Prognostic role of platelet-to-lymphocyte ratio and neutrophil-to-lymphocyte ratio in patients with non-metastatic and metastatic prostate cancer: A meta-analysis and systematic review
Stefano Salcicciaa,Marco Frisendaa*(),Giulio Bevilacquaa,Pietro Viscusoa,Paolo Casaleb,Ettore De Berardinisa,Giovanni Battista Di Pierroa,Susanna Cattarinoa,Gloria Giorginoa,Davide Rosatia,Francesco Del Giudicea,Alessandro Sciarraa,Gianna Mariottia,Alessandro Gentiluccia
aDepartment of Urology, Sapienza Rome University, Policlinico Umberto I, 00161 Rome, Italy bDepartment of Urology, Humanitas, 20089 Rozzano, MI, Italy
Objective: To analyze data available in the literature regarding a possible prognostic value of the platelet-to-lymphocyte ratio (PLR) and neutrophil-to-lymphocyte ratio (NLR) in prostate cancer (PCa) patients stratified in non-metastatic and metastatic diseases.
Methods: A literature search process was performed following the Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines. In our meta-analysis, the pooled event rate estimated and the pooled hazard ratio were calculated using a random effect model.
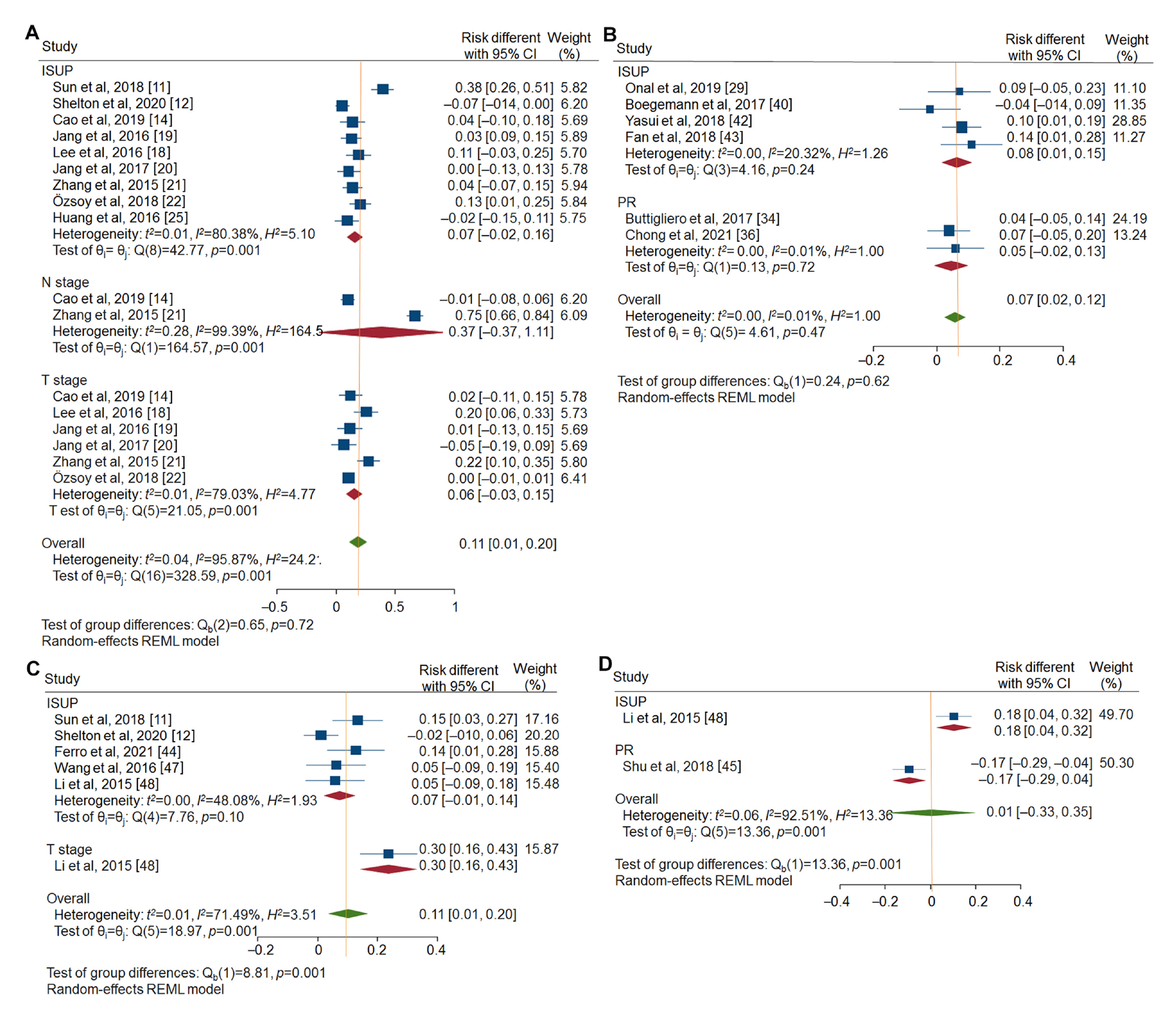
Results: Forty-two articles were selected for our analysis. The pooled risk difference for non-organ confined PCa between high and low NLR cases was 0.06 (95% confidence interval [CI]: −0.03-0.15) and between high and low PLR cases increased to 0.30 (95% CI: 0.16-0.43). In non-metastatic PCa cases, the pooled hazard ratio for overall mortality between high and low NLR was 1.33 (95% CI: 0.78-1.88) and between high and low PLR was 1.47 (95% CI: 0.91-2.03), whereas in metastatic PCa cases, between high and low NLR was 1.79 (95% CI: 1.44-2.13) and between high and low PLR was 1.05 (95% CI: 0.87-1.24).
