|
|
|
| Treatment trends of muscle invasive bladder cancer: Evidence from the Surveillance, Epidemiology, and End Results database, 1988 to 2013 |
Victor Chalfanta,*( ),Michael L. BluteJr.a,Peter Silbersteinb ),Michael L. BluteJr.a,Peter Silbersteinb
|
a Urology at CHI Health Creighton University Medical Center Omaha, NE, USA
b Hematology Oncology at CHI Health Creighton University Medical Center Omaha, NE, USA |
|
|
|
|
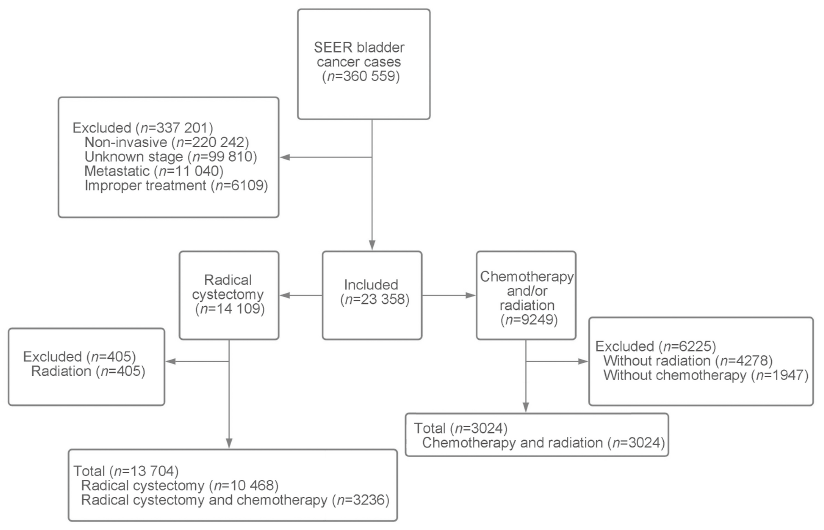
Abstract Objective: Guidelines for muscle-invasive bladder cancer (MIBC) recommend that patients receive neoadjuvant chemotherapy with radical cystectomy as treatment over radical cystectomy alone. Though trends and practice patterns of MIBC have been defined using the National Cancer Database, data using the Surveillance, Epidemiology, and End Results (SEER) program have been poorly described. Methods: Using the SEER database, we collected data of MIBC according to the American Joint Commission on Cancer. We considered differences in patient demographics and tumor characteristics based on three treatment groups: chemotherapy (both adjuvant and neoadjuvant) with radical cystectomy, radical cystectomy, and chemoradiotherapy. Multinomial logistic regression was performed to compare likelihood ratios. Temporal trends were included for each treatment group. Kaplan-Meier curves were performed to compare cause-specific survival. A Cox proportional-hazards model was utilized to describe predictors of survival. Results: Of 16 728 patients, 10 468 patients received radical cystectomy alone, 3236 received chemotherapy with radical cystectomy, and 3024 received chemoradiotherapy. Patients who received chemoradiotherapy over radical cystectomy were older and more likely to be African American; stage III patients tended to be divorced. Patients who received chemotherapy with radical cystectomy tended to be males; stage II patients were less likely to be Asian than Caucasian. Stage III patients were less likely to receive chemoradiotherapy as a treatment option than stage II. Chemotherapy with radical cystectomy and chemoradiotherapy are both underutilized treatment options, though increasingly utilized. Kaplan-Meier survival curves showed significant differences between stage II and III tumors at each interval. A Cox proportional-hazards model showed differences in gender, tumor stage, treatment modality, age, and marital status. Conclusion: Radical cystectomy alone is still the most commonly used treatment for muscle-invasive bladder cancer based on temporal trends. Significant disparities exist in those who receive radical cystectomy over chemoradiotherapy for treatment.
|
|
Received: 06 September 2020
Available online: 20 January 2023
|
|
Corresponding Authors:
Victor Chalfant
E-mail: victorchalfant@creighton.edu
|
|
|
|
|
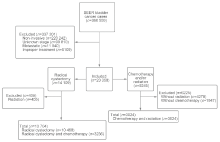
Case flow diagram. SEER, the Surveillance, Epidemiology, and End Results.
