|
|
|
| A phase II study of neoadjuvant chemotherapy followed by organ preservation in patients with muscle-invasive bladder cancer |
Chinna Babu Drachama,Narendra Kumara,*( ),Santosh Kumarb,Arun Elangovana,Budhi Singh Yadava,Ravimohan S. Mavudurub,Anupam Lalc,Pramod K. Guptad,Rakesh Kapoora ),Santosh Kumarb,Arun Elangovana,Budhi Singh Yadava,Ravimohan S. Mavudurub,Anupam Lalc,Pramod K. Guptad,Rakesh Kapoora
|
aDepartment of Radiotherapy & Oncology, PGIMER, Chandigarh, India
bDepartment of Urology, PGIMER, Chandigarh, India
cDepartment of Radiodiagnosis, PGIMER, Chandigarh, India
dDepartment of Biostatistics, PGIMER, Chandigarh, India |
|
|
|
|
Abstract Objective: Conservative approaches in muscle-invasive bladder cancer (MIBC) have been evolved to avoid aggressive surgery, but are limited to elderly, frail, and patients medically unfit for surgery. Our study aimed to assess the response rate of neoadjuvant chemotherapy (NACT) before radiotherapy (RT) in MIBC patients.
Methods: Forty patients with urothelial carcinoma of stage T2-T4a, N0, M0 were enrolled between November 2013 and November 2015, and treated with three cycles of NACT with gemcitabine-cisplatin. Post-NACT response was assessed using Response Evaluation Criteria in Solid Tumors (RECIST) criteria. Patients who achieved complete response (CR) and partial response (PR) >50% were treated with radical RT, and those who had PR <50%, stable disease (SD), and progressive disease (PD) underwent radical cystectomy (RC). Survival analysis was done with Kaplan-Meier method and point-to-time events were analyzed with Cox-proportional hazards regression model.
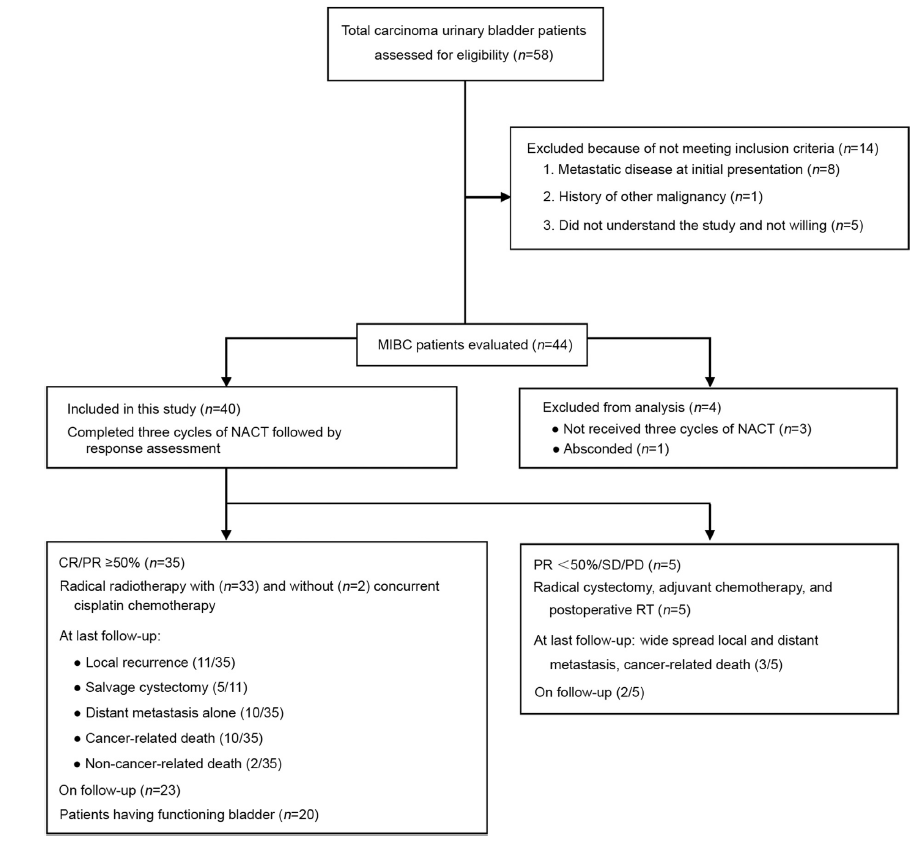
Results: After NACT, 35 (87.5%) patients achieved either PR >50% or CR, and were treated with RT. Five (12.5%) patients who had PR <50%, SD, or PD underwent RC. All patients who received radiation showed CR after 6 weeks. Median follow-up was 43 months (range: 10-66 months) and median overall survival (OS) was not reached. Three-year OS, local control, and disease-free survival were 70.1%, 60.9%, 50.6%, respectively, and 50% of patients preserved their functioning bladder. Three-year OS rate was 88.9% in patients who achieved CR to NACT, 73.1% in patients with PR ≥50% and 40% in patients with PR <50%.