Conclusion: The prognostic values of NLR and PLR in terms of PCa characteristics and responses after treatment show a high level of heterogeneity of results among studies. These two ratios can represent the inflammatory and immunity status of the patient related to several conditions. A higher predictive value is related to a high NLR in terms of risk for overall mortality in metastatic PCa cases under systemic treatments.
. [J]. Asian Journal of Urology, 2024, 11(2): 191-207.
Stefano Salciccia, Marco Frisenda, Giulio Bevilacqua, Pietro Viscuso, Paolo Casale, Ettore De Berardinis, Giovanni Battista Di Pierro, Susanna Cattarino, Gloria Giorgino, Davide Rosati, Francesco Del Giudice, Alessandro Sciarra, Gianna Mariotti, Alessandro Gentilucci. Prognostic role of platelet-to-lymphocyte ratio and neutrophil-to-lymphocyte ratio in patients with non-metastatic and metastatic prostate cancer: A meta-analysis and systematic review. Asian Journal of Urology, 2024, 11(2): 191-207.
Sciarra A, Voria G, Monti S, Mazzone L, Mariotti G, Pozza M, et al. Clinical understaging in patients with prostate adenocarcinoma submitted to radical prostatectomy: predictive value of serum chromogranin A. Prostate 2004; 58:421e8.
pmid: 14968443
[2]
Mottet N, van den Bergh RCN. Prostate cancer: European association of urology (EAU) guidelines. 2021. https://uroweb.org/guideline/prostate-cancer/. [Accessed 10 January 2022].
[3]
Briganti A, Larcher A, Abdollah F, Capitanio U, Gallina A, Suardi N, et al. Updated nomogram predicting lymph node invasion in patients with prostate cancer undergoing extended pelvic lymph node dissection: the essential importance of percentage of positive cores. Eur Urol 2012; 61:480. https://doi.org/10.1016/j.eururo.2011.10.044.
doi: 10.1016/j.eururo.2011.10.044
pmid: 22078338
[4]
Gandaglia G, Fosati N, Zaffuto E, Catellani M, Ferro M, Cordima G, et al. Development and internal validation of a novel model to identify the candidates for extended pelvic lymph node dissection in prostate cancer. Eur Urol 2017; 72: 632. https://doi.org/10.1016/j.urolonc.2020.11.040.