|

| Patient demographic | Treatment (n=9243) | p-Valuea | | Radical cystectomy; n=5185 (56.1%) | Radical cystectomy + chemotherapy; n=1615 (17.5%) | Chemotherapy + radiation; n=2443 (26.4%) | | Age at diagnosis | | | | <0.001 | | Population age, mean, year | 66.2 | 63.8 | 72.1 | | | 85+ years old, n (%) | 165 (3.2) | 15 (0.9) | 384 (15.7) | | | Sex, n (%) | | | | <0.001 | | Male | 3918 (75.6) | 1264 (78.3) | 1785 (73.1) | | | Female | 1267 (24.4) | 351 (21.7) | 658 (26.9) | | | Race, n (%) | | | | <0.001 | | Caucasian | 4663 (89.9) | 1482 (91.8) | 2179 (89.2) | | | Asian or Pacific Islander | 221 (4.3) | 48 (3.0) | 82 (3.4) | | | African American | 275 (5.3) | 74 (4.6) | 170 (7.0) | | | Unknown | 26 (0.5) | 11 (0.7) | 2 (0.5) | | | Marital status, n (%) | | | | <0.001 | | Married | 3382 (65.2) | 1108 (68.6) | 1383 (56.6) | | | Widowed | 613 (11.8) | 122 (7.6) | 532 (21.8) | | | Divorced | 460 (8.9) | 147 (9.1) | 211 (8.6) | | | Single | 510 (9.8) | 163 (10.1) | 209 (8.6) | | | Unknown | 220 (4.2) | 75 (4.6) | 108 (4.4) | | | Primary site, n (%) | | | | <0.05 | | Trigone of bladder | 329 (6.3) | 89 (5.5) | 177 (7.2) | | | Dome of bladder | 194 (3.7) | 63 (3.9) | 124 (5.1) | | | Bladder wall | 1607 (31.0) | 505 (31.3) | 847 (34.7) | | | Overlapping lesion of bladder | 881 (17.0) | 278 (17.2) | 375 (15.4) | | | Unknown | 2174 (41.9) | 680 (42.1) | 920 (37.7) | | | Grade, n (%) | | | | <0.001 | | Moderately differentiated | 387 (7.5) | 51 (3.2) | 94 (3.8) | | | Poorly differentiated or undifferentiated | 4553 (87.8) | 1450 (89.8) | 2187 (89.5) | | | Unknown | 245 (4.7) | 114 (7.1) | 162 (6.6) | |
|
|
Patient demographics and tumor characteristics based on treatment groups for stage II.
|
| Patient demographic | Treatment (n=7485) | p-Valuea | | Radical cystectomy; n=5283 (70.6%) | Radical cystectomy + chemotherapy; n=1621 (21.7%) | Chemotherapy + radiation; n=581 (7.8%) | | Age at diagnosis | | | | <0.001 | | Population age, mean, year | 68.9 | 65.5 | 71.9 | | | 85+ years old, n (%) | 229 (4.3) | 20 (1.2) | 78 (13.4) | | | Sex, n (%) | | | | <0.001 | | Male | 3707 (70.2) | 1216 (75.0) | 438 (75.4) | | | Female | 1576 (29.8) | 405 (25.0) | 143 (24.6) | | | Race, n (%) | | | | <0.05 | | Caucasian | 4728 (89.5) | 1462 (90.2) | 499 (85.9) | | | Asian or Pacific Islander | 214 (4.1) | 66 (4.1) | 27 (4.6) | | | African American | 317 (6.0) | 84 (5.2) | 53 (9.1) | | | Unknown | 24 (0.5) | 9 (0.6) | 2 (0.3) | | | Marital status, n (%) | | | | <0.001 | | Married | 3275 (62.0) | 1104 (68.1) | 325 (55.9) | | | Widowed | 870 (16.5) | 146 (9.0) | 122 (21.0) | | | Divorced | 471 (8.9) | 134 (8.3) | 64 (11.0) | | | Single | 487 (9.2) | 174 (10.7) | 49 (8.4) | | | Unknown | 180 (3.4) | 63 (3.9) | 21 (3.6) | | | Primary site, n (%) | | | | NS | | Trigone of bladder | 317 (6.0) | 263 (16.2) | 42 (7.2) | | | Dome of bladder | 263 (5.0) | 67 (4.1) | 16 (2.8) | | | Bladder wall | 1509 (28.6) | 459 (28.3) | 147 (25.3) | | | Overlapping lesion of bladder | 1146 (21.7) | 343 (21.2) | 111 (19.1) | | | Unknown | 2048 (38.8) | 489 (30.2) | 265 (45.6) | | | Grade, n (%) | | | | <0.001 | | Moderately differentiated | 418 (7.9) | 80 (4.9) | 30 (5.2) | | | Poorly differentiated or undifferentiated | 4700 (89.0) | 1479 (91.2) | 510 (87.8) | | | Unknown | 165 (3.1) | 62 (3.8) | 41 (7.1) | |
|
|
Patient demographics and tumor characteristics based on treatment groups for stage III.
