|
|
|
| Subadventitial resection of the ureter—new method for surgical corrections of the ureteropelvic junction and ureterovesical junction obstructions |
Akif Memmedoglu Bağirov( ) )
|
| Department of Urology, Azerbaijan Medical University, Azerbaijan, Baku, Azerbaijan |
|
|
|
|
Abstract Objective: The aim of our study was to examine results of pyeloplasty using the new method—subadventitial resection of the ureter with preservation of the ureteral artery proposed by us and the possibility of using this method in one-stage surgery with ureteropelvic junction (UPJ) and ureterovesical junction (UVJ) obstructions or vesicoureteral reflux.
Methods: A retrospective analysis of 108 patients with hydronephrosis (including two patients with hydroureteronephrosis) who received treatment from March 1998 to March 2020 was carried out, with an average follow-up period of 36 months. Dismembered pyeloplasty using a subadventitial technique with preservation of ureteral blood supply was performed in 108 patients (including bilateral in two cases). In one patient with UPJ and UVJ obstructions and in one patient with UPJ obstruction and vesicoureteral reflux subadventitial resection of the ureter were performed in both segments.
Results: All patients managed to preserve the integrity of the ureteral artery during dismembered pyeloplasty, and two patients simultaneously underwent ureterocystostomy by subadventitial resection of the ureter. The method of pyeloureteroplasty with subadventitial resection of the ureter makes it possible to improve long-term results in patients with hydronephrosis, including those with lesions of the UPJ and UVJ segments. In all cases, it was feasible to achieve a decrease in the degree of hydronephrosis. Postoperative complications were observed in five cases (4.6%), in none of which there were complications associated with the surgical technique, and were eliminated without loss of renal function.
Conclusion: Our 22 years of experience shows that the technique of subadventitial resection of the ureter allows us to preserve the ureteral blood circulation during dismembered pyeloplasty and thus creates conditions for prevention of restenosis of UPJ and for single-stage ureteroplasty on the upper and lower ureteral segments.
|
|
Received: 17 January 2021
Available online: 20 April 2023
|
| About author:: E-mail address: dr.akif.bagirov@gmail.com. |
|
|
|
|
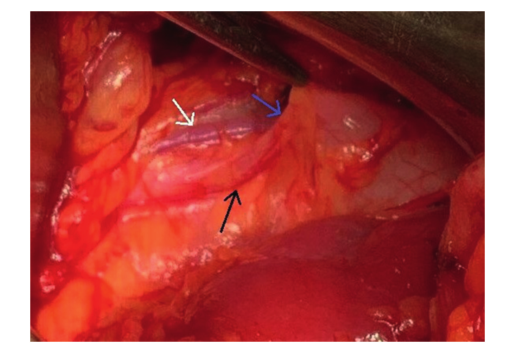
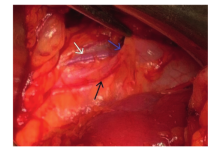
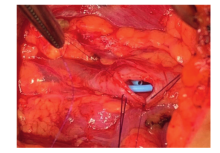
Ureteropelvic junction area in open dismembered ureteropyeloplasty. White arrow shows testicular vein; blue arrow shows ureter; black arrow shows ureteral artery.
|
|
|
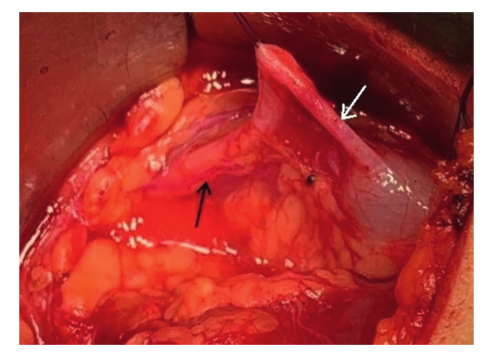
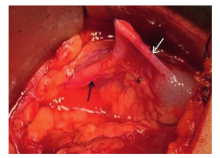
Incision and dissection adventitious layer of the ureter. White arrow shows ureter; black arrow shows ureteral artery.
|
|
|
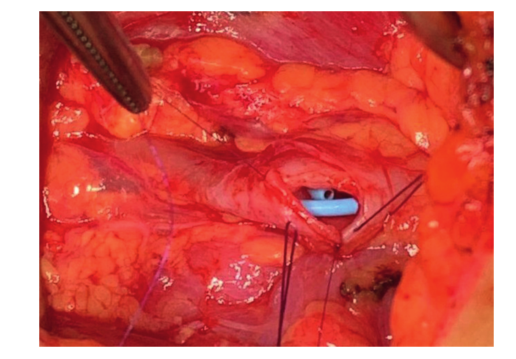
An anastomosis of the posterior wall between the ureter and the renal pelvis.