doi: S0302-2838(17)30280-4
pmid: 28412062
[5]
Shariat SF. Critical review of prostate cancer predictive tools. Future Oncol 2009; 5:1555e84.
doi: 10.2217/fon.09.121
pmid: 20001796
[6]
Sciarra A, Gentilucci A, Salciccia S, Pierella F, Del Bianco F, Gentile V, et al. Prognostic value of inflammation in prostate cancer progression and response to therapeutic: a critical review. J Inflamm 2016; 13:35. https://doi.org/10.1186/s12950-016-0143-2.
doi: 10.1186/s12950-016-0143-2
[7]
Murray NP, Fuentealba C, Salazar A, Reyes E. Platelet-tolymphocyte ratio and systemic immune-inflammation index versus circulating prostate cells to predict significant prostate cancer at first biopsy. Turk J Urol 2020; 46:115e22.
doi: 10.5152/tud.2020.19203
pmid: 32053099
[8]
Zanaty M, Ajib K, Alnazari M, El Rassy E, Aoun F, Zorn KC, et al. Prognostic utility of neutrophil-to-lymphocyte and platelets-to-lymphocyte ratio in predicting biochemical recurrence post robotic prostatectomy. Biomarkers Med 2018; 12:841e8.
doi: 10.2217/bmm-2017-0321
[9]
Wang J, Zhou X, He Y, Chen X, Liu N, Ding Z, et al. Prognostic role of platelet to lymphocyte ratio in prostate cancer: a meta-analysis. Medicine (Baltim) 2018; 97:e12504. https://doi.org/10.1097/MD.0000000000012504.
doi: 10.1097/MD.0000000000012504
[10]
Guo J, Fang J, Huang X, Liu Y, Yuan Y, Zhang X, et al. Prognostic role of neutrophil to lymphocyte ratio and platelet to lymphocyte ratio in prostate cancer: a meta-analysis of results from multivariate analysis. Int J Surg 2018; 60:216e23.
doi: S1743-9191(18)31714-X
pmid: 30468905
[11]
Sun Z, Ju Y, Han F, Sun X, Wang F. Clinical implications of pretreatment inflammatory biomarkers as independent prognostic indicators in prostate cancer. J Clin Lab Anal 2018; 32: e22277. https://doi.org/10.1002/jcla.22277.
doi: 10.1002/jcla.2018.32.issue-3
[12]
Shelton TM, Greenberg JW, Silberstein JL, Krane LS. Hematologic parameters are not predictors of upgrading or treatment in a racially diverse prospective study of men with prostate cancer on active surveillance. Aging Male 2020; 23: 1400e8.
doi: 10.1080/13685538.2020.1772227
[13]
Vidal AC, Howard LE, de Hoedt A, Cooperberg MR, Kane CJ, Aronson WJ, et al. Neutrophil, lymphocyte and platelet counts, and risk of prostate cancer outcomes in white and black men: results from the SEARCH database. Cancer Causes Control 2018; 29:581e8.
[14]
Cao Z, Ji J, Zhang C, Wang F, Xu H, Yu Y, et al. The preoperative neutrophil-to-lymphocyte ratio is not a marker of prostate cancer characteristics but is an independent predictor of biochemical recurrence in patients receiving radical prostatectomy. Cancer Med 2019; 8:1004e12.
doi: 10.1002/cam4.2019.8.issue-3
[15]
Nkengurutse G, Tian F, Jiang S, Wang Q, Wang Y, Sun W. Preoperative predictors of biochemical recurrence-free survival in high-risk prostate cancer following radical prostatectomy. Front Oncol 2020; 10:1761e9.
doi: 10.3389/fonc.2020.01761
pmid: 33014867
[16]
Taussky D, Soulieres D, Chagnon M, Delouya G, Bahig H. Systemic inflammatory markers are predictive of the response to brachytherapy in the prostate. Cells 2020; 9:2153e62.
doi: 10.3390/cells9102153
[17]
Langsenlehner T, Thurner EM, Krenn-Pilko S, Langsenlehner U, Stojakovic T, Gerger A, et al. Validation of the neutrophil-to-lymphocyte ratio as a prognostic factor in a cohort of European prostate cancer patients. World J Urol 2015; 33:1661e7.