|
| Stages | Treatment | Total | | Radical cystectomy | Radical cystectomy + chemotherapy | Chemotherapy + radiation | | II | 5185 (56.1) | 1615 (17.5) | 2443 (26.4) | 9243 | | III | 5283 (70.6) | 1621 (21.7) | 581 (7.8) | 7485 | | p-Valuea | NS | NS | <0.001 | |
|
|
Treatment groups were separated into stage II and III.
|
| Patient demographic | Likelihood ratio (95% CI) of stage II patients | Likelihood ratio (95% CI) of stage III patients | | Radical cystectomy + chemotherapy | Chemotherapy + radiation | p-Value | Radical cystectomy + chemotherapy | Chemotherapy + radiation | p-Value | | Sex | | | <0.001 | | | <0.001 | | Male | Reference | Reference | | Reference | Reference | | | Female | 0.9 (0.8-1.0) | 1.1 (1.0-1.2) | | 0.8 (0.7-0.9) | 0.8 (0.6-0.9) | | | Age, year | | | <0.001 | | | <0.001 | | 55-65 | Reference | Reference | | Reference | Reference | | | 65-75 | 1.1 (0.9-1.2) | 2.0 (1.6-2.4) | | 0.7 (0.6-0.9) | 1.1 (0.8-1.4) | | | 75-85 | 2.3 (1.9-2.7) | 8.7 (7.0-10.7) | | 0.4 (0.4-0.5) | 2.0 (1.5-2.6) | | | 85+ | Reference | Reference | | 1.0 (0.5-1.9) | 0.1 (0.1-0.2) | | | Race | | | <0.001 | | | <0.05 | | Caucasian | Reference | Reference | | Reference | Reference | | | Asian | 0.7 (0.5-0.9) | 0.8 (0.6-1.0) | | 1.0 (0.8-1.3) | 1.2 (0.8-1.8) | | | African American | 0.8 (0.7-1.1) | 1.3 (1.1-1.6) | | 0.9 (0.7-1.1) | 1.6 (1.2-2.2) | | | Marital status | | | <0.001 | | | <0.001 | | Married | Reference | Reference | | Reference | Reference | | | Divorced | 0.9 (0.7-1.2) | 1 (0.7-1.4) | | 0.84 (0.7-1.0) | 1.4 (1.0-1.8) | | | Grade | | | <0.001 | | | <0.001 | | Moderately differentiated | Reference | Reference | | Reference | Reference | | | Poorly or undifferentiated | 2.4 (1.8-3.3) | 2 (1.6-2.5) | | 1.6 (1.2-2.0) | 1.7 (1.1-2.6) | |
|
|
Cox proportional hazards model indicating likelihood of group receiving either chemotherapy with radical cystectomy or chemotherapy plus radiation compared to reference radical cystectomy group.
