2019; 202:475e83.
doi: 10.1097/JU.0000000000000342
pmid: 31412438
[4]
Brisbane W, Bailey MR, Sorensen MD. An overview of kidney stone imaging techniques. Nat Rev Urol 2016; 13:654e62.
doi: 10.1038/nrurol.2016.154
pmid: 27578040
[5]
Lazar M, Ringl H, Baltzer P, Toth D, Seitz C, Krauss B, et al. Protocol analysis of dual-energy CT for optimization of kidney stone detection in virtual non-contrast reconstructions. Eur Radiol 2020; 30:4295e305.
doi: 10.1007/s00330-020-06806-9
pmid: 32242275
[6]
Lim GS, Jang SH, Son JH, Lee JW, Hwang JS, Lim CH, et al. Comparison of non-contrast-enhanced computed tomography and intravenous pyelogram for detection of patients with urinary calculi. Korean J Urol 2014; 55:120e3.
doi: 10.4111/kju.2014.55.2.120
pmid: 24578808
[7]
Tzou DT, Usawachintachit M, Taguchi K, Chi T. Ultrasound use in urinary stones: adapting old technology for a modern-day disease. J Endourol 2017; 31:89e94.
doi: 10.1089/end.2016.0584
pmid: 27733052
[8]
Passerotti C, Chow JS, Silva A, Schoettler CL, Rosoklija I, Perez-Rossello J, et al. Ultrasound versus computerized to-mography for evaluating urolithiasis. J Urol 2009; 182:1829e34.
doi: 10.1016/j.juro.2009.03.072
pmid: 19692054
[9]
Bari V. Direct observation of procedural skills in radiology. AJR Am J Roentgenol 2010; 195:14e8.
[10]
Gulati M, Cheng J, Loo JT, Skalski M, Malhi H, Duddalwar V. Pictorial review: renal ultrasound. Clin Imag 2018; 51:133e54.
doi: S0899-7071(18)30043-3
pmid: 29477809
[11]
Smith-Bindman R, Aubin C, Bailitz J, Bengiamin RN, Camargo CA, Corbo J, et al. Ultrasonography versus computed tomography for suspected nephrolithiasis. N Engl J Med 2014; 371:1100e10.
doi: 10.1056/NEJMoa1404446
[12]
Rahmouni A, Bargoin R, Herment A, Bargoin N, Vasile N. Color Doppler twinkling artifact in hyperechoic regions. Radiology 1996; 199:269e71.
doi: 10.1148/radiology.199.1.8633158
pmid: 8633158
[13]
Korkmaz M, Aras B, Sanal B, Yücel M, Güneyli S, Ko?ak A, et al. Investigating the clinical signi?cance of twinkling artifacts in patients with urolithiasis smaller than 5 mm. Jpn J Radiol 2014; 32:482e6.
[14]
Gliga ML, Chirila CN, Podeanu DM, Imola T, Voicu SL, Gliga MG, et al. Twinkle, twinkle little stone: an artifact improves the ultrasound performance. Med Ultrason 2017; 19:272e5.
[15]
Abdel-Gawad M, Kadasne RD, Elsobky E, Ali-El-Dein B, Monga M. A prospective comparative study of color Doppler ultrasound with twinkling and noncontrast computerized to-mography for the evaluation of acute renal colic. J Urol 2016; 196:757e62.
doi: 10.1016/j.juro.2016.03.175
pmid: 27063853
[16]
Masch WR, Cohan RH, Ellis JH, Dillman JR, Rubin JM, Davenport MS. Clinical effectiveness of prospectively reported sonographic twinkling artifact for the diagnosis of renal cal-culus in patients without known urolithiasis. AJR Am J Roentgenol 2016; 206:326e31.
doi: 10.2214/AJR.15.14998
[17]
Puttmann K, Dajusta D, Rehfuss AW. Does twinkle artifact truly represent a kidney stone on renal ultrasound? J Pediatr Urol 2021; 17:475e6.
[18]
Dai JC, Dunmire B, Sternberg KM, Liu Z, Larson T, Thiel J, et al. Retrospective comparison of measured stone size and posterior acoustic shadow width in clinical ultrasound images. World J Urol 2018; 36:727e32.
doi: 10.1007/s00345-017-2156-8
pmid: 29243111
[19]
Durr-E-Sabih A, Khan AN, Craig M, Worrall JA. Sonographic mimics of renal calculi. J Ultrasound Med 2004; 23:1361e7.
pmid: 15448326
[20]
Fazil Marickar YM, Salim A, Vijay A. Stone symptoms and uri-nary deposits. Urol Res 2010; 38:65e9.
doi: 10.1007/s00240-009-0227-z
pmid: 19888570
[21]
Fan J, Chandhoke PS. Examination of crystalluria in freshly voided urines of recurrent calcium stone formers and normal individuals using a new ?lter technique. J Urol 1999; 161: 1685e8.
pmid: 10210440
[22]
Tamo?aityté S, Hendrixson V, ?elvys A, Tyla R, Ku?inskiené ZA, Jankevi?ius F, et al. Combined studies of chemical composi-tion of urine sediments and kidney stones by means of infrared microspectroscopy. J Biomed Opt 2013; 18: 27011.
doi: 10.1117/1.JBO.18.2.027011
[23]
Hsi RS, Dunmire B, Cunitz BW, He X, Sorensen MD, Harper JD, et al. Content and face validation of a curriculum for ultra-sonic propulsion of calculi in a human renal model. J Endourol 2014; 28:459e63.
doi: 10.1089/end.2013.0589