|
|
|
| Updates in the use of radiotherapy in the management of primary and locally-advanced penile cancer |
Akshar Patela,Arash O. Naghavib,Peter A. Johnstoneb,Philippe E. Spiessc,G. Daniel Grassb,*( ) )
|
aUniversity of South Florida Morsani College of Medicine, Tampa, FL, USA
bDepartment of Radiation Oncology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL, USA
cDepartment of Genitourinary Oncology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL, USA |
|
|
|
|
Abstract Objective: Penile cancer is a rare malignancy in most developed countries, but may represent a significant oncologic challenge in certain African, Asian, and South American regions. Various treatment approaches have been described in penile cancer, including radiotherapy. This review aimed to provide a synopsis of radiotherapy use in penile cancer management and the associated toxicities. In addition, we aimed to discuss palliative radiation for metastases to the penis and provide a brief overview of how tumor biology may assist with treatment decision-making. Methods: Peer-reviewed manuscripts related to the treatment of penile cancer with radiotherapy were evaluated by a PubMed search (1960-2021) in order to assess its role in the definitive and adjuvant settings. Selected manuscripts were also evaluated for descriptions of radiation-related toxicity. Results: Though surgical resection of the primary is an excellent option for tumor control, select patients may be treated with organ-sparing radiotherapy by either external beam radiation or brachytherapy. Data from randomized controlled trials comparing radiotherapy and surgery are lacking, and thus management is frequently determined by institutional practice patterns and available expertise. Similarly, this lack of clinical trial data leads to divergence in opinion regarding lymph node management. This is further complicated in that many cited studies evaluating lymph node radiotherapy used non-modern radiotherapy delivery techniques. Groin toxicity from either surgery or radiotherapy remains a challenging problem and further risk assessment is needed to guide intensification with multi-modal therapy. Intrinsic differences in tumor biology, based on human papillomavirus infection, may help aid future prognostic and predictive models in patient risk stratification or treatment approach. Conclusion: Penile cancer is a rare disease with limited clinical trial data driving the majority of treatment decisions. As a result, the goal of management is to effectively treat the disease while balancing the importance of quality of life through integrated multidisciplinary discussions. More international collaborations and interrogations of penile cancer biology are needed to better understand this disease and improve patient outcomes.
|
|
Received: 12 November 2021
Available online: 20 October 2022
|
|
Corresponding Authors:
G. Daniel Grass
E-mail: daniel.grass@moffitt.org
|
|
|

| Study | Pts, n | RT dose, Gy | Median follow-up, month | 5-year LC, % | 5-year CSS, % | 5-year penile preservation, % | Stenosis or necrosis rate | Tumor characteristic | Tumor location | | McLean et al., 1993 [22] | 26 | 35 Gy/10 fx;
60 Gy/25 fx | 116 | 61 | 69 | 66 | ?
NR (seven Pts with late complications) | ?
73.1% T1; 15.3% T2; 7.7% T3; 3.9% T4 | ?
65% glans or prepuce; 4% shaft; 31% multiple sites | | Sarin et al., 1997 [29] | 59 | 60 Gy/30 fx | 62 | 55 | 66 | 50 | ?
3% necrosis; 14% stenosis | ?
86.4% T1; 8.5% T2; 1.7% T3; 3.4% T4 | ?
In 101 Pts, 78% were confined to glans; only 59 received EBRT | | Gotsadze et al., 2000 [25] | 155 | 40-60 Gy | 40 | 65 | 86 | 65 | ?
1% necrosis; 7% stenosis | ?
36.8% T1; 55.5% T2; 7.7% T3; | ?
NR | | Zouhair et al., 2001 [27] | 23 | 45-74 Gy/25-37 fx | 12 | 41 | NR | 36 | ?
10% stenosis | ?
29% T1; 59% T2; 10% T3; 2% Tx | ?
In 41 Pts: 41% glans; 22% prepuce; 20% shaft; 10% corona; 5% prepuce or glans; 2% prepuce or shaft | | Azrif et al., 2006 [24] | 41 | 50.0-52.5 Gy/16 fx | 41 | 62 | 96 | 62 | ?
8% necrosis; 29% stenosis | ?
90.2% T1; 9.8% T2 | ?
98% glans/prepuce | | Ozsahin et al., 2006 [23] | 21 | 52 Gy | 62 | 49 | NR | 52 | ?
10% stenosis | ?
37% T1; 53% T2; 8% T3; 2% Tx | ?
In 60 Pts: 40% glans; 26% prepuce; 22% shaft; 7% corona;
3% prepuce/glans; 1% prepuce/shaft | | Mistry et al., 2007 [26] | 18 | 55 Gy/16 fx?50 Gy/20fx | 62 | 63 | NR | 62 | ? 10% necrosis;
5% stenosis | ?
23.5% Tx; 17.6% in situ; 35.3% T1; 17.6% T2; 6% T3 | ?
In 65 Pts: 76% were on glans/prepuce; 5% on shaft |
|
|
Use of EBRT in definitive management of primary penile squamous cell carcinoma.
|
| Study | Brachytherapy type | Patient, n | RT dose, median (range), Gy | Follow-up, median (range), month | 5-year LC, % | 5-year CSS, % | 5-year penile preservation, % | Stenosis or necrosis rate | Tumor characteristic | | Crook et al., 2005 [38] | Pulsed dose rate | 49 | 60 (NR) | 33.4 (4.0-140.0) | 85.3 | 90 | 86.5 | ?
16% necrosis; 12% stenosis | ?
51% T1; 33% T2; 8% T3; 4% Tx; 4% in situ | | Crook et al., 2009 [28] | Pulsed dose rate/low dose rate | 67 | 60 | 48.0 (2.4-194.4) | 87.3 | 83.6 | 88.0 | ?
16% necrosis; 12% stenosis | ?
56% T1; 33% T2; 8% T3; 3% Tx | | de Crevoisier et al., 2009 [41] | Low dose rate | 144 | 65 (37-75) | 68.4 (6.0-348.0) | 80.0 (at 10 years) | 92.0 (at 10 years) | 7.0 (at 10 years) | ?
26% necrosis; 29% stenosis | ?
Confined to glans, N0 | | Pimenta et al., 2015 [42] | Low dose rate | 25 | 60 (50-65) | 110.4 (0.0-228.0) | NR | 91.3 (at 5 years and 10 years) | 86.1 | ?
0% necrosis; 43% stenosis | ?
T1-T2 | | Cordoba et al., 2016 [40] | Low dose rate | 73 | 60 (40-70) | 51.0 (33.4-68.7) | NR | 91.4 | 87.6 | ?
6.8% necrosis; 6.6% stenosis | ?
91.8% of lesions on glans | ?
75.3% T1 lesions; 15% T2; 1.3% Tx | | Kellas-Sleczka et al., 2019 [44] | High dose rate | 76 | 28?54.8a (median EQD2);47.4?55.1b (median EQD2) | 76.0 (7.0-204.0) | 65.6 | 85.0 | 69.5 | ?