|
|
|
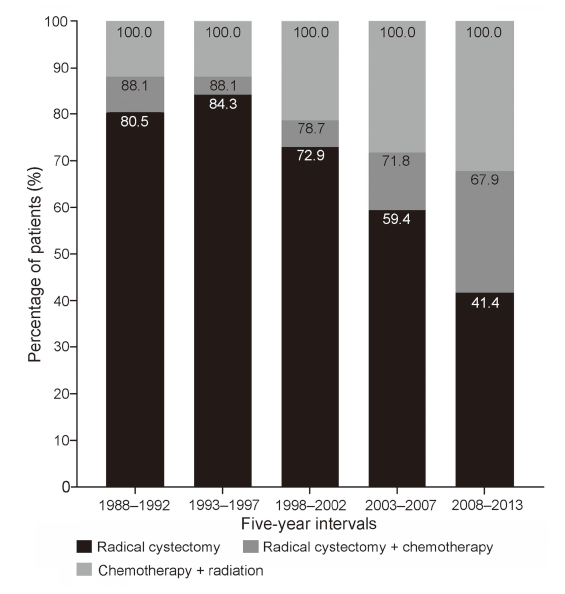
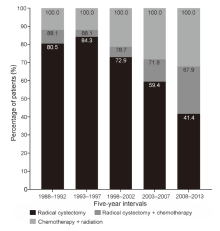
Percentage of patients by treatment group treated for stage II MIBC from 1988 to 2013 based on 5-year intervals. For 1988-1992, n=399; 1993-1997, n=597; 1998-2002, n=1186; 2003-2007, n=2848; 2008-2013, n=4213 (highly significant of p-values of <0.001).
|
|
|
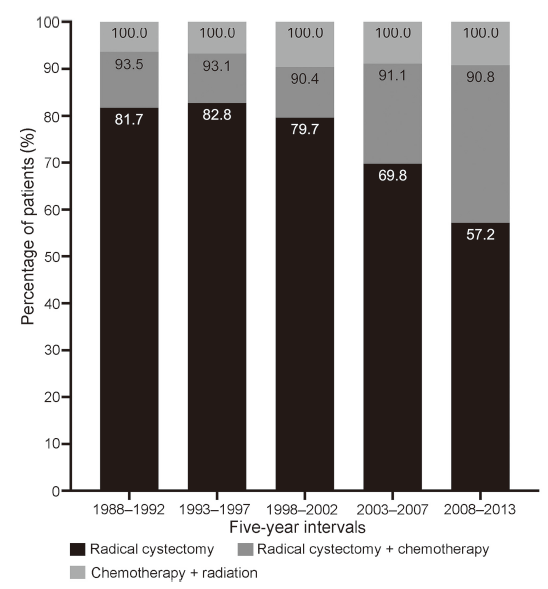
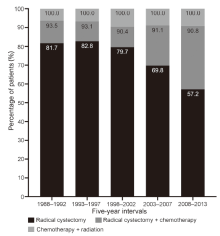
Percentage of patients by treatment treated for stage III MIBC from 1988 to 2013 based on 5-year intervals. For 1988-1992, n=478; 1993-1997, n=743; 1998-2002, n=1666; 2003-2007, n=2060; 2008-2013, n=2538 (highly significant of p-values of <0.001).
|

|
|
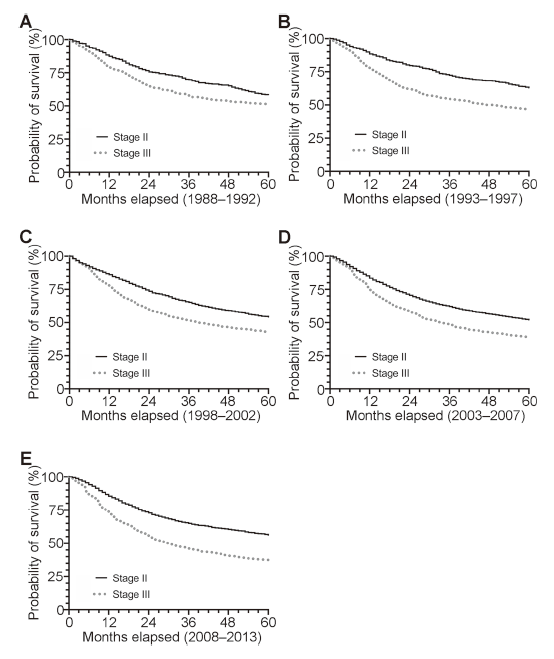
5-year cause-specific survival curves of muscle-invasive bladder cancer for stage II versus stage III from 1988 to 2013 at 5-year intervals. Cases from (A) 1988-1992, n=877; (B) 1993-1997, n=1340; (C) 1998-2002, n=2852; (D) 2003-2007, n=4908; (E) 2008-2013, n=6751 (p-values <0.05).
|
| [1] |
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin 2019; 69:7e34.
|
| [2] |
Pasin E, Josephson DY, Mitra AP, Cote RJ, Stein JP. Super?cial bladder cancer: an update on etiology, molecular develop-ment, classi?cation, and natural history. Rev Urol 2008; 10: 31e43.