Conclusion: NACT followed by RT provides a high probability of local response with bladder preservation in CR patients. Appropriate use of this treatment regimen in carefully selected patients may omit the need for morbid surgery.
|
|
Received: 11 January 2020
Available online: 20 July 2022
|
|
Corresponding Authors:
Narendra Kumar
E-mail: drnarendra74@gmail.com
|
|
|
|
|
Study flowchart with a summary of methods and results. CR, complete response; NACT, neoadjuvant chemotherapy; PD, progressive disease; PR, partial response; SD, stable disease; MIBC, muscle-invasive bladder cancer; RT, radiotherapy.
|

| Characteristic | Patient, n (%) | | Transitional cell carcinoma | 40 (100) | | High grade | 40 (100) | | Carcinoma in situ | 5 (12.5) | | T stage | | T2 | 18 (45) | | T3 | 16 (40) | | T4a | 6 (15) | | N stage | | N0 | 40 (100) | | Composite stage (AJCC 2010) | | II | 18 (45) | | III | 22 (55) | | Comorbidities | | Hypertension | 10 (25) | | Diabetes | 6 (15) | | Coronary artery disease | 4 (10) | | Hydroureteronephrosis | 4 (10) | | Smoking and alcohol intake | 20 (50) |
|
|
Disease and patient characteristics.
|
|
|
Survival function curves estimated by Kaplan-Meier method along with their 95% confidence interval bands (at any time point, there is a 95% chance that the interval band contains true percentage survival). (A) Overall survival; (B) Disease-free survival; (C) Local control.
|
|
|
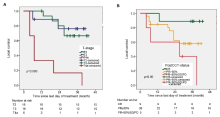
Survival function curve computed by Kaplan-Meier method. (A) For local control with tumor (T) stage; (B) With NACT response. CR, complete response; NACT, neoadjuvant chemotherapy; PD, progressive disease; PR, partial response; SD, stable disease; PostCCT-status, post-chemotherapy (NACT) status.
|
|
|
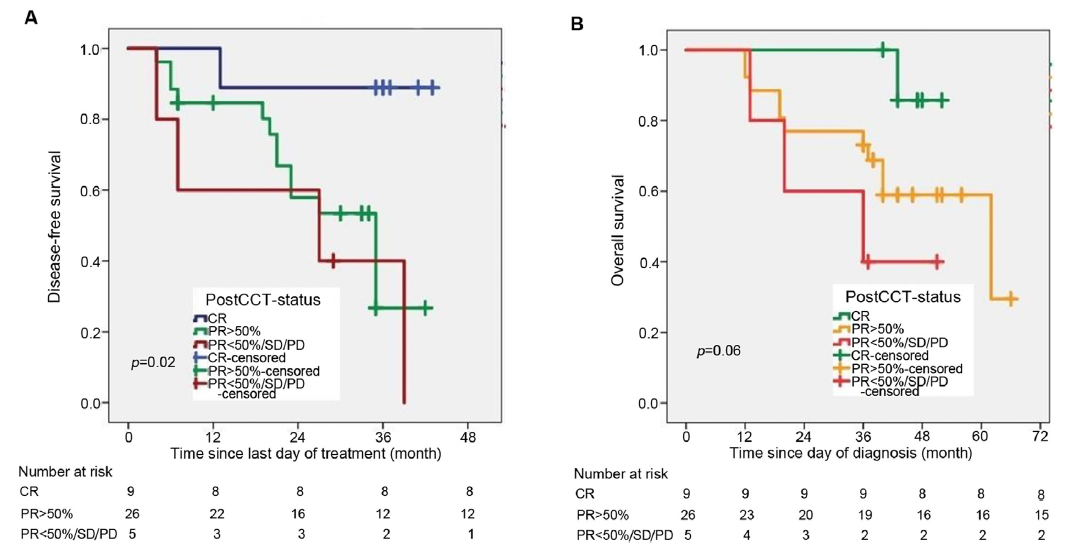
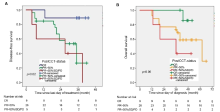
Survival function curve computed by Kaplan-Meier method. (A) For disease-free survival with NACT response; (B) For overall survival with NACT response. CR, complete response; NACT, neoadjuvant chemotherapy; PD, progressive disease; PR, partial response; SD, stable disease; PostCCT-status, post-chemotherapy (NACT) status.