2.6% necrosis; 1.3% stenosis | ?
11.8% in situ; 46.1% T1; 21.1% T2; 9.2% T3; 11.8% Tx | | Martz et al., 2021 [10] | High dose rate | 29 | 36 (31-39) | 72.4 (3-174) | 82.0 | 88.0 | 79.3 | ?
10.3% necrosis; 17% telangiectasia | ?
T1-T2, N0-N2, M0 |
|
|
Use of brachytherapy in management of primary penile squamous cell carcinoma.
|
|
|
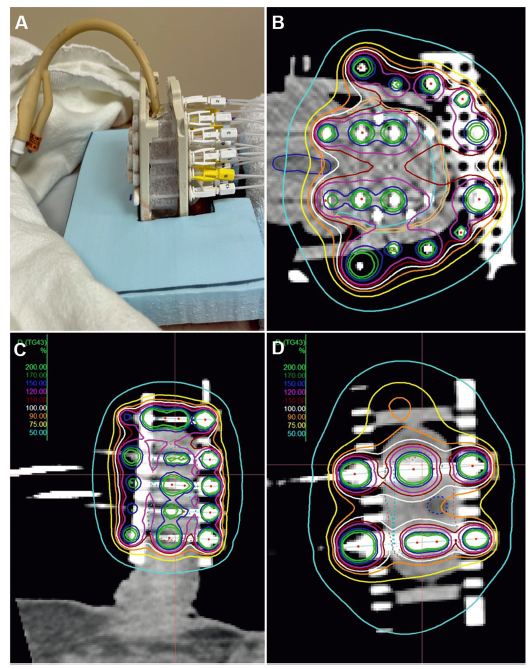
High dose rate interstitial penile brachytherapy. (A) Example of a mobile hybrid implantation with interstitial catheters, bolus with external catheters to supplement superficial dose and aid in homogeneity, along with a foley in place during the duration of the implant; (B-D) Treatment planning of a bilateral glans tumor. (B) Axial; (C) Sagittal; (D) Coronal. Note the catheter spacing and dosing, limiting the V150 (blue) and V200 (green) volume to mitigate stenosis/necrosis risk. Note the catheter spacing from the urethra/meatus and supplementing dose from outside of the bolus, allowing a homogenous plan and limiting urethral toxicity. Note the supplemental dose from outside the template contributing to the target volume.
|
| Study | Treatment years | Patient, n | LND, n | EBRT, n | Age, median (IQR), year | Median follow-up, month | Chemotherapy, n or % | Adjuvant EBRT target | | Demkow, 1999 [75] | 1989-1994 | 64 | 35 | 12 | 64 (21-86) | 33.0 | NACT: 2;
CCRT: 3 | NR | | Zouhair et al., 2001 [27] | 1962-1994 | 41 | 5 | 14 | 59 (35-75) | 70.0 | No | ILN | | Chen et al., 2004 [108] | 1989-2000 | 45 | 19 | 9 | 64 (29-87) | 37.0 | CT: 1 | Primary/bilateral ILN and lower iliac LN | | Langsenlehner et al., 2008 [52] | 1987-2006 | 24 | 8 | Penis/surgical stump (n=14); ILN (n=8) | 62.7 (35.5-90.4) | 58.4 | No | Penis/stump/ILN & iliac nodes | | Franks et al., 2011 [77] | 2002-2008 | 23 | 14 | 14 | 58 (40-81) | 27.0 | No | Bilateral ILN and PLN | | Graafland et al., 2011 [73] | 1988-2007 | 161 | 161 | 67 | 64 (33-91) | 60.0 | NACT: 4 | Ipsilateral ILN ± PLN | | Tang et al., 2017 [84] | 1980-2013 | 92 | 92 | 40 | 65.3 (53-70) | 9.3 | Perioperative CT: 27 | Bilateral PLN | | Winters et al., 2018 [68] | 1998-2012 | 589 | 589 | 136 | 61.8 (NR) | NR | Perioperative CT: 169 | ILN + PLN | | Johnstone et al., 2019 [85] | Multi-institutional (NR) | 93 | 93 | 58 | 65.3 (36-90) | 9.4 | Perioperative CT: 46 | ILN ± PLN (ipsilateral if involved) | | Ager et al., 2021 [87] | 2002-2017 | 146 | 146 | 121 | 59 (54-70) | 10.6 | CCRT: 41% | Ipsilateral ILN ± pelvic LN | | Choo et al., 2020 [89] | 1995-2015 | 23 | 23 | 11 | 57 (43-68) | 15.8 | CCRT: 11 | Bilateral ILN & PLN | | Li et al., 2021 [91] | 2003-2015 | 93 | 93 | 32 | 49 (NR) | 8.8 | CCRT: 34% | NR | | Jaipuria et al., 2020 [90] | 2011-2017 | 45 | 45 | 31 | 56 (45-67) | 12.5 | CCRT: 6 | Bilateral ILN and PLN + suprapubic region | | Yuan et al., 2020 [123] | 1999-2016 | 51 | 47 | 19 | 61 (37-91) | 36.6 | CCRT: 17;
CT alone: 20 | PLN (n=15);
ILN (n=13) | | Mittal et al., 2021 [78] | 2014-2017 | 14 | 14 | 14 | NR | 24.0 | CT: 14 | Bilateral ILN ± PLN | | Khurud et al., 2022 [88] | 2010-2018 | 128 | 128 | 78 | 57 (50-65) | 22.0 | CT alone: 19%;
CCRT: 13%;
CT into EBRT: 24%;
CT into CCRT: 12% | Variable: involved ILN and PLN (68%); involved & uninvolved ILN + PLN (32%) | | Demkow, 1999 [75] | ≥2 ILNs or ENE | NR | NR | NR | NR (3-yr: 76%) | NR | NR | LR: 11% (entire cohort) | | Zouhair et al., 2001 [27] | (+) surgical margins or lymph node involvement | Parallel opposed AP/PA fields (18 MV); e-field boost for positive nodes | 36-66 Gy/20-36 fx | NR | 57% | 48% | NR | pN2: 7%; pN3: 1% | | Chen et al., 2004 [108] | pN+ | Parallel opposed AP/PA field | 40-70 Gy/20-35 fx | NR | 54.30% | NR (3-yr: 89% [AIRT group]) | Grade 3 lymphedema: 22% (AIRT); radionecrosis of inguinal region: 11% (AIRT group) | pN+ (n=17) | | Langsenlehner et al., 2008 [52] | (+) surgical margins and pN+ | Parallel opposed AP/PA fields; e-field boost for positive nodes | 45-60 Gy/25-60 fx | 84.30% | 56.60% | 100% with AIRT | 10% with persistent lymphedema | Of 12 patients with cN+, definitive EBRT to ILN resulted in 5-yr regional control of 92% | | Franks et al., 2011 [77] | pN2/3 or ENE | Parallel opposed AP/PA fields; e-field boost for positive nodes | Phase I: 45 Gy/20 fx;Phase II: 12 Gy/5 fx (boost if needed) | NR | NR (3-yr: 66%) | NR (3-yr: 56%) | Scrotal/penile/lower leg lymphedema: 6 | Locoregional relapse-free survival: 56% | | Graafland et al., 2011 [73] | ≥2 ILNs or ENE | NR | 50 Gy/25 fx | NR | NR | NR | NR | 5-yr ILN recurrence: 16% | | Tang et al., 2017 [84] | pN3 | NR | 50 Gy/25 fx (n=27);<40 Gy (n=4);>50 Gy (n=5) | 14.4 months | 12.2 months | Adjuvant EBRT with better median time to recurrence (7.7 vs. 5.3 months) | NR | Median PLN+ (n=2);ENE+ in PLN (n=39) | | Winters et al., 2018 [68] | NR | NR | 75% received ≥45 Gy | NR | 64% | NR | NR | pN2 (n=433) | | Johnstone et al., 2019 [85] | ≥2 ILNs or ENE | NR | 50 Gy in 25 fx | NR | Median OS: 10.6 months | NR | NR | Median ILN+ (n=4), 72% ENE; median PLN+ (n=2), 49% ENE; median DSS: 11 months | | Ager et al., 2021 [87] | pN3 | NR | Variable:
45 Gy/20 fx;
54 Gy/27 fx;
50-54 Gy/25-27 fx | 51% | 44% | 56% | NR | ENE: 99% (ILN: 74%; PLN: 25%);
5-yr RFS: 51%; in-field recurrence: 47% | | Choo et al., 2020 [89] | Regional LN+ | NR | 45 Gy/25 fx (uninvolved LN);
56 Gy/28 fx (involved LN) | NR (2-yr: 49.3%) | NR (2-yr: 25%) | NR (2-yr: 27%) | Lymphedema: 46%; necrosis: 9% | pN3: 43% | | Li et al., 2021 [91] | pN3 | Parallel opposed AP/PA fields (equally weighted) | 30-68 Gy/15-34 fx | NR (3-yr CSS: 28.5% [CCRT] vs. 16.2% [CT]) | NR | NR | NR | 21% CCRT underwent salvage surgery | | Jaipuria et al., 2020 [90] | ≥2 ILNs ± PLN ± ENE | IMRT/VMAT | 45 Gy/25 fx (pelvis);
54 Gy (ENE+ region);
57-60 Gy (gross residual) | NR | Mean OS: 3.9 yr (RT);
mean OS: 2.8 yr (Chemo);
median OS not met in PLN-cohort | NR | 39% of RT group with persistent lymphedema; no RT-related necrosis | Pelvic LN+ (n=13);
ENE: 78% | | Yuan et al., 2020 [123] | NR | NR | 39.6-54 Gy/22-30 fx (PLN);
42.5-64.8 Gy (ILN) | NR | NR | 2-yr: 54% | G2 skin: 18% (acute);
G2 GI; 12% (acute);
G1 lymphedema: 18% (late) | N2/3 (n=23);
ENE+: 12% | | Mittal et al., 2021 [78] | pN3 | IMRT | 50 Gy/25 fx | NR | NR (2-yr: 79%) | NR (2-yr: 79%) | G2 lymphedema: 29%;
G3 lymphedema: 0% | 93% received adjuvant and CCRT | | Khurud et al., 2022 [88] | pN3 | Conventional (54%);
3DCRT (26%);
IMRT (20%); | 45 Gy/25 fx;
50.4 Gy/28 fx;
50 Gy/25 fx | NR | NR (2-yr: 62%) | NR (2-yr: 83% [multi-modal]) | 45% of AIRT group with lymphedema | 2-yr DFS: 55% |
|
|
Select studies evaluating adjuvant EBRT ± chemotherapy to the groin or pelvis.
|
|
|
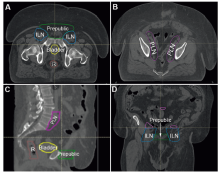
Adjuvant EBRT to prepubic fat and bilateral ILNs and PLNs. Case of a 55-year-old male with hrHPV? pT3 N3 M0 poorly differentiated PSCC of the glans status post partial penectomy with mons panniculectomy requiring reconstruction with split thickness graft. Approximately 2 months later he underwent bilateral superficial and deep ILN dissection with pathology demonstrating negative margins at the primary site and 3/15 ILNs involved with malignancy with evidence of bilateral ENE. (A and B) Axial slices showing the prepubic space (green), bilateral ILNs (blue), and bilateral PLNs (pink) clinical target volumes; (C) Sagittal view demonstrating prepubic space and PLN coverage; (D) Coronal view showing prepubic space and ILN interface. Other organs at risk include bladder (yellow) and rectum (brown). The patient was treated with 52 Gy to the prepubic fat and bilateral PLNs and 62.4 Gy to the bilateral ILNs over 26 fractions with concurrent weekly cisplatin. EBRT, external beam radiotherapy; ILN, lymph node; PLN, pelvic lymph node; hrHPV, high-risk HPV; PSCC, penile squamous cell carcinoma; ENE, extranodal extension; R, rectum.
|
| [1] |
Douglawi A, Masterson TA. Penile cancer epidemiology and risk factors: a contemporary review. Curr Opin Urol 2019; 29: 145e9.
|
| [2] |
Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin 2021; 71:7e33.
|
| [3] |
Montes Cardona CE, Garcia-Perdomo HA. Incidence of penile cancer worldwide: systematic review and meta-analysis. Rev Panam Salud Publica 2017; 41:e117. https://doi.org/10.26633/RPSP.2017.117.
|
| [4] |
Vieira CB, Feitoza L, Pinho J, Teixeira-Júnior A, Lages J, Calixto J, et al. Profile of patients with penile cancer in the region with the highest worldwide incidence. Sci Rep 2020; 10:2965. https://doi.org/10.1038/s41598-020-59831-5.
doi: 10.1038/s41598-020-59831-5
pmid: 32076037
|
| [5] |
Barnholtz-Sloan JS, Maldonado JL, Pow-sang J, Giuliano AR. Incidence trends in primary malignant penile cancer. Urol Oncol 2007; 25:361e7.
|
| [6] |
Hernandez BY, Barnholtz-Sloan J, German RR, Giuliano A, Goodman MT, King JB, et al. Burden of invasive squamous cell carcinoma of the penis in the United States, 1998-2003. Cancer 2008; 113:2883e91.
|
| [7] |
Djajadiningrat RS, Graafland NM, van Werkhoven E, Meinhardt W, Bex A, van der Poel HG, et al. Contemporary management of regional nodes in penile cancerdimprovement of survival. J Urol 2014; 191:68e73.