pmid: 18470273
|
| [3] |
Anastasiadis A, de Reijke TM. Best practice in the treatment of nonmuscle invasive bladder cancer. Ther Adv Urol 2012; 4: 13e32.
doi: 10.1177/1756287211431976
|
| [4] |
Burger M, Catto JW, Dalbagni G, Grossman HB, Herr H, Karakiewicz P, et al. Epidemiology and risk factors of uro-thelial bladder cancer. Eur Urol 2013; 63:234e41.
doi: 10.1016/j.eururo.2012.07.033
|
| [5] |
Flaig TW, Spiess PE, Agarwal N, Bangs R, Boorjian SA, Buyyounouski MK, et al. Bladder cancer, version 3.2020, NCCN clinical practice guidelines in Oncology. J Natl Compr Cancer Netw 2020; 18:329e54.
|
| [6] |
International collaboration of trialists on behalf of the Medical Research Council Advanced Bladder Cancer Working Party, EORTC Genito-Urinary group, Australian Bladder Cancer Study Group, National Cancer Institute of Canada Clinical Trials Group, Finnbladder, Norwegian Bladder Cancer Study Group, Club Urologico Espanol de Tratamiento Oncologico (CUETO) Group. Neoadjuvant cisplatin, methotrexate, and vinblastine chemotherapy for muscle-invasive bladder cancer: a rando-mised controlled trial. International collaboration of trialists. Lancet 1999; 354:533e40.
doi: 10.1016/S0140-6736(99)02292-8
|
| [7] |
International Collaboration of Trialists; Medical Research Council Advanced Bladder Cancer Working Party (now the National Cancer Research Institute Bladder Cancer Clinical Studies Group); European Organisation for Research and Treatment of Cancer Genito-Urinary Tract Cancer Group; Australian Bladder Cancer Study Group; National Cancer Institute of Canada Clinical Trials Group; Finnbladder, et al. International phase III trial assessing neoadjuvant cisplatin, methotrexate, and vinblastine chemotherapy for muscle-invasive bladder cancer: long-term results of the BA06 30894 trial. J Clin Oncol 2011; 29:2171e7.
doi: 10.1200/JCO.2010.32.3139
pmid: 21502557
|
| [8] |
Grossman HB, Natale RB, Tangen CM, Speights VO, Vogelzang NJ, Trump DL, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med 2003; 349:859e66.
doi: 10.1056/NEJMoa022148
|
| [9] |
Sherif A, Holmberg L, Rintala E, Mestad O, Nilsson J, Nilsson S, et al. Neoadjuvant cisplatinum based combination chemotherapy in patients with invasive bladder cancer: a combined analysis of two Nordic studies. Eur Urol 2004; 45: 297e303.
doi: 10.1016/j.eururo.2003.09.019
pmid: 15036674
|
| [10] |
Advanced Bladder Cancer ABC Meta-analysis Collaboration. Neoadjuvant chemotherapy in invasive bladder cancer: up-date of a systematic review and meta-analysis of individual patient data advanced bladder cancer (ABC) meta-analysis collaboration. Eur Urol 2005; 48:202e6.
doi: 10.1016/j.eururo.2005.04.006
|
| [11] |
Rosenblatt R, Sherif A, Rintala E, Wahlqvist R, Ullén A, Nilsson S, et al. Pathologic downstaging is a surrogate marker for ef?cacy and increased survival following neoadjuvant chemotherapy and radical cystectomy for muscle-invasive urothelial bladder cancer. Eur Urol 2012; 61:1229e38.
doi: 10.1016/j.eururo.2011.12.010
pmid: 22189383
|
| [12] |
Meleis L, Moore R, Inman BA, Harrison MR. Retrospective analysis of the ef?cacy and safety of neoadjuvant gemcita-bine and cisplatin in muscle-invasive bladder cancer. J Oncol Pharm Pract 2020; 26:330e7.
doi: 10.1177/1078155219845434
pmid: 31081469
|
| [13] |
Vashistha V, Wang H, Mazzone A, Liss MA, Svatek RS, Schleicher M, et al. Radical cystectomy compared to combined modality treatment for muscle-invasive bladder cancer: a systematic review and meta-analysis. Int J Radiat Oncol Biol Phys 2017; 97:1002e20.
