|
|
|
| Comparison of post-urethroplasty complication rates in pediatric cases with hypospadias using Vicryl or polydioxanone sutures |
Mehdi Shirazia,Abdolreza Haghpanaha,*( ),Anahita Dehghania,Sezaneh Haghpanahb,Mehdi Ghahartarsc,Mahdi Rahmaniand ),Anahita Dehghania,Sezaneh Haghpanahb,Mehdi Ghahartarsc,Mahdi Rahmaniand
|
a Shiraz Nephro-urology Research Center, Shiraz University of Medical Sciences, Shiraz, Iran
b Hematology Research Center, Shiraz University of Medical Sciences, Shiraz, Iran
c Molecular Dermatology Research Center, Shiraz University of Medical Sciences, Shiraz, Iran
d Medical School, MPH Department, Shiraz University of Medical Sciences, Shiraz, Iran |
|
|
|
|
Abstract Objective: Hypospadias is a common congenital problem among male newborns. Both rapid absorbable sutures (polyglactin, Vicryl) and delayed absorbable sutures (polydioxanone, PDO) are used in hypospadias repair based on the surgeon's preference. This study was conducted to compare post-urethroplasty complication rates in pediatric patients with hypospadias using Vicryl or PDO sutures. Methods: This is a retrospective study which was designed and performed on 583 children aged 1-7 years old who had undergone hypospadias repair from January 2012 to December 2018. Required data were obtained from the patients' medical records. Results: Overall, post-surgical complications were observed in 60 (10.3%) patients comprising urethro-cutaneous fistula (n=39, 6.7%), meatal stenosis (n=10, 1.7%), urethral stricture (n=7, 1.2%), and glans dehiscence (n=4, 0.7%). The mean age of the children with complications was 3.0±1.3 years. According to Kaplan-Meier estimate, the interval between surgery and development of complications was significantly shorter in the Vicryl group (p=0.037). Overall, complications were more prevalent in Vicryl suture than PDO suture (15.1% vs. 5.3%, p<0.001). Regression model revealed that in comparison to the distal type, proximal hypospadias (odds ratio [OR]:103.9, 95% confidence interval [CI]: 32.2-334.9, p<0.001) and mid-shaft hypospadias (OR: 82.9, 95% CI: 25.9-264.6, p<0.001) while using Vicryl suture instead of PDO suture (OR: 62.4, 95% CI: 21.2-183.8, p<0.001) increased the odds of developing post-urethroplasty complications. Conclusion: We suggest PDO suture in the repair of hypospadias due to its lower complication rate, especially in cases of proximal and mid-shaft hypospadias which can get more complicated than the distal type.
|
|
Received: 25 July 2020
Available online: 20 April 2022
|
|
Corresponding Authors:
Abdolreza Haghpanah
E-mail: rezahaghpanah@yahoo.com
|
|
|

| Parameter | Complication, n (%) | p-Value | | Hypospadias type | | <0.001 | | Distal (n=374) | 16 (4.3) | | | Mid-shaft (n=125) | 22 (17.6) | | Proximal (n=84) | 22 (26.2) | | Suture type | | <0.001 | | Vicryl (n=298) | 45 (15.1) | | | PDO (n=285) | 15 (5.3) |
|
|
Comparison of the frequencies of post-hypospadias repair complications based on hypospadias type and suture type.
|
| Complication | Vicryl, n (%) | PDO, n (%) | p-Valuea | | Urethro-cutaneous fistula | 27 (9.1) | 12 (4.2) | 0.460 | | Glans dehiscence | 4 (1.3) | 0 (0) | | Meatal stenosis | 8 (2.7) | 2 (0.7) | | Urethral stricture | 6 (2.0) | 1 (0.4) |
|
|
Comparison of post-surgical complication rates between Vicryl and PDO sutures in children with hypospadias repair.
|

|
|
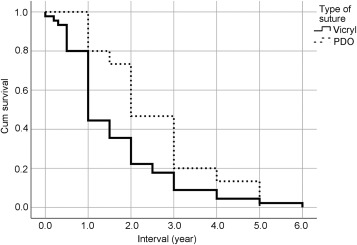
Kaplan-Meier survival plot showing time to develop post-surgical complications in the Vicryl and PDO groups. PDO, polydioxanone.
|
| Parameter | Regression coefficient | Standard error | p-Value | OR | 95% CI of OR | | Intercept | -6.883 | 0.6043 | <0.001 | 0.001 | 0.000-0.003 | | Hypospadias type (distal as reference) | | Proximal | 4.644 | 0.5971 | <0.001 | 103.9 | 32.2-334.9 | | Mid-shaft | 4.418 | 0.5921 | <0.001 | 82.9 | 25.9-264.6 | | Suture type (PDO as reference) | | Vicryl | 4.135 | 0.5507 | <0.001 | 62.4 | 21.2-183.8 |
|
|
Results of binary logistic regression.a
|
| [1] |
Kraft KH, Shukla AR, Canning DA. Hypospadias. Urol Clin 2010; 37:167-81.