|
| [8] |
Maddineni SB, Lau MM, Sangar VK. Identifying the needs of penile cancer sufferers: a systematic review of the quality of life, psychosexual and psychosocial literature in penile cancer. BMC Urol 2009; 9:8. https://doi.org/10.1186/1471-2490-9-8.
doi: 10.1186/1471-2490-9-8
pmid: 19664235
|
| [9] |
Pagliaro LC, Crook J. Multimodality therapy in penile cancer: when and which treatments. World J Urol 2009; 27:221e5.
|
| [10] |
Martz N, Bodokh Y, Gautier M, Thamphya B, Schiappa R, Lam Cham Kee D, et al. High-dose rate brachytherapy in localized penile cancer: 5-Year clinical outcome analysis. Clin Transl Radiat Oncol 2021; 27:89e95.
|
| [11] |
Canter DJ, Nicholson S, Watkin N, Hall E, Pettaway C; InPACT Executive Committee. The international penile advanced cancer trial (InPACT): rationale and current status. Eur Urol Focus 2019; 5:706e9.
|
| [12] |
Murrell DS, Williams JL. Radiotherapy in the treatment of carcinoma of the penis. Br J Urol 1965; 37:211e22.
|
| [13] |
Alexander LL, Medina A, Benninghoff DL, Camiel MR. Cancer of the penis. Radiation therapy or surgery. J Natl Med Assoc 1972; 64:533e6.
|
| [14] |
Menon H, Patel RR, Ludmir EB, Muralidhar V, Cushman TR, Amini A, et al. Local management of preinvasive and clinical T1-3 penile cancer: utilization of diverse treatment modalities. Future Oncol 2020; 16:955e60.
|
| [15] |
Shen X, Parker W, Miller L, TenNapel M. Opportunities for use of radiation therapy in penile cancer based on patterns of care in the United States from 2007 to 2013. Ther Adv Urol 2019; 11:1756287219828972. https://doi.org/10.1177/1756287219828972.
|
| [16] |
Mulherkar R, Hasan S, Wegner RE, Verma V, Glaser SM, Kalash R, et al. National patterns of care for early-stage penile cancers in the United States: how is radiation and brachytherapy utilized. Brachytherapy 2019; 18:503e9.
|
| [17] |
Hakenberg OW, Comperat EM, Minhas S, Necchi A, Protzel C, Watkin N. EAU guidelines on penile cancer: 2014 update. Eur Urol 2015; 67:142e50.
|
| [18] |
Kamel MH, Bissada N, Warford R, Farias J, Davis R. Organ sparing surgery for penile cancer: a systematic review. J Urol 2017; 198:770e9.
|
| [19] |
Roussel E, Peeters E, Vanthoor J, Bozzini G, Muneer A, Ayres B, et al. Predictors of local recurrence and its impact on survival after glansectomy for penile cancer: time to challenge the dogma. BJU Int 2021; 127:606e13.
|
| [20] |
Neubert T, Lehmann P. Bowen’s diseaseda review of newer treatment options. Ther Clin Risk Manag 2008; 4:1085e95.
|
| [21] |
Baumgarten A, Chipollini J, Yan S, Ottenhof SR, Tang DH, Draeger D, et al. Penile sparing surgery for penile cancer: a multicenter international retrospective cohort. J Urol 2018; 199:1233e7.
|
| [22] |
McLean M, Akl AM, Warde P, Bissett R, Panzarella T, Gospodarowicz M. The results of primary radiation therapy in the management of squamous cell carcinoma of the penis. Int J Radiat Oncol Biol Phys 1993; 25:623e8.
|
| [23] |
Ozsahin M, Jichlinski P, Weber DC, Azria D, Zimmermann M, Guillou L, et al. Treatment of penile carcinoma: to cut or not to cut. Int J Radiat Oncol Biol Phys 2006; 66:674e9.
|
| [24] |
Azrif M, Logue JP, Swindell R, Cowan RA, Wylie JP, Livsey JE. External-beam radiotherapy in T1-2 N0 penile carcinoma. Clin Oncol 2006; 18:320e5.
|
| [25] |
Gotsadze D, Matveev B, Zak B, Mamaladze V. Is conservative organ-sparing treatment of penile carcinoma justified. Eur Urol 2000; 38:306e12.
|
| [26] |
Mistry T, Jones RW, Dannatt E, Prasad KK, Stockdale AD. A 10-year retrospective audit of penile cancer management in the UK. BJU Int 2007; 100:1277e81.
|
| [27] |
Zouhair A, Coucke PA, Jeanneret W, Douglas P, Do HP, Jichlinski P, et al. Radiation therapy alone or combined surgery and radiation therapy in squamous-cell carcinoma of the penis. Eur J Cancer 2001; 37:198e203.
|
| [28] |
Crook J, Ma C, Grimard L. Radiation therapy in the management of the primary penile tumor: an update. World J Urol 2009; 27:189e96.
|
| [29] |
SarinR, Norman AR, SteelGG, Horwich A. Treatment results and prognostic factors in 101 men treated for squamous carcinoma of the penis. Int J Radiat Oncol Biol Phys 1997; 38:713e22.
|
| [30] |
Korzeniowski MA, Crook JM. Contemporary role of radiotherapy in the management of penile cancer. Transl Androl Urol 2017; 6:855e67.
|
| [31] |
Soria JC, Fizazi K, Piron D, Kramar A, Gerbaulet A, Haie-Meder C, et al. Squamous cell carcinoma of the penis: multivariate analysis of prognostic factors and natural history in monocentric study with a conservative policy. Ann Oncol 1997; 8:1089e98.
|
| [32] |
Kiltie AE, Elwell C, Close HJ, Ash DV. Iridium-192 implantation for node-negative carcinoma of the penis: the Cookridge Hospital experience. Clin Oncol 2000; 12:25e31.
|
| [33] |
Mazeron JJ, Langlois D, Lobo PA, Huart JA, Calitchi E, Lusinchi A, et al. Interstitial radiation therapy for carcinoma of the penis using iridium 192 wires: the Henri Mondor experience (1970e1979). Int J Radiat Oncol Biol Phys 1984; 10:1891e5.
|
| [34] |
Crook J. Organ preserving radiation strategies for penile cancer. Urol Oncol 2022; 40:184e90.
|
| [35] |
Hasan S, Francis A, Hagenauer A, Hirsh A, Kaminsky D, Traughber B, et al. The role of brachytherapy in organ preservation for penile cancer: a meta-analysis and review of the literature. Brachytherapy 2015; 14:517e24.
|
| [36] |
Delannes M, Malavaud B, Douchez J, Bonnet J, Daly NJ. Iridium-192 interstitial therapy for squamous cell carcinoma of the penis. Int J Radiat Oncol Biol Phys 1992; 24:479e83.
|
| [37] |
Rozan R, Albuisson E, Giraud B, Donnarieix D, Delannes M, Pigneux J, et al. Interstitial brachytherapy for penile carcinoma: a multicentric survey (259 patients). Radiother Oncol 1995; 36:83e93.