doi: 10.1007/s00345-015-1494-7
pmid: 25617235
[18]
Lee H, Jeong SJ, Hong SK, Byun SS, Lee SE, Oh JJ. High preoperative neutrophil-lymphocyte ratio predicts biochemical recurrence in patients with localized prostate cancer after radical prostatectomy. World J Urol 2016 Jun; 34:821e7.
doi: 10.1007/s00345-015-1701-6
pmid: 26449784
[19]
Jang WS, Cho KS, Kim KHoon CY, Kang YJ, Lee JY, et al. Prognostic impact of preoperative neutrophil-to-lymphocyte ratio after radical prostatectomy in localized prostate cancer. Prostate Cancer Prostatic Dis 2016; 19:298e304.
doi: 10.1038/pcan.2016.20
[20]
Jang WS, Cho KS, Kim MS, Yoon CY, Kang DH, Kang YJ, et al. The prognostic significance of postoperative neutrophil-tolymphocyte ratio after radical prostatectomy for localized prostate cancer. Oncotarget 2017; 8:11778e87.
doi: 10.18632/oncotarget.14349
pmid: 28052031
[21]
Zhang GM, Zhu Y, Ma XC, Qin XJ, Wan FN, Dai B, et al. Pretreatment neutrophil-to-lymphocyte ratio: a predictor of advanced prostate cancer and biochemical recurrence in patients receiving radical prostatectomy. Medicine (Baltim) 2015; 94:e1473. https://doi.org/10.1097/MD.0000000000001473.
doi: 10.1097/MD.0000000000001473
[22]
?zsoy M, Moschini M, Fajkovic H, Soria F, Seitz C, Klatte T, et al. Elevated preoperative neutrophil-lymphocyte ratio predicts upgrading at radical prostatectomy. Prostate Cancer Prostatic Dis 2018; 21:100e5.
doi: 10.1038/s41391-017-0015-8
[23]
Adhyatma KP, Prapiska FF, Siregar GP, Siregar GP, Warli SM. Systemic inflammatory response in predicting prostate cancer: the diagnostic value of neutrophil-to-lymphocyte ratio. Open Access Maced J Med Sci 2019; 7:1628e30.
doi: 10.3889/oamjms.2019.177
pmid: 31210812
[24]
Masuda H, Mikami K, Otsuka K, Hou K, Suyama T, Araki K, et al. Validation of the effectiveness of neutrophil-to-lymphocyte ratio (NLR) as a predictive factor in patients undergoing prostate biopsy with prostate specific antigen (PSA) between 4.0 and 10.0 ng/mL. In Vivo 2021; 35:1641e6.
doi: 10.21873/invivo.12422
pmid: 33910847
[25]
Huang TB, Mao SY, Lu SM, Yu JJ, Luan Y, Gu X, et al. Predictive value of neutrophil-to-lymphocyte ratio in diagnosis of prostate cancer among men who underwent template-guided prostate biopsy: a STROBE-compliant study. Medicine (Baltim) 2016; 95:e5307. https://doi.org/10.1097/MD.0000000000005307.
doi: 10.1097/MD.0000000000005307
[26]
Oh JJ, Kwon O, Lee JK, Byun SS, Lee SE, Lee S, et al. Association of the neutrophil-to-lymphocyte ratio and prostate cancer detection rates in patients via contemporary multicore prostate biopsy. Asian J Androl 2016; 18:937e41.
doi: 10.4103/1008-682X.164198
[27]
Hashimoto M, Matsumura N, Ohzeki T, Hongo S, Sugimoto K, Shimizu N, et al. The change in neutrophil lymphocyte ratio from the first to the last repeat prostate biopsy proposed as a marker of carcinogenesis. Urol Int 2018; 101:74e9.
doi: 10.1159/000489400
pmid: 29909414
[28]
Lolli C, Caffo O, Scarpi E, Aieta M, Conteduca V, Maines F, et al. Systemic immune-inflammation index predicts the clinical outcome in patients with mCRPC treated with abiraterone. Front Pharmacol 2016; 7:376e82.
