Long-term outcomes of urethral balloon dilation for anterior urethral stricture: A prospective cohort study
Ahmed M. Abdel Gawadab,Abhijit Patila,Abhishek Singha,Arvind P. Ganpulea*(),Ravindra B. Sabnisa,Mahesh R. Desaia
aDepartment of Urology, Muljibhai Patel Urological Hospital, Nadiad, India bDepartment of Urology, Faculty of Medicine, Al-Azhar University, Damietta, Egypt
Objective: To prospectively follow up a cohort of anterior urethral stricture disease patients managed with balloon dilation (BD) for 3 years to evaluate the long-term outcomes and to study factors that contribute to recurrence.
Methods: This study included men who had urethral BD for significant anterior urethral stricture disease between January 2017 and March 2019. Data about the patient age, stricture characteristics, and recurrence date were recorded, along with information on postoperative indwelling catheter use and operative complications. Furthermore, information about the self-calibration procedure was collected and where available, free flow (FF) measurements during the follow-up period were recorded and analyzed. Success was defined as a lack of symptoms and acceptable FF rates (maximum flow rate>12 mL/s).
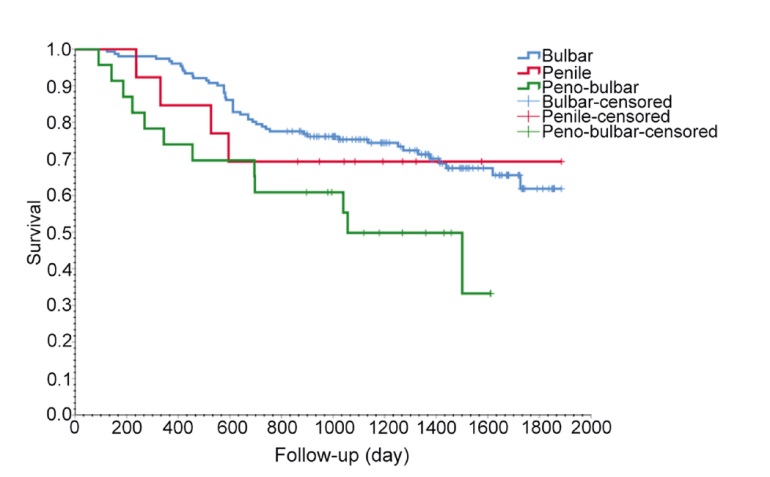
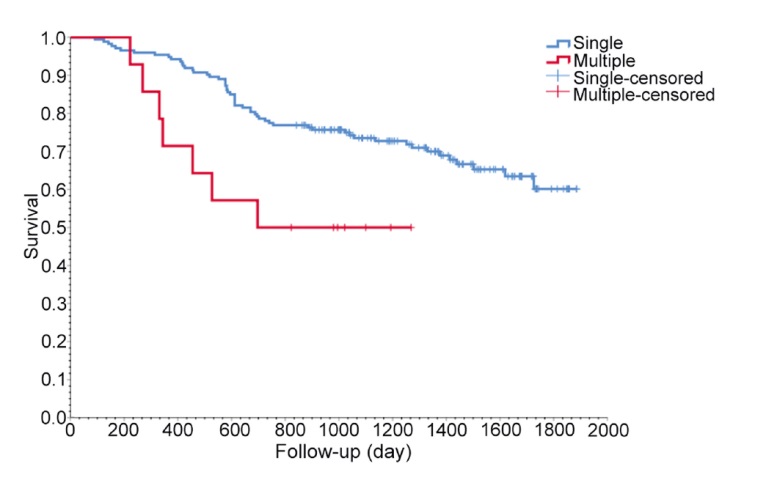
Results: The final analysis was conducted on 187 patients. The mean follow-up period was 37 months. The long-term overall success rate at the end of our study was 66.8%. Our recurrence rate was 7.4% at 12 months, 24.7% at 24 months, and reached 33.2% at the end of our study. The time to recurrence ranged from 91 days to 1635 days, with a mean of 670 days. The stricture-free survival was significantly shorter with lengthy peno-bulbar (p=0.031) and multiple strictures (p=0.015), and in the group of patients who were not committed to self-calibration protocol (p<0.011). However, post-procedural self-calibration was the most important factor that may have decreased the incidence of recurrence (odds ratio=5.85). Adjuvant self-calibration after BD not only reduced the recurrence rate from 85.4% in the non-self-calibration group to 15.1% in the self-calibration one (p<0.001), but also improved the overall stricture-free survival and FF parameters.
Conclusion: Urethral BD has a high recurrence rate in the long-term, especially with long and multiple strictures. Adjuvant self-calibration has proven to reduce the recurrence risk and the need for re-intervention.
. [J]. Asian Journal of Urology, 2024, 11(3): 480-485.
Ahmed M. Abdel Gawad, Abhijit Patil, Abhishek Singh, Arvind P. Ganpule, Ravindra B. Sabnis, Mahesh R. Desai. Long-term outcomes of urethral balloon dilation for anterior urethral stricture: A prospective cohort study. Asian Journal of Urology, 2024, 11(3): 480-485.