|
| Variable (n) | Local control | Disease-free survival | Overall survival | | 3-year, % | p-Value | 3-year, % | p-Value | 3-year, % | p-Value | | Composite stage | | 0.05 | | 0.07 | | 0.22 | | II (18) | 74.0 | | 60.0 | | 77.8 | | | III (22) | 42.1 | | 51.0 | | 68.2 | | | T-stage | | 0.00 | | 0.00 | | 0.06 | | T2 (18) | 76.2 | | 60.7 | | 77.8 | | | T3 (16) | 60.0 | | 53.0 | | 65.0 | | | T4a (6) | 16.2 | | 16.7 | | 33.3 | | | Response to NACT | | 0.05 | | 0.02 | | 0.06 | | CR (9) | 85.7 | | 85.7 | | 88.9 | | | PR≥50% (26) | 57.9 | | 40.4 | | 73.1 | | | PR<50%/SD/PD (5) | 40.0 | | 26.7 | | 40.0 | |
|
|
Local control, disease-free survival, and overall survival, analyses with Kaplan-Meier method using log-rank test.
|
| Variable | Number of events/number of patients | Median time in months (95% CI) | Hazard ratio (95% CI) | p-Value | | Local control (n=15) | | Age | | | 0.57 (0.19-1.71) | 0.34 | | ≤60 years | 10/22 | 29.0 (23.3-34.6) | | | | >60 years | 5/18 | 35.0 (28.8-41.3) | | | | Comorbidity | | | 0.66 (0.22-1.97) | 0.72 | | Yes | 5/12 | 30.6 (22.2-39.1) | | | | No | 10/28 | 32.4 (27.3-37.5) | | | | T stage | | | 6.93 (2.03-20.67) | 0.00 | | T2 | 4/18 | Not estimablea | | | | T3 | 5/16 | 35.9 (30.6-41.2) | | | | T4a | 6/6 | 13.5 (2.4-24.5) | | | | Composite stage | | | 0.19 (0.22-1.73) | 0.14 | | II | 4/18 | 34.8 (29.2-40.3) | | | | III | 11/22 | 29.2 (23.0-35.4) | | | | NACT response | | | 2.72 (1.17-6.31) | 0.05 | | CR | 1/9 | Not estimablea | | | | PR≥50% | 10/26 | 31.2 (25.7-36.6) | | | | PR<50%/SD/PD | 4/5 | 23.2 (7.8-38.5) | | | | Disease-free survival (n=19) | | Age | | | 0.60 (0.22-1.64) | 0.60 | | ≤60 years | 12/22 | 27.4 (22.3-32.4) | | | | >60 years | 7/18 | 32.1 (25.6-38.7) | | | | Comorbidity | | | 0.86 (0.30-2.46) | 0.86 | | Yes | 5/12 | 30.6 (22.2-39.1) | | | | No | 14/28 | 35.0 (25.6-35.6) | | | | T stage | | | 4.43 (1.44-13.6) | 0.001 | | T2 | 6/18 | Not estimablea | | | | T3 | 7/16 | 33.0 (27.3-38.6) | | | | T4a | 6/6 | 13.5 (2.4-24.7) | | | | Composite stage | | | 0.35 (0.05-2.37) | 0.28 | | II | 6/18 | 34.6 (29.3-39.8) | | | | III | 13/22 | 27.2 (21.2-33.2) | | | | NACT response | | | 2.62 (1.28-5.36) | 0.01 | | CR | 1/9 | Not estimablea | | | | PR≥50% | 14/26 | 28.3 (23.2-33.3) | | | | PR<50%/SD/PD | 4/5 | 23.2 (7.8-35.5) | | | | Overall survival (n=15) | | Age | | | 0.83 (0.28-2.45) | 0.76 | | ≤60 years | 8/22 | 44.9 (38.3-51.4) | | | | >60 years | 7/18 | 50.5 (41.0-60.7) | | | | Comorbidity | | | 0.86 (0.26-2.82) | 0.55 | | Yes | 4/12 | 39.8 (30.3-49.6) | | | | No | 11/28 | 51.0 (44.1-58.0) | | | | T stage | | | 2.01 (0.96-4.26) | 0.06 | | T2 | 4/18 | Not estimablea | | | | T3 | 7/16 | 47.0 (39.1-54.8) | | | | T4a | 4/6 | 28.3 (14.7-41.2) | | | | Composite stage | | | 0.54 (0.06-4.55) | 0.20 | | II | 4/18 | 47.0 (39.1-54.8) | | | | III | 11/22 | 47.6 (39.6-55.7) | | | | NACT response | | | 2.62 (1.06-6.47) | 0.03 | | CR | 1/9 | Not estimablea | | | | PR≥50% | 11/26 | 48.2 (40.1-56.3) | | | | PR<50%/SD/PD | 3/5 | 34.2 (20.5-47.8) | | |