pmid: 27790145
[29]
Onal C, Sedef AM, Kose F, Oymak E, Guler OC, Sumbul AT, et al. The hematologic parameters in metastatic castrationresistant prostate cancer patients treated with abiraterone acetate. Future Oncol 2019; 15:1469e79.
doi: 10.2217/fon-2018-0635
pmid: 30977383
[30]
Bauckneht M, Rebuzzi SE, Signori A, Donegani MI, Murianni V, Miceli A, et al. The prognostic role of baseline metabolic tumor burden and systemic inflammation biomarkers in metastatic castration-resistant prostate cancer patients treated with Radium-223: a proof of concept study. Cancers 2020; 12: 3213e21.
doi: 10.3390/cancers12113213
[31]
Bauckneht M, Rebuzzi SE, Signori A, Frantellizzi V, Murianni V, Lodi Rizzini E, et al. The prognostic power of inflammatory indices and clinical factors in metastatic castration-resistant prostate cancer patients treated with radium-223 (BIO-Ra study). Eur J Nucl Med Mol Imag 2022; 49:1063e74.
doi: 10.1007/s00259-021-05550-6
[32]
Pei XQ, He DL, Tian G, Lv W, Jiang YM, Wu DP, et al. Prognostic factors of first-line docetaxel treatment in castrationresistant prostate cancer: roles of neutrophil-to-lymphocyte ratio in patients from Northwestern China. Int Urol Nephrol 2017; 49:629e35.
doi: 10.1007/s11255-017-1524-z
[33]
Sonpavde G, Pond GR, Armstrong AJ, Clarke SJ, Vardy JL, Templeton AJ, et al. Prognostic impact of the neutrophil-tolymphocyte ratio in men with metastatic castration-resistant prostate cancer. Clin Genitourin Cancer 2014; 12:317e24.
doi: 10.1016/j.clgc.2014.03.005
[34]
Buttigliero C, Pisano C, Tucci M, Vignani F, Bertaglia V, Iaconis D, et al. Prognostic impact of pretreatment neutrophil-to-lymphocyte ratio in castration-resistant prostate cancer patients treated with first-line docetaxel. Acta Oncol 2017; 56:555e62.
doi: 10.1080/0284186X.2016.1260772
pmid: 28068151
[35]
Kawahara T, Kato M, Tabata K, Kojima I, Yamada H, Kamihira O, et al. A high neutrophil-to-lymphocyte ratio is a poor prognostic factor for castration-resistant prostate cancer patients who undergo abiraterone acetate or enzalutamide treatment. BMC Cancer 2020; 20:919e26.
doi: 10.1186/s12885-020-07410-2
pmid: 32977754
[36]
Chong W, Zhang Z, Luo R, Gu J, Lin J, Wei Q, et al. Integration of circulating tumor cell and neutrophil-lymphocyte ratio to identify high-risk metastatic castration-resistant prostate cancer patients. BMC Cancer 2021; 21:655e61.
doi: 10.1186/s12885-021-08405-3
pmid: 34078304
[37]
Lorente D, Mateo J, Templeton AJ, Zafeiriou Z, Bianchini D, Ferraldeschi R, et al. Baseline neutrophil-lymphocyte ratio (NLR) is associated with survival and response to treatment with second-line chemotherapy for advanced prostate cancer independent of baseline steroid use. Ann Oncol 2015; 26:750e5.
doi: S0923-7534(19)31457-7
pmid: 25538172
[38]
Uemura K, Kawahara T, Yamashita D, Jikuya R, Abe K, Tatenuma T, et al. Neutrophil-to-lymphocyte ratio predicts prognosis in castration-resistant prostate cancer patients who received cabazitaxel chemotherapy. BioMed Res Int 2017; 2017:7538647. https://doi.org/10.1155/2017/7538647.