Length of catheter stay post-operatively, median (range), day
2 (1-3)
Self-calibration, n (%)
Yes
139 (74.3)
No
48 (25.7)
Procedural failure, n (%)
Primary
9 (4.8)
Overall
62 (33.2)
Need for auxiliary procedure, n (%)
47 (25.1)
BD
32 (17.1)
BD and D-VIU
5 (2.7)
Urethroplasty
10 (5.3)
FU, mean±SD, day
1127.95±467.69
Time to recurrence, mean (SD; range), day
670 (392; 91-1635)
FF parameter
Pre-procedure
At 1 month after procedure
At the end of FU period
Qmax, mL/s
4.95±2.35
23.23±8.71
16.11±7.33
VV, mL
190.59±122.49
306.35±148.49
277.76±140.71
PVR urine volume, mL
74.53±70.07
30.81±22.14
41.49±38.01
Variable
Failure, n
Total, n
p-Value
No
Yes
Etiology
0.279
Iatrogenic
58
22
80
Inflammatory
2
3
5
Traumatic
2
1
3
Unspecified
61
38
99
Site
0.153
Bulbar
103
48
151
Penile
9
4
13
Peno-bulbar
11
12
23
Single or multiple
0.196
Single
116
57
173
Multiple
7
7
14
Primary or recurrent
0.521
Primary
112
60
172
Recurrence
11
4
15
Stricture grade
0.581
2
2
1
3
3
78
37
115
4
42
27
69
Self-calibration
<0.001
No
7
41
48
Yes
116
23
139
[1]
Palminteri E, Berdondini E, Verze P, De Nunzio C, Vitarelli A, Carmignani L. Contemporary urethral stricture characteristics in the developed world. Urology 2013; 81:191-6.
[2]
Kulkarni SB, Bhat A, Bhatyal HS, Sharma GR, Dubey DD, Khattar N, et al. The Urological Society of India guidelines for the management of urethral stricture (executive summary). Indian J Urol 2021; 37:6-9.
[3]
Pang KH, Chapple CR, Chatters R, Downey AP, Harding CK, Hind D, et al. A systematic review and meta-analysis of adjuncts to minimally invasive treatment of urethral stricture in men. Eur Urol 2021; 80:467-79.
[4]
Isen K, Nal?ac?o?lu V. Direct vision internal urethrotomy by using endoscopic scissors. Int Urol Nephrol 2015; 47:905-8.
[5]
Yu SC, Wu HY, Wang W, Xu LW, Ding GQ, Zhang ZG, et al. Highpressure balloon dilation for male anterior urethral stricture: single-center experience. J Zhejiang Univ Sci B 2016; 17:722-7.
[6]
Campos-Juanatey F, Osman NI, Greenwell T, Martins FE, Riechardt S, Waterloos M, et al. European Association of Urology guidelines on urethral stricture disease (part 2): diagnosis, perioperative management, and follow-up in males. Eur Urol 2021; 80:201-12.
[7]
Angermeier KW, Rourke KF, Dubey D, Forsyth RJ, Gonzalez CM. SIU/ICUD consultation on urethral strictures: evaluation and follow-up. Urology 2014; 83(Suppl. 3):S8-17. https://doi.org/10.1016/j.urology.2013.09.011
doi: https://doi.org/10.1016/j.urology.2013.09.011
[8]
Lauritzen M, Greis G, Sandberg A, Wedren H, Ojdeby G, Henningsohn L. Intermittent self-dilatation after internal urethrotomy for primary urethral strictures: a case-control study. Scand J Urol Nephrol 2009; 43:220-5.
[9]
Lumen N, Hoebeke P, Willemsen P, De Troyer B, Pieters R, Oosterlinck W. Etiology of urethral stricture disease in the 21st century. J Urol 2009; 182:983-7.
[10]
Singh J, Priyadarshi V, Pandey P. Urethral stricture etiology revisited: an Indian scenario. UroToday Int J 2013 ;6. https://doi.org/10.3834/uij.1944-5784.2013.02.05
doi: https://doi.org/10.3834/uij.1944-5784.2013.02.05
[11]
Stein DM, Thum DJ, Barbagli G, Kulkarni S, Sansalone S, Pardeshi A, et al. A geographic analysis of male urethral stricture aetiology and location. BJU Int 2013; 112:830-4.
[12]
Pickard R, Goulao B, Carnell S, Shen J, MacLennan G, Norrie J, et al. Open urethroplasty versus endoscopic urethrotomy for recurrent urethral stricture in men: the OPEN RCT. Health Technol Assess 2020; 24:1-110.
[13]
Steenkamp JW, Heyns CF, de Kock ML. Internal urethrotomy versus dilation as treatment for male urethral strictures: a prospective, randomized comparison. J Urol 1997; 157:98-101.
[14]
Pansadoro V, Emiliozzi P. Internal urethrotomy in the management of anterior urethral strictures: long-term followup. J Urol 1996; 156:73-5.
[15]
Mangir N, Chapple C. Recent advances in treatment of urethral stricture disease in men. F1000Res 2020; 9:F1000 Faculty Rev-330. https://doi.org/10.12688/f1000research.21957.1
doi: https://doi.org/10.12688/f1000research.21957.1
[16]
Vyas JB, Ganpule AP, Muthu V, Sabnis RB, Desai MR. Balloon dilatation for male urethral strictures “revisited”. Urol Ann 2013; 5:245-8.
[17]
Chhabra JS, Balaji SS, Singh A, Mishra S, Ganpule AP, Sabnis RB, et al. Urethral balloon dilatation: factors affecting outcomes. Urol Int 2016; 96:427-31.
[18]
Tunc M, Tefekli A, Kadioglu A, Esen T, Uluocak N, Aras N. A prospective, randomized protocol to examine the efficacy of postinternal urethrotomy dilations for recurrent bulbomembranous urethral strictures. Urology 2002; 60:239-44.