|
|
Univariate analyses for survival end points (local control, disease-free survival, and overall survival).
|
| NACT response | Local control | Disease-free survival | Overall survival | | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | | CR | 1 | 0.05 | 1 | 0.01 | 1 | 0.03 | | PR ≥50% | 1.47 (0.14-1.96) | 0.46 | 1.75 (0.22-2.18) | 0.87 | 1.51 (0.14-1.88) | 0.65 | | PR <50%/SD/PD | 2.72 (1.17-6.31) | 0.02 | 2.62 (1.28-5.36) | 0.023 | 2.26 (1.06-6.47) | 0.04 |
|
|
Multivariate analyses for survival end points with Cox-proportional hazard regression model.
|
| [1] |
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68:394e424.
|
| [2] |
Mathur P, Sathishkumar K, Chaturvedi M, Das P, Sudarshan KL, Santhappan S, et al. ICMR-NCDIR-NCRP Investigator Group Cancer statistics, 2020:report from National Cancer Registry Programme, India. JCO Glob Oncol 2020; 6:1063e75.
|
| [3] |
Milowsky MI, Rumble RB, Booth CM, Gilligan T, Eapen LJ, Hauke RJ, et al. Guideline on muscle-invasive and metastatic bladder cancer (European Association of Urology guideline): American Society of Clinical Oncology Clinical Practice guideline endorsement. J Clin Oncol 2016; 34: 1945e52.
|
| [4] |
International Collaboration of Trialists, Medical Research Council Advanced Bladder Cancer Working Party (now the National Cancer Research Institute Bladder Cancer Clinical Studies Group), European Organisation for Research and Treatment of Cancer Genito-Urinary Tract Cancer Group, Australian Bladder Cancer Study Group, National Cancer Institute of Canada Clinical Trials Group, Finnbladder, Norwegian Bladder Cancer Study Group, Club Urologico Espanol de Tratamiento Oncologico Group, Griffiths G, Hall R, Sylvester R, Raghavan D, Parmar MK. International phase III trial assessing neoadjuvant cisplatin, methotrexate, and vinblastine chemotherapy for muscle-invasive bladder cancer: long-term results of the BA06 30894 trial. J Clin Oncol 2011; 29: 2171e7.
|
| [5] |
Hautmann RE, Gschwend JE, de Petriconi RC, Kron M, Volkmer BG. Cystectomy for transitional cell carcinoma of the bladder: results of a surgery only series in the neobladder era. J Urol 2006; 176:486e92.
doi: 10.1016/j.juro.2006.03.038
pmid: 16813874
|
| [6] |
Christodouleas JP, Baumann BC, He J, Hwang WT, Tucker KN, Bekelman JE, et al. Optimizing bladder cancer locoregional failure risk stratification after radical cystectomy using SWOG 8710. Cancer 2014; 120:1272e80.
doi: 10.1002/cncr.28544
pmid: 24390799
|
| [7] |
Madersbacher S, Hochreiter W, Burkhard F, Thalmann GN, Danuser H, Markwalder R, et al. Radical cystectomy for bladder cancer todayda homogeneous series without neoadjuvant therapy. J Clin Oncol 2003; 21:690e6.