[39]
Templeton AJ, Pezaro C, Omlin A, McNamara MG, Leibowitz-Amit R, Vera-Badillo FE, et al. Simple prognostic score for metastatic castration-resistant prostate cancer with incorporation of neutrophil-to-lymphocyte ratio. Cancer 2014; 120: 3346e52.
doi: 10.1002/cncr.28890
pmid: 24995769
[40]
Boegemann M, Schlack K, Thomes S, Steinestel J, Rahbar K, Semjonow A, et al. The role of the neutrophil to lymphocyte ratio for survival outcomes in patients with metastatic castration-resistant prostate cancer treated with abiraterone. Int J Mol Sci 2017; 18:380e9.
doi: 10.3390/ijms18020380
[41]
Conteduca V, Caffo O, Galli L, Maugeri A, Scarpi E, Maines F, et al. Association among metabolic syndrome, inflammation, and survival in prostate cancer. Urol Oncol 2018; 36:e1e11. https://doi.org/10.1016/j.urolonc.2018.01.007.
[42]
Yasui M, Hasegawa Y, Kawahara T, Kumano Y, Miyoshi Y, Matsubara N, et al. Baseline neutrophil-to-lymphocyte ratio predicts the prognosis of castration-resistant prostate cancer treated with abiraterone acetate. Mol Clin Oncol 2018; 8: 587e91.
doi: 10.3892/mco.2018.1562
pmid: 29541468
[43]
Fan L, Wang R, Chi C, Cai W, Zhang Y, Qian H, et al. Systemic immune-inflammation index predicts the combined clinical outcome after sequential therapy with abiraterone and docetaxel for metastatic castration-resistant prostate cancer patients. Prostate 2018; 78:250e6.
doi: 10.1002/pros.23465
pmid: 29285775
[44]
Ferro M, Musi G, Matei DV, Mistretta AF, Luzzago S, Cozzi G, et al. Assessment of PSIM (prostatic systemic inflammatory markers) score in predicting pathologic features at robotic radical prostatectomy in patients with low-risk prostate cancer who met the inclusion criteria for active surveillance. Diagnostics 2021; 11:355e64.
doi: 10.3390/diagnostics11020355
[45]
Shu K, Zheng Y, Chen J, Li W, Jiang K. Prognostic value of selected preoperative inflammation-based scores in patients with high-risk localized prostate cancer who underwent radical prostatectomy. Onco Targets Ther 2018; 11:4551e8.
doi: 10.2147/OTT
[46]
Lee JW, Jeong H, Son H, Cho MC. Platelet-to-lymphocyte ratio is not a predictor of clinically significant prostate cancer at the prostate biopsy: a large cohort study. Sci Rep 2021; 11: 14240e52.
doi: 10.1038/s41598-021-93637-3
pmid: 34244550
[47]
Wang Y, Xu F, Pan J, Zhu Y, Shao X, Sha J, et al. Platelet to lymphocyte ratio as an independent prognostic indicator for prostate cancer patients receiving androgen deprivation therapy. BMC Cancer 2016; 16:329e36.
doi: 10.1186/s12885-016-2363-5
pmid: 27222030
[48]
Li F, Hu H, Gu S, Chen X, Sun Q. Platelet to lymphocyte ratio plays an important role in prostate cancer’s diagnosis and prognosis. Int J Clin Exp Med 2015; 8:11746e51.
[49]
Langsenlehner T, Pichler M, Thurer EM, Krenn-Pilko S, Stojakovic T, Gerger A, et al. Evaluation of the platelet-to-lymphocyte ratio as a prognostic indicator in a European cohort of patients with prostate cancer treated with radiotherapy. Urol Oncol 2015; 33:e9e201. https://doi.org/10.1016/j.urolonc.2015.02.002.
[50]
Adhyatma KP, Warli SM. Diagnostic value of platelet-tolymphocyte ratio in prostate cancer. Open Access Maced J Med Sci 2019; 7:1093e6.
doi: 10.3889/oamjms.2019.252
[51]
Shi X, Fan J, Pei X, Wang Y, Guo G, Yang T, et al. Inflammatory factor-based prognostic risk stratification for patients with metastatic castration-resistant prostate cancer treated with docetaxel. Andrologia 2021; 53:e14064. https://doi.org/10.1111/and.14064.