doi: 10.1016/j.ijrobp.2016.11.056
|
| [14] |
Premo C, Apolo AB, Agarwal PK, Citrin DE. Trimodality therapy in bladder cancer: who, what, and when? Urol Clin 2015; 42: 169e80.
|
| [15] |
Shipley WU, Kaufman DS, Zehr E, Heney NM, Lane SC, Thakral HK, et al. Selective bladder preservation by com-bined modality protocol treatment: long-term outcomes of 190 patients with invasive bladder cancer. Urology 2002; 60: 62e8.
pmid: 12100923
|
| [16] |
Cahn DB, Handorf EA, Ghiraldi EM, Ristau BT, Geynisman DM, Churilla TM, et al. Contemporary use trends and survival outcomes in patients undergoing radical cystectomy or bladder-preservation therapy for muscle-invasive bladder cancer. Cancer 2017; 123:4337e45.
|
| [17] |
Duplisea JJ, Mason RJ, Reichard CA, Li R, Shen Y, Boorjian SA, et al. Trends and disparities in the use of neoadjuvant chemotherapy for muscle-invasive urothelial carcinoma. Can Urol Assoc J 2019; 13:24e8.
|
| [18] |
Haque W, Verma V, Butler EB, Teh BS. Radical cystectomy versus chemoradiation for muscle-invasive bladder cancer: impact of treatment facility and sociodemographics. Anti-cancer Res 2017; 37:5603e8.
|
| [19] |
Martini T, Gilfrich C, Mayr R, Burger M, Pycha A, Aziz A, et al. The use of neoadjuvant chemotherapy in patients with uro-thelial carcinoma of the bladder: current practice among clinicians. Clin Genitourin Cancer 2017; 15:356e62.
doi: 10.1016/j.clgc.2016.09.003
|
| [20] |
Reardon ZD, Patel SG, Zaid HB, Stimson CJ, Resnick MJ, Keegan KA, et al. Trends in the use of perioperative chemo-therapy for localized and locally advanced muscle-invasive bladder cancer: a sign of changing tides. Eur Urol 2015; 67: 165e70.
doi: 10.1016/j.eururo.2014.01.009
|
| [21] |
Zaid HB, Patel SG, Stimson CJ, Resnick MJ, Cookson MS, Barocas DA, et al. Trends in the utilization of neoadjuvant chemotherapy in muscle-invasive bladder cancer: results from the National Cancer Database. Urology 2014; 83:75e80.
doi: 10.1016/j.urology.2013.07.072
pmid: 24231210
|
| [22] |
Joshi SS, Handorf ER, Smaldone MC, Geynisman DM. What can the National Cancer Database tell us about disparities in advanced bladder cancer outcomes? Transl Androl Urol 2018; 7:732e5.
doi: 10.21037/tau.2018.06.16
pmid: 30211063
|
| [23] |
Audenet F, Waingankar N, Ferket BS, Niglio SA, Marqueen KE, Sfakianos JP, et al. Effectiveness of transurethral resection plus systemic chemotherapy as de?nitive treatment for mus-cle invasive bladder cancer in population level data. J Urol 2018; 200:996e1004.
doi: 10.1016/j.juro.2018.06.001
|
| [24] |
Gray PJ, Fedewa SA, Shipley WU, Efstathiou JA, Lin CC, Zietman AL, et al. Use of potentially curative therapies for muscle-invasive bladder cancer in the United States: results from the National Cancer Data Base. Eur Urol 2013; 63:823e9.
doi: 10.1016/j.eururo.2012.11.015
pmid: 23200811
|
| [25] |
Trenta P, Calabrò F, Cerbone L, Sternberg CN. Chemotherapy for muscle-invasive bladder cancer. Curr Treat Options Oncol 2016; 17:6. https://doi.org/10.1007/s11864-015-0376-y.
|
| [26] |
Sandler HM, Mirhadi AJ. Current role of radiation therapy for bladder cancer. Semin Oncol 2012; 39:583e7.
doi: 10.1053/j.seminoncol.2012.08.005
pmid: 23040254
|
| [27] |
Mohamed HAH, Salem MA, Elnaggar MS, Gabr A, Abdelrheem AM. Trimodalities for bladder cancer in elderly: transurethral resection, hypofractionated radiotherapy and gemcitabine. Cancer Radiother 2018; 22:236e40.