|
| [38] |
Crook JM, Jezioranski J, Grimard L, Esche B, Pond G. Penile brachytherapy: results for 49 patients. Int J Radiat Oncol Biol Phys 2005; 62:460e7.
|
| [39] |
Chaudhary AJ, Ghosh S, Bhalavat RL, Kulkarni JN, Sequeira BV. Interstitial brachytherapy in carcinoma of the penis. Strahlenther Onkol 1999; 175:17e20.
|
| [40] |
Cordoba A, Escande A, Lopez S, Mortier L, Mirabel X, Coche-Déqueant B, et al. Low-dose brachytherapy for early stage penile cancer: a 20-year single-institution study (73 patients). Radiat Oncol 2016; 11:96. https://doi.org/10.1186/s13014-016-0676-9.
|
| [41] |
de Crevoisier R, Slimane K, Sanfilippo N, Bossi A, Albano M, Dumas I, et al. Long-term results of brachytherapy for carcinoma of the penis confined to the glans (Ne or NX). Int J Radiat Oncol Biol Phys 2009; 74:1150e6.
|
| [42] |
Pimenta A, Gutierrez C, Mosquera D, Pera J, Martínez E, Londres B, et al. Penile brachytherapydretrospective review of a single institution. Brachytherapy 2015; 14:525e30.
|
| [43] |
Escande A, Haie-Meder C, Mazeron R, Maroun P, Cavalcanti A, de Crevoisier R, et al. Brachytherapy for conservative treatment of invasive penile carcinoma: prognostic factors and long-term analysis of outcome. Int J Radiat Oncol Biol Phys 2017; 99:563e70.
|
| [44] |
Kellas-Sleczka S, Bialas B, Fijalkowski M, Wojcieszek P, Szlag M, Cholewka A, et al. Nineteen-year single-center experience in 76 patients with penile cancer treated with high-dose-rate brachytherapy. Brachytherapy 2019; 18: 493e502.
|
| [45] |
Rouscoff Y, Falk AT, Durand M, Gal J, Chand ME, Gautier M, et al. High-dose rate brachytherapy in localized penile cancer: short-term clinical outcome analysis. Radiat Oncol 2014; 9:142. https://doi.org/10.1186/1748-717X-9-142.
doi: 10.1186/1748-717X-9-142
pmid: 24941956
|
| [46] |
Marban M, Crook J, Keyes M, Dubash R, Batchelar D. Highdose-rate brachytherapy for localized penile cancer: evolution of a technique. Brachytherapy 2020; 19:201e9.
|
| [47] |
Sharma DN, Joshi NP, Gandhi AK, Haresh KP, Gupta S, Julka PK, et al. High-dose-rate interstitial brachytherapy for T1-T2-stage penile carcinoma: short-term results. Brachytherapy 2014; 13:481e7.
|
| [48] |
Pohankova D, Sirak I, Kasaova L, Grepl J, Paluska P, Louda M, et al. High-dose rate brachytherapy in the treatment of early stages of penile carcinoma. Klin Onkol 2019; 32:52e7.
|
| [49] |
Petera J, Sirak I, Kasaova L, Macingova Z, Paluska P, Zouhar M, et al. High-dose rate brachytherapy in the treatment of penile carcinomadfirst experience. Brachytherapy 2011; 10:136e40.
|
| [50] |
Crook JM, Haie-Meder C, DemanesDJ, Mazeron JJ, Martinez AA, Rivard MJ. American Brachytherapy Society-Groupe Européen de Curiethérapie-European Society of Therapeutic Radiation Oncology (ABS-GEC-ESTRO) consensus statement for penile brachytherapy. Brachytherapy 2013; 12:191e8.
|
| [51] |
Crook J, Jezioranski J, Cygler JE. Penile brachytherapy: technical aspects and postimplant issues. Brachytherapy 2010; 9:151e8.
|
| [52] |
Langsenlehner T, Mayer R, Quehenberger F, Prettenhofer U, Langsenlehner U, Pummer K, et al. The role of radiation therapy after incomplete resection of penile cancer. Strahlenther Onkol 2008; 184:359e63.
|
| [53] |
Ficarra V, Akduman B, Bouchot O, Palou J, Tobias-Machado M. Prognostic factors in penile cancer. Urology 2010; 76:S66e73. https://doi.org/10.1016/j.urology.2010.04.008.
|
| [54] |
Pandey D, Mahajan V, Kannan RR. Prognostic factors in nodepositive carcinoma of the penis. J Surg Oncol 2006; 93:133e8.
|
| [55] |
Leone A, Diorio GJ, Pettaway C, Master V, Spiess PE. Contemporary management of patients with penile cancer and lymph node metastasis. Nat Rev Urol 2017; 14:335e47.
|
| [56] |
Thomas A, Necchi A, Muneer A, Tobias-Machado M, Tran ATH, Van Rompuy AS, et al. Penile cancer. Nat Rev Dis Prim 2021; 7: 11. https://doi.org/10.1038/s41572-021-00246-5.
|
| [57] |
Coblentz TR, Theodorescu D. Morbidity of modified prophylactic inguinal lymphadenectomy for squamous cell carcinoma of the penis. J Urol 2002; 168:1386e9.
|
| [58] |
Clark PE, Spiess PE, Agarwal N, Biagioli MC, Eisenberger MA, Greenberg RE, et al. Penile cancer: clinical practice guidelines in oncology. J Natl Compr Canc Netw 2013; 11:594e615.
|
| [59] |
Protzel C, Alcaraz A, Horenblas S, Pizzocaro G, Zlotta A, Hakenberg OW. Lymphadenectomy in the surgical management of penile cancer. Eur Urol 2009; 55:1075e88.
|
| [60] |
Zargar-Shoshtari K, Djajadiningrat R, Sharma P, Catanzaro M, Zhu Y, Nicolai N, et al. Establishing criteria for bilateral pelvic lymph node dissection in the management of penile cancer: lessons learned from an international multicenter collaboration. J Urol 2015; 194:696e701.
|
| [61] |
Slaton JW, Morgenstern N, Levy DA, Santos MW, Tamboli P, Ro JY, et al. Tumor stage, vascular invasion and the percentage of poorly differentiated cancer: independent prognosticators for inguinal lymph node metastasis in penile squamous cancer. J Urol 2001; 165:1138e42.
|
| [62] |
Ekstrom T, Edsmyr F. Cancer of the penis; a clinical study of 229 cases. Acta Chir Scand 1958; 115:25e45.
|
| [63] |
Heyns CF, Fleshner N, Sangar V, Schlenker B, Yuvaraja TB, van Poppel H. Management of the lymph nodes in penile cancer. Urology 2010; 76:S43e57.
|
| [64] |
Network NCC. Penile cancer (version 2.2021). Available from: URL: https://www.nccn.org/professionals/physician_gls/pdf/penile.pdf.