|
| [2] |
Baskin LS, Ebbers MB. Hypospadias: Anatomy, etiology, and technique. J Pediatr Surg 2006; 41:463-72.
doi: 10.1016/j.jpedsurg.2005.11.059
|
| [3] |
Gilliver SC, Ashcroft GS. Sex steroids and cutaneous wound healing: The contrasting influences of estrogens and androgens. Climacteric 2007; 10:276-88.
pmid: 17653954
|
| [4] |
Ulman I, Erikci V, Avanoglu A, Gokdemir A. The effect of suturing technique and material on complication rate following hypospadias repair. Eur J Pediatr Surg 1997; 7:156-7.
pmid: 9241502
|
| [5] |
DiSandro M, Palmer JM. Stricture incidence related to suture material in hypospadias surgery. J Pediatr Surg 1996; 31: 881-4.
pmid: 8811548
|
| [6] |
Snodgrass W. Tubularized, incised plate urethroplasty for distal hypospadias. J Urol 1994; 151:464-5.
doi: 10.1016/s0022-5347(17)34991-1
pmid: 8283561
|
| [7] |
Smith DP. A comprehensive analysis of a tubularized incised plate hypospadias repair. Urology 2001; 57:778-81. discussion 81-2.
doi: 10.1016/S0090-4295(00)00947-X
|
| [8] |
Sugarman ID, Trevett J, Malone PS. Tubularization of the incised urethral plate (Snodgrass procedure) for primary hypospadias surgery. BJU Int 1999; 83:88-90.
pmid: 10233458
|
| [9] |
Uygur MC, Erol D, Germiyanoğlu C. Lessons from 197 Mathieu hypospadias repairs performed at a single institution. Pediatr Surg Int 1998; 14:192-4.
pmid: 9880746
|
| [10] |
Koyle MA. Hypospadias: A 30-year personal journey. Scand J Surg 2011; 100:250-5.
pmid: 22182846
|
| [11] |
Bellenger CR. Sutures. Part I. The purpose of sutures and available suture materials. Compend Continuing Educ Pract Vet 1982; 4:507-15.
|
| [12] |
Boothe HW. Selecting suture materials for small animal surgery. Compend Continuing Educ Pract Vet 1998; 20:155-63.
|
| [13] |
Castagnetti M, El-Ghoneimi A. Surgical management of primary severe hypospadias in children: Systematic 20-year review. J Urol 2010; 184:1469-74.
doi: 10.1016/j.juro.2010.06.044
pmid: 20727541
|
| [14] |
Lu W, Tao Y, Wisniewski AB, Frimberger D, Kropp BP. Different outcomes of hypospadias surgery between North America, Europe and China: Is patient age a factor? Nephro-Urol Mon 2012; 4:609-12.
doi: 10.5812/numonthly.1853
|
| [15] |
Snodgrass W, Villanueva C, Bush NC. Duration of follow-up to diagnose hypospadias urethroplasty complications. J Pediatr Urol 2014; 10:208-11.
doi: 10.1016/j.jpurol.2013.11.011
pmid: 24439629
|
| [16] |
Chung J-W, Choi SH, Kim BS, Chung SK. Risk factors for the development of urethrocutaneous fistula after hypospadias repair: A retrospective study. Kor J Urol 2012; 53:711-5.
|
| [17] |
Pfistermuller KL, McArdle AJ, Cuckow PM. Meta-analysis of complication rates of the tubularized incised plate (TIP) repair. J Pediatr Urol 2015; 11:54-9.
doi: 10.1016/j.jpurol.2014.12.006
pmid: 25819601
|
| [18] |
Castagnetti M, Zhapa E, Rigamonti W. Primary severe hypospadias: Comparison of reoperation rates and parental perception of urinary symptoms and cosmetic outcomes among 4 repairs. J Urol 2013; 189:1508-13.
doi: 10.1016/j.juro.2012.11.013
pmid: 23154207
|
| [19] |
Long CJ, Chu DI, Tenney RW, Morris AR, Weiss DA, Shukla AR, et al. Intermediate-term followup of proximal hypospadias repair reveals high complication rate. J Urol 2017; 197: 852-8.
doi: 10.1016/j.juro.2016.11.054
|
| [20] |
Cimador M, Castagnetti M, Milazzo M, Sergio M, De Grazia E. Suture materials: Do they affect fistula and stricture rates in flap urethroplasties? Urol Int 2004; 73: 320-4.
pmid: 15604576
|
| [21] |
Guarino N, Vallasciani SA, Marrocco G. A new suture material for hypospadias surgery: A comparative study. J Urol 2009; 181:1318e22. discussion 22-3.
|
| [22] |
Shirazi M, Noorafshan A, Serhan A. Effects of different suture materials used for the repair of hypospadias: A stereological study in a rat model. Urol Int 2012; 89:395-401.
doi: 10.1159/000343423
pmid: 23108502
|
|
|
|