pmid: 12586807
|
| [8] |
Hautmann RE, de Petriconi RC, Pfeiffer C, Volkmer BG. Radical cystectomy for urothelial carcinoma of the bladder without neoadjuvant or adjuvant therapy: long-term results in 1100 patients. Eur Urol 2012; 61:1039e47.
doi: 10.1016/j.eururo.2012.02.028
pmid: 22381169
|
| [9] |
Advanced Bladder Cancer ABC Meta-analysis Collaboration. Neoadjuvant chemotherapy in invasive bladder cancer: update of a systematic review and meta-analysis of individual patient data advanced bladder cancer (ABC) meta-analysis collaboration. Eur Urol 2005; 48:202e6.
doi: 10.1016/j.eururo.2005.04.006
|
| [10] |
von der Maase H, Hansen SW, Roberts JT, Dogliotti L, Oliver T, Moore MJ, et al. Gemcitabine and cisplatin versus methotrexate, vinblastine, doxorubicin, and cisplatin in advanced or metastatic bladder cancer: results of a large, randomized, multinational, multicenter, phase III study. J Clin Oncol 2000; 18:3068e77.
doi: 10.1200/JCO.2000.18.17.3068
pmid: 11001674
|
| [11] |
Shelley MD, Cleves A, Wilt TJ, Mason MD. Gemcitabine chemotherapy for the treatment of metastatic bladder carcinoma. BJU Int 2011; 108:168e79.
doi: 10.1111/j.1464-410X.2011.10341.x
|
| [12] |
Holma¨ng S, Hedelin H, Borghede G, Johansson SL. Long-term followup of a bladder carcinoma cohort: questionable value of radical radiotherapy. J Urol 1997; 157:1642e6.
doi: 10.1016/S0022-5347(01)64818-3
|
| [13] |
Efstathiou JA, Spiegel DY, Shipley WU, Heney NM, Kaufman DS, Niemierko A, et al. Long-term outcomes of selective bladder preservation by combined-modality therapy for invasive bladder cancer: the MGH experience. Eur Urol 2012; 61:705e11.
doi: 10.1016/j.eururo.2011.11.010
pmid: 22101114
|
| [14] |
Rödel C, Grabenbauer GG, KÜhn R, Papadopoulos T, Dunst J, Meyer M, et al. Combined-modality treatment and selective organ preservation in invasive bladder cancer: long-term results. J Clin Oncol 2002; 20:3061e71.
|
| [15] |
Huddart RA, Hall E, Hussain SA, Jenkins P, Rawlings C, Tremlett J, et al. Randomized noninferiority trial of reduced high-dose volume versus standard volume radiation therapy for muscle-invasive bladder cancer: results of the BC 2001 trial (CRUK/01/004). Int J Radiat Oncol Biol Phys 2013; 87:261e9.
doi: 10.1016/j.ijrobp.2013.06.2044
|
| [16] |
Giacalone NJ, Shipley WU, Clayman RH, Niemierko A, Drumm M, Heney NM, et al. Long-term outcomes after bladder-preserving tri-modality therapy for patients with muscle-invasive bladder cancer: an updated analysis of the Massachusetts general hospital experience. Eur Urol 2017; 71:952e60.
doi: S0302-2838(16)30924-1
pmid: 28081860
|
| [17] |
Kulkarni GS, Hermanns T, Wei Y, Bhindi B, Satkunasivam R, Athanasopoulos P, et al. Propensity score analysis of radical cystectomy versus bladder-sparing trimodal therapy in the setting of a multidisciplinary bladder cancer clinic. J Clin Oncol 2017; 35:2299e305.
doi: 10.1200/JCO.2016.69.2327
pmid: 28410011
|
| [18] |
Uysal B, Beyzadeoglu M, Demiral S, Gamsiz H, Dincoglan F, Sager O, et al. Outcomes of trimodality approach in the management of T2N0M 0 bladder cancer. Tumori 2015; 101:232e7.
doi: 10.5301/tj.5000294
pmid: 25768321
|
| [19] |
Huddart RA, Birtle A, Maynard L, Beresford M, Blazeby J, Donovan J, et al. Clinical and patient-reported outcomes of SPAREda randomised feasibility study of selective bladder preservation versus radical cystectomy. BJU Int 2017; 120: 639e50.