|
| [65] |
Kulkarni JN, Kamat MR. Prophylactic bilateral groin node dissection versus prophylactic radiotherapy and surveillance in patients with N0 and N1-2A carcinoma of the penis. Eur Urol 1994; 26:123e8.
|
| [66] |
Stehman FB, Bundy BN, Thomas G, Varia M, Okagaki T, Roberts J, et al. Groin dissection versus groin radiation in carcinoma of the vulva: a Gynecologic Oncology Group study. Int J Radiat Oncol Biol Phys 1992; 24:389e96.
|
| [67] |
Koh WJ, Chiu M, Stelzer KJ, Greer BE, Mastras D, Comsia N, et al. Femoral vessel depth and the implications for groin node radiation. Int J Radiat Oncol Biol Phys 1993; 27: 969e74.
|
| [68] |
Winters BR, Kearns JT, Holt SK, Mossanen M, Lin DW, Wright JL. Is there a benefit to adjuvant radiation in stage III penile cancer after lymph node dissection? Findings from the National Cancer Database. Urol Oncol 2018; 36:e11e6. https://doi.org/10.1016/j.urolonc.2017.11.005.
|
| [69] |
Bouchot O, Auvigne J, Peuvrel P, Glemain P, Buzelin JM. Management of regional lymph nodes in carcinoma of the penis. Eur Urol 1989; 16:410e5.
|
| [70] |
el-Demiry MI, Oliver RT, Hope-Stone HF, Blandy JP. Reappraisal of the role of radiotherapy and surgery in the management of carcinoma of the penis. Br J Urol 1984; 56: 724e8.
|
| [71] |
Horenblas S. Lymphadenectomy for squamous cell carcinoma of the penis. Part 2: the role and technique of lymph node dissection. BJU Int 2001; 88:473e83.
|
| [72] |
Robinson R, Marconi L, MacPepple E, Hakenberg OW, Watkin N, Yuan Y, et al. Risks and benefits of adjuvant radiotherapy after inguinal lymphadenectomy in node-positive penile cancer: a systematic review by the European Association of Urology Penile Cancer Guidelines Panel. Eur Urol 2018; 74:76e83.
|
| [73] |
Graafland NM, Moonen LM, van Boven HH, van Werkhoven E, Kerst JM, Horenblas S. Inguinal recurrence following therapeutic lymphadenectomy for node positive penile carcinoma: outcome and implications for management. J Urol 2011; 185:888e93.
|
| [74] |
Ravi R, Chaturvedi HK, Sastry DV. Role of radiation therapy in the treatment of carcinoma of the penis. Br J Urol 1994; 74: 646e51.
|
| [75] |
Demkow T. The treatment of penile carcinoma: experience in 64 cases. Int Urol Nephrol 1999; 31:525e31.
|
| [76] |
Chen WK, Wu ZG. Adding radiotherapy based on chemotherapy can improve cancer-specific survival in N3 penile cancer: a SEER-based study. Transl Androl Urol 2020; 9: 2587e95.
|
| [77] |
Franks KN, Kancherla K, Sethugavalar B, Whelan P, Eardley I, Kiltie AE. Radiotherapy for node positive penile cancer: experience of the Leeds teaching hospitals. J Urol 2011; 186: 524e9.
|
| [78] |
Mittal R, Krishnatry R, Maitre P, Murthy V. Recommendations and clinical validation of inguinal clinical target volume delineation in penile cancer. Int J Radiat Oncol Biol Phys 2021; 111:741e53.
|
| [79] |
Milano MT, Jani AB, Farrey KJ, Rash C, Heimann R, Chmura SJ. Intensity-modulated radiation therapy (IMRT) in the treatment of anal cancer: toxicity and clinical outcome. Int J Radiat Oncol Biol Phys 2005; 63:354e61.
|
| [80] |
Sharma P, Djajadiningrat R, Zargar-Shoshtari K, Catanzaro M, Zhu Y, Nicolai N, et al. Adjuvant chemotherapy is associated with improved overall survival in pelvic node-positive penile cancer after lymph node dissection: a multi-institutional study. Urol Oncol 2015; 33:e417e23. https://doi.org/10.1016/j.urolonc.2015.05.008.
|
| [81] |
Peyraud F, Allenet C, Gross-Goupil M, Domblides C, Lefort F, Daste A, et al. Current management and future perspectives of penile cancer: an updated review. Cancer Treat Rev 2020; 90:102087. https://doi.org/10.1016/j.ctrv.2020.102087.
|
| [82] |
Bermejo C, Busby JE, Spiess PE, Heller L, Pagliaro LC, Pettaway CA. Neoadjuvant chemotherapy followed by aggressive surgical consolidation for metastatic penile squamous cell carcinoma. J Urol 2007; 177:1335e8.
|
| [83] |
Leijte JA, Kerst JM, Bais E, Antonini N, Horenblas S. Neoadjuvant chemotherapy in advanced penile carcinoma. Eur Urol 2007; 52:488e94.
|
| [84] |
Tang DH, Djajadiningrat R, Diorio G, Chipollini J, Ma Z, Schaible BJ, et al. Adjuvant pelvic radiation is associated with improved survival and decreased disease recurrence in pelvic node-positive penile cancer after lymph node dissection: a multi-institutional study. Urol Oncol 2017; 35:e617e23. https://doi.org/10.1016/j.urolonc.2017.06.001.
|
| [85] |
Johnstone PAS, Boulware D, Djajadiningrat R, Ottenhof S, Necchi A, Catanzaro M, et al. Primary penile cancer: the role of adjuvant radiation therapy in the management of extranodal extension in lymph nodes. Eur Urol Focus 2019; 5: 737e41.
|
| [86] |
Yuan Z, Grass GD, Azizi M, Ahmed KA, Yoder GSJ, Welsh EA, et al. Intrinsic radiosensitivity, genomic-based radiation dose and patterns of failure of penile cancer in response to adjuvant radiation therapy. Rep Pract Oncol Radiother 2019; 24:593e9.
|
| [87] |
Ager M, Njoku K, Serra M, Robinson A, Pickering L, Afshar M, et al. Long-term multicentre experience of adjuvant radiotherapy for pN3 squamous cell carcinoma of the penis. BJU Int 2021; 128:451e9.
|
| [88] |
Khurud P, Krishnatry R, Telkhade T, Patil A, Prakash G, Joshi A, et al. Impact of adjuvant treatment in pN3 penile cancer. Clin Oncol (R Coll Radiol) 2022; 34:172e8.
|
| [89] |
Choo R, Nehra A, Zattoni F, Pagliaro LC, Karnes RJ. Is there any benefit in adding postoperative adjuvant concurrent radiotherapy and chemotherapy for penile cancer with regional lymph node metastasis. Minerva Urol Nefrol 2020; 72:474e81.