doi: S1278-3218(18)30042-8
pmid: 29678595
|
| [28] |
Fedeli U, Fedewa SA, Ward EM. Treatment of muscle invasive bladder cancer: evidence from the National Cancer Database, 2003 to 2007. J Urol 2011; 185:72e8.
doi: 10.1016/j.juro.2010.09.015
pmid: 21074192
|
| [29] |
Canter D, Viterbo R, Kutikov A, Wong YN, Plimack E, Zhu F, et al. Baseline renal function status limits patient eligibility to receive perioperative chemotherapy for invasive bladder cancer and is minimally affected by radical cystectomy. Urology 2011; 77:160e5.
doi: 10.1016/j.urology.2010.03.091
pmid: 20709369
|
| [30] |
Dash A, Galsky MD, Vickers AJ, Serio AM, Koppie TM, Dalbagni G, et al. Impact of renal impairment on eligibility for adjuvant cisplatin-based chemotherapy in patients with urothelial carcinoma of the bladder. Cancer 2006; 107: 506e13.
doi: 10.1002/cncr.22031
pmid: 16773629
|
| [31] |
Apolo AB, Grossman HB, Bajorin D, Steinberg G, Kamat AM. Practical use of perioperative chemotherapy for muscle-invasive bladder cancer: summary of session at the Society of Urologic Oncology annual meeting. Urol Oncol 2012; 30:772e80.
doi: 10.1016/j.urolonc.2012.01.012
pmid: 23218068
|
| [32] |
Lindgren D, Frigyesi A, Gudjonsson S, Sj?dahl G, Hallden C, Chebil G, et al. Combined gene expression and genomic pro?ling de?ne two intrinsic molecular subtypes of urothelial carcinoma and gene signatures for molecular grading and outcome. Cancer Res 2010; 70:3463e72.
doi: 10.1158/0008-5472.CAN-09-4213
pmid: 20406976
|
| [33] |
Seiler R, Ashab HAD, Erho N, van Rhijn BWG, Winters B, Douglas J, et al. Impact of molecular subtypes in muscle-invasive bladder cancer on predicting response and survival after neoadjuvant chemotherapy. Eur Urol 2017; 72: 544e54.
doi: S0302-2838(17)30251-8
pmid: 28390739
|
| [34] |
Vollmer T, Schlickeiser S, Amini L, Schulenberg S, Wendering DJ, Banday V, et al. The intratumoral CXCR3 che-mokine system is predictive of chemotherapy response in human bladder cancer. Sci Transl Med 2021; 13:eabb3735. https://doi.org/10.1126/scitranslmed.abb3735.
doi: 10.1126/scitranslmed.abb3735
|
| [1] |
Chinna Babu Dracham,Narendra Kumar,Santosh Kumar,Arun Elangovan,Budhi Singh Yadav,Ravimohan S. Mavuduru,Anupam Lal,Pramod K. Gupta,Rakesh Kapoor. A phase II study of neoadjuvant chemotherapy followed by organ preservation in patients with muscle-invasive bladder cancer[J]. Asian Journal of Urology, 2022, 9(3): 318-328. |
| [2] |
Christian Winter,Andreas Hiester. Treatment of clinical stage I non-seminoma[J]. Asian Journal of Urology, 2021, 8(2): 161-169. |
| [3] |
Olivier Rouviere,Paul Cezar Moldovan. The current role of prostate multiparametric magnetic resonance imaging[J]. Asian Journal of Urology, 2019, 6(2): 137-145. |
| [4] |
Laurence Klotz. Contemporary approach to active surveillance for favorable risk prostate cancer[J]. Asian Journal of Urology, 2019, 6(2): 146-152. |
| [5] |
Kenneth Chen,Kae Jack Tay,Yan Mee Law,Hakan Aydin,Henry Ho,Christopher Cheng,John Shyi Peng Yuen. Outcomes of combination MRI-targeted and transperineal template biopsy in restaging low-risk prostate cancer for active surveillance[J]. Asian Journal of Urology, 2018, 5(3): 184-193. |
| [6] |
Wei Wang, Haitao Liu, Shujie Xia. Thulium laser treatment for bladder cancer[J]. Asian Journal of Urology, 2016, 3(3): 130-133. |
|
|
|
|