doi: 10.1111/bju.13900
pmid: 28453896
|
| [20] |
Khaled HM, Shafik HE, Zabhloul MS, Ghoneim M, Saber RA, Manie M, et al. Gemcitabine and cisplatin as neoadjuvant chemotherapy for invasive transitional and squamous cell carcinoma of the bladder: effect on survival and bladder preservation. Clin Genitourin Cancer 2014; 12:e233e40. https://doi.org/10.1016/j.clgc.2014.04.002.
doi: 10.1016/j.clgc.2014.04.002
|
| [21] |
Jiang DM, Jiang H, Chung PWM, Zlotta AR, Fleshner NE, Bristow RG, et al. Neoadjuvant chemotherapy before bladdersparing chemoradiotherapy in patients with nonmetastatic muscle-invasive bladder cancer. Clin Genitourin Cancer 2019; 17:38e45.
doi: 10.1016/j.clgc.2018.09.021
|
| [22] |
Redpath AT, Muren LP. CT-guided intensity-modulated radiotherapy for bladder cancer: isocentre shifts, margins and their impact on target dose. Radiother Oncol 2006; 81:276e83.
doi: 10.1016/j.radonc.2006.10.017
|
| [23] |
McBain CA, Logue JP. Radiation therapy for muscle-invasive bladder cancer: treatment planning and delivery in the 21st century. Semin Radiat Oncol 2005; 15:42e8.
doi: 10.1016/j.semradonc.2004.07.015
|
| [24] |
Logue J, McBain CA. Radiation therapy for muscle-invasive bladder cancer: treatment planning and delivery. Clin Oncol (R Coll Radiol) 2005; 17:508e13.
doi: 10.1016/j.clon.2005.07.004
|
| [25] |
Kamat AM, Hahn NM, Efstathiou JA, Lerner SP, Malmström PU, Choi W, et al. Bladder cancer. Lancet 2016; 388:2796e810.
doi: 10.1016/S0140-6736(16)30512-8
|
| [26] |
Sternberg CN, Yagoda A, Scher HI, Watson RC, Ahmed T, Weiselberg LR, et al. Preliminary results of M-VAC (methotrexate, vinblastine, doxorubicin and cisplatin) for transitional cell carcinoma of the urothelium. J Urol 1985; 133:403e7.
|
| [27] |
Grossman HB, Natale RB, Tangen CM, Speights VO, Vogelzang NJ, Trump DL, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med 2003; 349:859e66.
doi: 10.1056/NEJMoa022148
|
| [28] |
Yeshchina O, Badalato GM, Wosnitzer MS, Hruby G, RoyChoudhury A, Benson MC, et al. Relative efficacy of perioperative gemcitabine and cisplatin versus methotrexate, vinblastine, adriamycin, and cisplatin in the management of locally advanced urothelial carcinoma of the bladder. Urology 2012; 79:384e90.
doi: 10.1016/j.urology.2011.10.050
pmid: 22196406
|
| [29] |
Yuh BE, Ruel N, Wilson TG, Vogelzang N, Pal SK. Pooled analysis of clinical outcomes with neoadjuvant cisplatin and gemcitabine chemotherapy for muscle invasive bladder cancer. J Urol 2013; 189:1682e6.
doi: 10.1016/j.juro.2012.10.120
|
| [30] |
Mertens LS, Meijer RP, Meinhardt W, van der Poel HG, Bex A, Kerst JM, et al. Occult lymph node metastases in patients with carcinoma invading bladder muscle: incidence after neoadjuvant chemotherapy and cystectomy vs. after cystectomy alone. BJU Int 2014; 114:67e74.
doi: 10.1111/bju.12447
pmid: 24053889
|
| [31] |
Nowak-Sadzikowska J, Jakubowicz J, Skóra T, Pudełek K. Transurethral resection, neoadjuvant chemotherapy and accelerated hyperfractionated radiotherapy (concomitant boost), with or without concurrent cisplatin, for patients with invasive bladder cancerdclinical outcome. Contemp Oncol (Pozn) 2013; 17:302e6.
|
| [32] |
Shipley WU, Winter KA, Kaufman DS, Lee WR, Heney NM, Tester WR, et al. Phase III trial of neoadjuvant chemotherapy in patients with invasive bladder cancer treated with selective bladder preservation by combined radiation therapy and chemotherapy: initial results of Radiation Therapy Oncology Group 89-03. J Clin Oncol 1998; 16:3576e83.