|
| [90] |
Jaipuria J, Kohli T, Venkatasubramaniyan M, Singh A, Gupta S, Pathak P, et al. Adjuvant radiation compares favorably to chemotherapy in patients with carcinoma penis and nodal positivity restricted to groin. Urol Oncol 2020; 38: 641.e9e18. https://doi.org/10.1016/j.urolonc.2020.03.026.
|
| [91] |
Li ZS, Li XY, Wang B, Chen P, Li X, Augusto OA, et al. Radiotherapy plus chemotherapy versus chemotherapy alone in penile cancer patients with extracapsular nodal extension after inguinal lymph node surgery: a multi-institutional study. World J Urol 2021; 39:113e9.
|
| [92] |
Pond GR, Milowsky MI, Kolinsky MP, Eigl BJ, Necchi A, Harshman LC, et al. Concurrent chemoradiotherapy for men with locally advanced penile squamous cell carcinoma. Clin Genitourin Cancer 2014; 12:440e6.
|
| [93] |
De Luca F, Zacharakis E, Shabbir M, Maurizi A, Manzi E, Zanghì A, et al. Malignant priapism due to penile metastases: case series and literature review. Arch Ital Urol Andro 2016; 88:150e2.
|
| [94] |
Marcu D, Iorga L, Mischianu D, Bacalbasa N, Balescu I, Bratu O. Malignant priapismdwhat do we know about it. In Vivo 2020; 34:2225e32.
|
| [95] |
Cherian J, Rajan S, Thwaini A, Elmasry Y, Shah T, Puri R. Secondary penile tumours revisited. Int Semin Surg Oncol 2006; 3:33. https://doi.org/10.1186/1477-7800-3-33.
pmid: 17032461
|
| [96] |
Hizli F, Berkmen F. Penile metastasis from other malignancies. A study of ten cases and review of the literature. Urol Int 2006; 76:118e21.
|
| [97] |
Davidson T, Domachevsky L, Giladi Y, et al. Penile secondary lesions: a rare entity detected by PET/CT. Sci Rep 2021; 11: 5912. https://doi.org/10.1038/s41598-021-85300-8.
doi: 10.1038/s41598-021-85300-8
pmid: 33723317
|
| [98] |
Spinapolice EG, Fuccio C, Rubino B, Palumbo R, Mensi M, Scopesi L, et al. Penile metastases from bladder and prostate cancer detected by PET/CT:a report of 3 cases and a review of literature. Clin Genitourin Cancer 2014; 12:e155e9. https://doi.org/10.1016/j.clgc.2014.03.013.
|
| [99] |
Parida GK, Tripathy S, Roy SG, Singhal A, Das C, Shamim SA. Incidentally detected penile metastases in a patient of carcinoma urinary bladder on follow-up FDG PET/CT. Clin Nucl Med 2017; 42:e273e4. https://doi.org/10.1097/RLU.0000000000001607.
|
| [100] |
Xing DT, Yilmaz H, Hettige S, Hegde R, Nair R. Successful treatment of malignant priapism by radiotherapy: report of a case, review of the literature, and treatment recommendations. Cureus 2021; 13:e17287. https://doi.org/10.7759/cureus.17287.
|
| [101] |
Ben-Yosef R, Kapp DS. Cancer metastatic to the penis: treatment with hyperthermia and radiation therapy and review of the literature. J Urol 1992; 148:67e71.
|
| [102] |
Gomez-Iturriaga A, Crook J, Evans W, Saibishkumar EP, Jezioranski J. The efficacy of hyperbaric oxygen therapy in the treatment of medically refractory soft tissue necrosis after penile brachytherapy. Brachytherapy 2011; 10:491e7.
|
| [103] |
Stroie FA, Houlihan MD, Kohler TS. Sexual function in the penile cancer survivor: a narrative review. Transl Androl Urol 2021; 10:2544e53.
|
| [104] |
Delaunay B, Soh PN, Delannes M, Riou O, Malavaud B, Moreno F, et al. Brachytherapy for penile cancer: efficacy and impact on sexual function. Brachytherapy 2014; 13:380e7.
|
| [105] |
Gambachidze D, Lebacle C, Maroun P, Escande A, Bossi A, Blanchard P, et al. Long-term evaluation of urinary, sexual, and quality of life outcomes after brachytherapy for penile carcinoma. Brachytherapy 2018; 17:221e6.
|
| [106] |
de Vries HM, Chipollini J, Slongo J, Boyd F, Korkes F, Albersen M, et al. Outcomes of perineal urethrostomy for penile cancer: a 20-year international multicenter experience. Urol Oncol 2021; 39:500.e9e13. https://doi.org/10.1016/j.urolonc.2021.04.023.
|
| [107] |
Johnstone PA. Impact of radiation therapy on perineal urethrostomy for penile cancer. Clinical and Translational Radiation Oncology 2021; 30:80e7.
|
| [108] |
Chen MF, Chen WC, Wu CT, Chuang CK, Ng KF, Chang JT. Contemporary management of penile cancer including surgery and adjuvant radiotherapy: an experience in Taiwan. World J Urol 2004; 22:60e6.
|
| [109] |
Ravi R. Radiation-induced carcinoma of the penis. Urol Int 1995; 54:147e9.
|
| [110] |
Wells AD, Pryor JP. Radiation-induced carcinoma of the penis. Br J Urol 1986; 58:325e6.
|
| [111] |
Heideman DA, Waterboer T, Pawlita M, Delis-van Diemen P, Nindl I, Leijte JA, et al. Human papillomavirus-16 is the predominant type etiologically involved in penile squamous cell carcinoma. J Clin Oncol 2007; 25:4550e6.
|
| [112] |
Olesen TB, Sand FL, Rasmussen CL, Albieri V, Toft BG, Norrild B, et al. Prevalence of human papillomavirus DNA and p16INK4a in penile cancer and penile intraepithelial neoplasia: a systematic review and meta-analysis. Lancet Oncol 2019; 20:145e8.
|
| [113] |
Kidd LC, Chaing S, Chipollini J, Giuliano AR, Spiess PE, Sharma P. Relationship between human papillomavirus and penile cancerdimplications for prevention and treatment. Transl Androl Urol 2017; 6:791e802.
|
| [114] |
Bezerra AL, Lopes A, Santiago GH, Ribeiro KC, Latorre MR, Villa LL. Human papillomavirus as a prognostic factor in carcinoma of the penis: analysis of 82 patients treated with amputation and bilateral lymphadenectomy. Cancer 2001; 91:2315e21.
|
| [115] |
Wiener JS, Effert PJ, Humphrey PA, Yu L, Liu ET, Walther PJ. Prevalence of human papillomavirus types 16 and 18 in squamous-cell carcinoma of the penis: a retrospective analysis of primary and metastatic lesions by differential polymerase chain reaction. Int J Cancer 1992; 50:694e701.
|
| [116] |
Lont AP, Kroon BK, Horenblas S, Gallee MP, Berkhof J, Meijer CJ, et al. Presence of high-risk human papillomavirus DNA in penile carcinoma predicts favorable outcome in survival. Int J Cancer 2006; 119:1078e81.