|
|
|
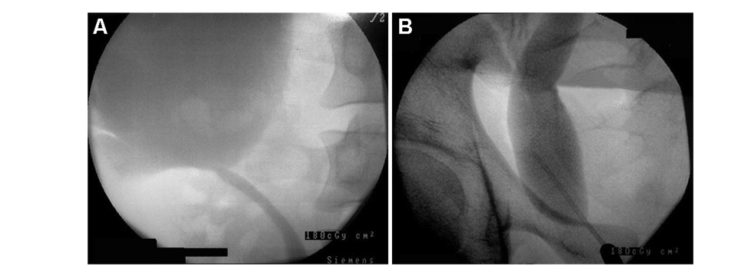
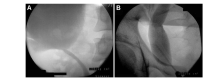
Retrograde ureteropyelography. (A) Stenosis of the right ureteropelvic junction and Grade III hydronephrosis; (B) Stenosis of right ureterovesical junction and megaureter.
|
|
|
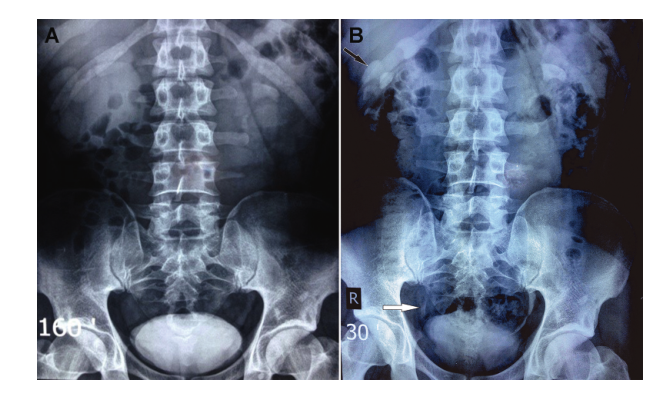
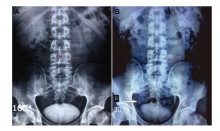
Preoperative and postoperative excretory urography. (A) Preoperative excretory urography. At 160 min on the left, the function was normal; on the right, only the contours of the kidney were determined. (B) Postoperative excretory urography (1 month after surgery). At 30 min, the functional ability of the right kidney improved; hydronephrosis decreased to Grade II (black arrow). The distal ureter was contrasted and the diameter was normal (white arrow).
|
|
|
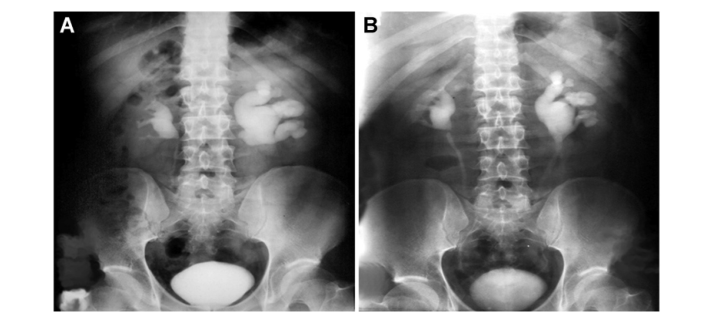
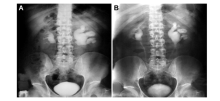
Preoperative and postoperative excretory urography of a patient using ureteropyeloplasty with subadventitial resection of the ureter. (A) Preoperative excretory urography. At 120 min, left-sided Grade III hydronephrosis and right-sided pyelectasis (Grade I hydronephrosis) were detected. (B) Postoperative excretory urography (after 1 month of surgery). At 30 min, it was determined that the ureteropelvic junction had normal patency and a decrease in hydronephrosis to Grade II.
|

| Complications and surgical variables | Tan et al., 2011 [9] (laparoscopic pyeloplasty, n=102) | Blanc et al., 2013 [10] (retroperitoneoscopic laparoscopic pyeloplasty, n=104) | Salih, 2015 [11] (laparoscopic pyeloplasty, n=14; open pyeloplasty, n=69) | Our study (open subadventitial pyeloplasty, n=110) | | Any complication, n | 32a | 13 | 10 | 5 | | Restenosis | 18 | 2 | 5 | 1 | | Parenchimal injury | NR | 2 | NR | 0 | | Stent complication | 5 | 2 | 1 | 1 | | Urine leak | 18 | 3 | 1 | 1 | | Urinar tract infection | NR | NR | NR | 2 (bacteriuria-1, urosepsis-1) | | Other | NR | 4 | 3 | 0 | | Surgical variable, n | | Conversion | 2 | 3 | NR | NR | | Reoperation | 16 (endopyelotomy?10;nephrectomy-6) | 2 | 5 (replasty-1; endopyelotomy-4) | 2 (replasty-1; ureteral stent extraction-1) |
|
|
Laparoscopic and open pyeloplasty complications and surgical variables (our results in comparison with literature data).