pmid: 9817278
|
| [33] |
Shipley WU, Kaufman DS, Tester WJ, Pilepich MV, Sandler HM, Radiation Therapy Oncology Group. Overview of bladder cancer trials in the Radiation Therapy Oncology Group. Cancer 2003; 97: 2115e9.
|
| [34] |
Rosenblatt R, Sherif A, Rintala E, Wahlqvist R, Ullén A, Nilsson S, et al. Nordic Urothelial Cancer Group. Pathologic downstaging is a surrogate marker for efficacy and increased survival following neoadjuvant chemotherapy and radical cystectomy for muscle-invasive urothelial bladder cancer. Eur Urol 2012; 61:1229e38.
doi: 10.1016/j.eururo.2011.12.010
pmid: 22189383
|
| [35] |
McHaffie DR, Kruser TJ, Gaston K, Mahoney J, Graham D, HaakeM. Chemoradiation for organ preservation inthe treatment of muscle-invasive bladder cancer. Urol Oncol 2016; 34:271e8.
doi: 10.1016/j.urolonc.2016.03.011
pmid: 27108225
|
| [36] |
Zietman AL, Sacco D, Skowronski U, Gomery P, Kaufman DS, Clark JA, et al. Organ conservation in invasive bladder cancer by transurethral resection, chemotherapy and radiation: results of a urodynamic and quality of life study on long-term survivors. J Urol 2003; 170:1772e6.
doi: 10.1097/01.ju.0000093721.23249.c3
|
| [37] |
Herr HW, Faulkner JR, Grossman HB, Natale RB, deVere White R, Sarosdy MF, et al. Surgical factors influence bladder cancer outcomes: a cooperative group report. J Clin Oncol 2004; 22:2781e9.
|
| [38] |
Baumann BC, Sargos P, Eapen LJ, Efstathiou JA, Choudhury A, Bahl A, et al. The rationale for post-operative radiation in localized bladder cancer. Bladder Cancer 2017; 33:19e30.
|
| [39] |
Zaghloul MS, Christodouleas JP, Smith A, Abdallah A, William H, Khaled HM, et al. Adjuvant sandwich chemotherapy plus radiotherapy vs. adjuvant chemotherapy alone for locally advanced bladder cancer after radical cystectomy: a randomized phase 2 trial. JAMA Surg 2018; 153:e174591. https://doi.org/10.1001/jamasurg.2017.4591.
|
| [1] |
Francesco Claps,Maria Carmen Mir,Homayoun Zargar. Molecular markers of systemic therapy response in urothelial carcinoma[J]. Asian Journal of Urology, 2021, 8(4): 376-390. |
| [2] |
Mengzhu Liu,Kun Jin,Shi Qiu,Pengyong Xu,Mingming Zhang,Wufeng Cai,Xiaonan Zheng,Lu Yang,Qiang Wei. Oncological outcomes of patients with ductal adenocarcinoma of the prostate receiving radical prostatectomy or radiotherapy[J]. Asian Journal of Urology, 2021, 8(2): 227-234. |
| [3] |
Sunny Goel,Rahul J. Sinha,Ved Bhaskar,Ruchir Aeron,Ashish Sharma,Vishwajeet Singh. Role of gemcitabine and cisplatin as neoadjuvant chemotherapy in muscle invasive bladder cancer: Experience over the last decade[J]. Asian Journal of Urology, 2019, 6(3): 222-229. |
| [4] |
Michel Bolla,Ann Henry,Malcom Mason,Thomas Wiegel. The role of radiotherapy in localised and locally advanced prostate cancer[J]. Asian Journal of Urology, 2019, 6(2): 153-161. |
| [5] |
Rei Umezawa,Koji Inaba,Satoshi Nakamura,Akihisa Wakita,Hiroyuki Okamoto,Keisuke Tsuchida,Tairo Kashihara,Kazuma Kobayashi,Ken Harada,Kana Takahashi,Naoya Murakami,Yoshinori Ito,Hiroshi Igaki,Keiichi Jingu,Jun Itami. Dose escalation of external beam radiotherapy for high-risk prostate cancer—Impact of multiple high-risk factor[J]. Asian Journal of Urology, 2019, 6(2): 192-199. |
|
|
|
|