|
| [117] |
Djajadiningrat RS, Jordanova ES, Kroon BK, van Werkhoven E, de Jong J, Pronk DT, et al. Human papillomavirus prevalence in invasive penile cancer and association with clinical outcome. J Urol 2015; 193:526e31.
|
| [118] |
Sand FL, Rasmussen CL, Frederiksen MH, Andersen KK, Kjaer SK. Prognostic significance of HPV and p16 status in men diagnosed with penile cancer: a systematic review and meta-analysis. Cancer Epidemiol Biomarkers Prev 2018; 27: 1123e32.
|
| [119] |
Yuan Z, Naghavi AO, Tang D, Ahmed KA, Dhillon J, Giuliano AR, et al. The relationship between HPV status and chemoradiotherapy in the locoregional control of penile cancer. World J Urol 2018; 36:1431e40.
|
| [120] |
Bandini M, Ross JS, Zhu Y, Ye DW, Ornellas AA, Watkin N, et al. Association between human papillomavirus infection and outcome of perioperative nodal radiotherapy for penile carcinoma. Eur Urol Oncol 2021; 4:802e10.
|
| [121] |
Scott JG, Berglund A, Schell MJ, Mihaylov I, Fulp WJ, Yue B, et al. A genome-based model for adjusting radiotherapy dose (GARD): a retrospective, cohort-based study. Lancet Oncol 2017; 18:202e11.
|
| [122] |
Eschrich S, Zhang H, Zhao H, Boulware D, Lee JH, Bloom G, et al. Systems biology modeling of the radiation sensitivity network: a biomarker discovery platform. Int J Radiat Oncol Biol Phys 2009; 75:497e505.
|
| [123] |
Yuan Z, Yang GQ, Ahmed KA, Torres-Roca JF, Spiess PE, Johnstone PA. Radiation therapy in the management of the inguinal region in penile cancer: what’s the evidence. Urol Oncol 2020; 40:223e8.
|
| [124] |
Aydin AM, Chahoud J, Adashek JJ, Azizi M, Magliocco A, Ross JS, et al. Understanding genomics and the immune environment of penile cancer to improve therapy. Nat Rev Urol 2020; 17:555e70.
|
| [125] |
Cosper PF, Bradley S, Luo L, Kimple RJ. Biology of HPV mediated carcinogenesis and tumor progression. Semin Radiat Oncol 2021; 31:265e73.
|
| [126] |
Stewart-Ornstein J, Iwamoto Y, Miller MA, Jambhekar A, Forrester WC, Weissleder R, et al. p53 dynamics vary between tissues and are linked with radiation sensitivity. Nat Commun 2021; 12:898. https://doi.org/10.1038/s41467-021-21145-z.
doi: 10.1038/s41467-021-21145-z
pmid: 33563973
|
| [127] |
Fenner A. HPV positivity and radiotherapy outcomes in PSCC. Nat Rev Urol 2021; 18:4. https://doi.org/10.1038/s41585-020-00411-7.
doi: 10.1038/s41585-020-00411-7
pmid: 33244177
|
| [1] |
Alcides Chaux,Diego F. Sanchez,María José Fernández-Nestosa,Sofía Cañete-Portillo,Ingrid M. Rodríguez,Giovanna A. Giannico,Antonio L. Cubilla. The dual pathogenesis of penile neoplasia: The heterogeneous morphology of human papillomavirus-related tumors[J]. Asian Journal of Urology, 2022, 9(4): 349-358. |
| [2] |
Karl H. Pang,Hussain M. Alnajjar,Asif Muneer. Advances in penile-sparing surgical approaches[J]. Asian Journal of Urology, 2022, 9(4): 359-373. |
| [3] |
Vidhu B. Joshi,Juskaran Chadha,Jad Chahoud. Penile cancer: Updates in systemic therapy[J]. Asian Journal of Urology, 2022, 9(4): 374-388. |
| [4] |
Chinna Babu Dracham,Narendra Kumar,Santosh Kumar,Arun Elangovan,Budhi Singh Yadav,Ravimohan S. Mavuduru,Anupam Lal,Pramod K. Gupta,Rakesh Kapoor. A phase II study of neoadjuvant chemotherapy followed by organ preservation in patients with muscle-invasive bladder cancer[J]. Asian Journal of Urology, 2022, 9(3): 318-328. |
| [5] |
Mengzhu Liu,Kun Jin,Shi Qiu,Pengyong Xu,Mingming Zhang,Wufeng Cai,Xiaonan Zheng,Lu Yang,Qiang Wei. Oncological outcomes of patients with ductal adenocarcinoma of the prostate receiving radical prostatectomy or radiotherapy[J]. Asian Journal of Urology, 2021, 8(2): 227-234. |
| [6] |
Bohdan Baralo,Patrick Samson,David Hoenig,Arthur Smith. Percutaneous kidney stone surgery and radiation exposure: A review[J]. Asian Journal of Urology, 2020, 7(1): 10-17. |
| [7] |
Michel Bolla,Ann Henry,Malcom Mason,Thomas Wiegel. The role of radiotherapy in localised and locally advanced prostate cancer[J]. Asian Journal of Urology, 2019, 6(2): 153-161. |
| [8] |
Rei Umezawa,Koji Inaba,Satoshi Nakamura,Akihisa Wakita,Hiroyuki Okamoto,Keisuke Tsuchida,Tairo Kashihara,Kazuma Kobayashi,Ken Harada,Kana Takahashi,Naoya Murakami,Yoshinori Ito,Hiroshi Igaki,Keiichi Jingu,Jun Itami. Dose escalation of external beam radiotherapy for high-risk prostate cancer—Impact of multiple high-risk factor[J]. Asian Journal of Urology, 2019, 6(2): 192-199. |
| [9] |
Shulian Chen,Rang Gao,Hong Li,Kunjie Wang. Management of acquired rectourethral fistulas in adults[J]. Asian Journal of Urology, 2018, 5(3): 149-154. |
| [10] |
Yoshiyasu Amiya, Yasutaka Yamada, Masahiro Sugiura, Makoto Sasaki, Takayuki Shima, Noriyuki Suzuki, Hiroomi Nakatsu, Shino Murakami, Jun Shimazaki. Outcomes of patients older than 75 years with non-metastatic prostate cancer[J]. Asian Journal of Urology, 2017, 4(2): 102-106. |
| [11] |
Yu Guang Tan, Weber Lau Kam On, Hong Hong Huang, Terence Tan Wee Kiat. Prostate specific antigen bounce after intensity-modulated radiation therapy in an Asian population[J]. Asian Journal of Urology, 2016, 3(2): 59-63. |
| [12] |
Cheng Yang, Mushuang Hu, Tongyu Zhu, Wanyuan He. Evaluation of kidney allograft status using novel ultrasonic technologies[J]. Asian Journal of Urology, 2015, 2(3): 142-150. |
|
|
|
|