|
|
|
| Initial experience with robot-assisted adrenalectomy for giant adrenal tumors |
Takayuki Ohzekia,*( ),Hiroyuki Kitaa,Remon Kunishigea,Taiji Hayashia,Tsukasa Nishiokaa,Koichi Sugimotob,Takafumi Minamic,Kazutoshi Fujitac ),Hiroyuki Kitaa,Remon Kunishigea,Taiji Hayashia,Tsukasa Nishiokaa,Koichi Sugimotob,Takafumi Minamic,Kazutoshi Fujitac
|
aDepartment of Urology, Izumi City General Hospital, 4-5-1 Wakecho, Izumi, Osaka 594-0073, Japan
bDepartment of Urology, Kaizuka City Hospital, 10-20 Hori 3-chome, Kaizuka, Osaka 594-0073, Japan
cDepartment of Urology, Kindai University Faculty of Medicine, 377-2 Ohno-Higashi, Osaka-Sayama, Osaka 589-8511, Japan |
|
|
|
|
|
|
Received: 10 March 2023
Available online: 20 July 2024
|
|
Corresponding Authors:
*E-mail address: takayuki.ozeki@tokushukai.jp (T. Ohzeki)
|
|
|
|
|
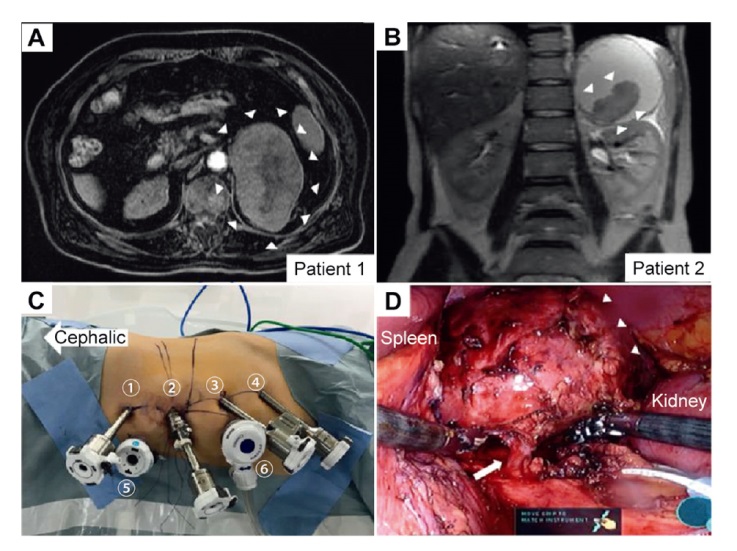
Imaging and intraoperative findings related to robotic-assisted adrenalectomy. (A) An 11.3 cm×6.2 cm substantial tumor (△) was found in the left adrenal gland, and the inside of the tumor showed a low absorption area that necrosis was suspected; (B) A 10 cm×10 cm cyst was observed in the left adrenal gland, and the contents indicated hyperintensity on both T1- and T2-weighted abdominal magnetic resonance imaging; a septum and a 52-mm solid component were found inside the cyst (△); (C) Ports for robotic adrenalectomy: ① 8 mm, port; ② 12 mm, camera; ③ 8 mm, port; ④ 8 mm, port; ⑤ 12 mm, assistant; and ⑥ 12 mm, assistant (AirSealTM Insufflation System, CONMED Japan KK, Tokyo, Japan); (D) Intraoperative findings for Patient 2; a blood vessel (arrow) flowing into a giant cyst (△) was observed, which was thought to be the central vein of the adrenal gland.
|
| [1] |
Kerkhofs TM, Verhoeven RH, Van der Zwan JM, Dieleman J, Kerstens MN, Links TP, et al. Adrenocortical carcinoma: a population-based study on incidence and survival in the Netherlands since 1993. Eur J Cancer 2013; 49:2579-86.
|
| [2] |
Kloos RT, Gross MD, Francis IR, Korobkin M, Shapiro B. Incidentally discovered adrenal masses. Endocr Rev 1995; 16:460-84.
|
| [3] |
Ohzeki T, Kita H, Kunishige R, Hayashi T, Nishioka T. Giant adrenal pseudocyst removed using robot-assisted surgery. IJU Case Rep 2023; 6:141-3.
|
| [4] |
Thompson LH, Nordenstr?m E, Almquist M, Jacobsson H, Bergenfelz A. Risk factors for complications after adrenalectomy: results from a comprehensive national database. Langenbecks Arch Surg 2017; 402:315-22.
|
| [5] |
Teo XL, Lim SK. Robotic assisted adrenalectomy: is it ready for prime time? Investig Clin Urol 2016 ;57(Suppl 2):S130-46. https://doi.org/10.4111/icu.2016.57.S2.S130
doi: https://doi.org/10.4111/icu.2016.57.S2.S130
|
| [6] |
Ariyan C, Strong VE. The current status of laparoscopic adrenalectomy. Adv Surg 2007; 41:133-53.
|
| [7] |
Agcaoglu O, Aliyev S, Karabulut K, Mitchell J, Siperstein A, Berber E. Robotic versus laparoscopic resection of large adrenal tumors. Ann Surg Oncol 2012; 19:2288-94.
|
| [8] |
Simone G, Anceschi U, Tuderti G, Misuraca L, Celia A, De Concilio B, et al. Robot-assisted partial adrenalectomy for the treatment of Conn’s syndrome: surgical technique, and perioperative and functional outcomes. Eur Urol 2019; 75:811-6.
|
| [9] |
Anceschi U, Tuderti G, Fiori C, Zappalà O, Ferriero MC, Brassetti A, et al. Minimally invasive partial versus total adrenalectomy for the treatment of primary aldosteronism: results of a multicenter series according to the PASO criteria. Eur Urol Focus 2021; 7:1418-23.
|
| [10] |
Anceschi U, Mormando M, Fiori C, Zappalà O, De Concilio B, Brassetti A, et al. Surgical quality, antihypertensive therapy, and electrolyte balance: a novel trifecta to assess long-term outcomes of adrenal surgery for unilateral primary aldosteronism. J Clin Med 2022; 11:794. https://doi.org/10.3390/jcm11030794
doi: https://doi.org/10.3390/jcm11030794
|
| No related articles found! |
|
|
|
|