|
| [1] |
Siddiqui MM, McDougal WS. Urologic assessment of decreasing renal function. Med Clin 2011; 95:161-8.
|
| [2] |
McGrath MA, Estrof J, Lebowitz RL. The coexistence of obstruction at the ureteropelvic and ureterovesical junctions. AJR Am J Roentgenol 1987; 149:403-6.
doi: 10.2214/ajr.149.2.403
|
| [3] |
Pitts WA, Muecke EL. Congenital megaloureter: a review of 80 patients. J Urol 1974; 111:468-73.
doi: 10.1016/s0022-5347(17)59993-0
pmid: 4819373
|
| [4] |
Pastorea V, Acetob G, Niglioa F, Basile A, Cocomazzi R, Faticato MG, et al. Clinical characteristics and management of children with ureteropelvic junction obstruction and severe vesicoureteral reflux: preliminary results. AOPS 2013; 9: 114-6.
|
| [5] |
Klingler HC, Remzi M, Janetschek G, Kratzik C, Marberger MJ. Comparison of open versus laparoscopic pyeloplasty techniques in treatment of uretero-pelvic junction obstruction. Eur Urol 2003; 44:340-5.
doi: 10.1016/s0302-2838(03)00297-5
pmid: 12932933
|
| [6] |
Carr MC, El-Ghoneimi A. Anomalies and surgery of ureteropelvic junction in children. In: Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Campbell-walsh Urology. 9 th ed. Philadelphia: W. B. Saunders; 2007. p8477-532.
|
| [7] |
Lee YS, Im YJ, Lee H, Kim MJ, Lee MJ, Jung HJ, et al. Coexisting ureteropelvic junction obstruction and ureterovesical junction obstruction: is pyeloplasty always the preferred initial surgery? Urology 2014; 83:443-9.
doi: 10.1016/j.urology.2013.08.087
pmid: 24246322
|
| [8] |
Kogan BA. Disorders of the ureter and ureteropelvic junction. In: Tanagho FA, McAninch JW, editors. Smith’s general urology. 17th ed. New York: McGraw-Hill Medical; 2012.p559-73.
|
| [9] |
Tan HJ, Ye Z, Roberts WW, Wolf JS. Failure after laparoscopic pyeloplasty: prevention and management. J Endourol 2011; 25:1457-62.
doi: 10.1089/end.2010.0647
|
| [10] |
Blanc T, Muller C, Abdoul H, Peev S, Paye-Jaouen, Peycelon M, et al. Retroperitoneal laparoscopic pyeloplasty in children: long-term outcome and critical analysis of 10-year experience in a teaching center. Eur Urol 2013; 63:565-72.
doi: 10.1016/j.eururo.2012.07.051
pmid: 22902039
|
| [11] |
Salih EM. Morphological and functional outcome of dismembered pyeloplasty in children with unilateral ureteropelvic junction obstruction. Afr J Urol 2015; 21:174-80.
doi: 10.1016/j.afju.2015.04.003
|
| [12] |
O’Reilly PH, Brooman PJ, Mak S, Jones M, Pickup C, Atkinson C, et al. The long-term results of Anderson-Hynes pyeloplasty. BJU Int 2001; 87:287-9.
doi: 10.1046/j.1464-410x.2001.00108.x
pmid: 11251517
|
| [13] |
Maheshwari R, Ansari MS, Mandhani A, Srivastava A, Kapoor R. Laparoscopic pyeloplasty in pediatric patients: the SGPGI experience. Indian J Urol 2010; 26:36-40.
doi: 10.4103/0970-1591.60441
|
| [1] |
Yiwei Wang, Liheng Gao, Mingxi Xu, Wenfeng Li, Yuanshen Mao, Fujun Wang, Lu Wang, Jun Da, Zhong Wang. A novel spherical-headed fascial dilator is feasible for second-stage ultrasound guided percutaneous nephrolithotomy: A pilot study[J]. Asian Journal of Urology, 2021, 8(4): 424-429. |
| [2] |
Farzaneh Sharifiaghdas,Mahboubeh Mirzaei,Azar Daneshpajooh,Shahin Abbaszadeh. Minimally invasive open dismembered pyeloplasty technique: Miniature incision, muscle-splitting dissection, and nopelvis reduction in children[J]. Asian Journal of Urology, 2019, 6(3): 290-293. |
| [3] |
Kristina Pavlovic, Dirk Lange, Ben H. Chew. Stents for malignant ureteral obstruction[J]. Asian Journal of Urology, 2016, 3(3): 142-149. |
| [4] |
Pradeep Kajal, Kamal Rattan, Vijender Sangwan, Namita Bhutani. Retrocaval ureter presenting at 6 years of age in a girl child——An extreme rarity[J]. Asian Journal of Urology, 2016, 3(2): 107-109. |
|
|
|
|