|
|
|
| Optimal interval for delayed retrieval surgery with reciprocating morcellators after enucleation of giant prostatic hyperplasia in holmium laser enucleation of the prostate |
Fumiyasu Endoa,*( ),Masaki Shimboa,Kenji Komatsua,Kazuhiro Ohwakib,Kazunori Hattoria ),Masaki Shimboa,Kenji Komatsua,Kazuhiro Ohwakib,Kazunori Hattoria
|
aDepartment of Urology, St. Luke’s International Hospital, 9-1 Akashi-cho, Chuo-ku, Tokyo, Japan
bDepartment of Hygiene and Public Health, Teikyo University School of Medicine Graduate School of Medicine, 2-11-1 Kaga, Itabashi-ku, Tokyo, Japan |
|
|
|
|
Abstract Objective: The aim of this research was to evaluate the efficiency of reciprocating morcellation for removing giant benign prostatic hyperplasia during holmium laser enucleation of the prostate, investigate whether performing morcellation as a two-stage procedure improves tissue retrieval efficiency, and seek to determine the optimal interval between the two surgeries. Methods: This study included nine cases of holmium laser enucleation of the prostate with an enucleated prostate weight exceeding 200 g, indicative of substantial prostate enlargement. Morcellation was performed on Day 0 (n=4), Day 4 (n=1), Day 6 (n=1), and Day 7 (n=3). The intervals were compared regarding the morcellation efficiency, beach ball presence, and pathology. Results: The mean estimated prostate volume was 383 (range 330-528) mL; the median enucleation weight was 252 (interquartile range [IQR] 222, 342) g; and the median enucleation time was 83 (IQR 62, 100) min. The mean morcellation efficiency was 1.44 (SD 0.55) g/min on Day 0 and 13.69 (SD 2.46) g/min on day 7. The morcellation efficiency was 4.15 g/min and 10.50 g/min on Day 4 and Day 6, respectively, with significantly higher in the two-stage group compared to one-stage group (11.0 g/min vs. 1.5 g/min; p=0.014). Efficiency was strongly correlated with intervals (p<0.001); the incidences of beach balls were 100% (4/4) and 60% (3/5) in the immediate and two-stage surgery groups, respectively. Conclusion: The efficiency of two-stage morcellation with reciprocating morcellators was highly related to the postoperative interval, with the maximum efficiency reached on Day 7.
|
|
Received: 27 November 2022
Available online: 20 July 2024
|
|
Corresponding Authors:
*E-mail address: endofum@luke.ac.jp (F. Endo).
|
|
|

| Parameter | One-stage surgery (n=4) | Two-stage surgery (n=5) | p-Value | | Age, year | 77.5 (73.5, 78.5) | 77.0 (72.0, 81.0) | 0.902 | | Body mass index, kg/m2 | 23.5 (23.0, 24.1) | 24.4 (24.2, 25.1) | 0.221 | | Estimated prostate volume, mean (range), mL | 373 (354-402) | 391 (330-528) | 1.000 | | Prostate-specific antigen, ng/mL | 12.5 (6.3, 19.7) | 8.2 (7.4, 9.7) | 0.807 | | Total operating time, min | 344 (266, 363) | 155 (132, 155) | 0.014 | | Enucleation time, min | 80 (52, 99) | 83 (74, 102) | 0.389 | | Enucleated weight, g | 228 (197, 255) | 252 (220, 361) | 0.462 | | Change in hemoglobin, g/dL | ?3.1 (?3.8, ?2.0) | ?2.3 (?3.6, ?1.1) | 0.462 | | Hypothermia (<34 °C), n (%) | 2 (50) | 0 (0) | 0.167 | | Continent recovery, mean (range), month | 2.5 (1-3) | 5.5 (1-15)a | 0.617 | | Hospital length of stay, day | 6.5 (5.0, 8.0) | 10 (9, 11) | 0.048 | | Morcellation efficiency, g/min | 1.5 (1.0, 1.9) | 11.0 (10.5, 14.4) | 0.014 |
|
|
Patients' background and surgical results.
|
|
|
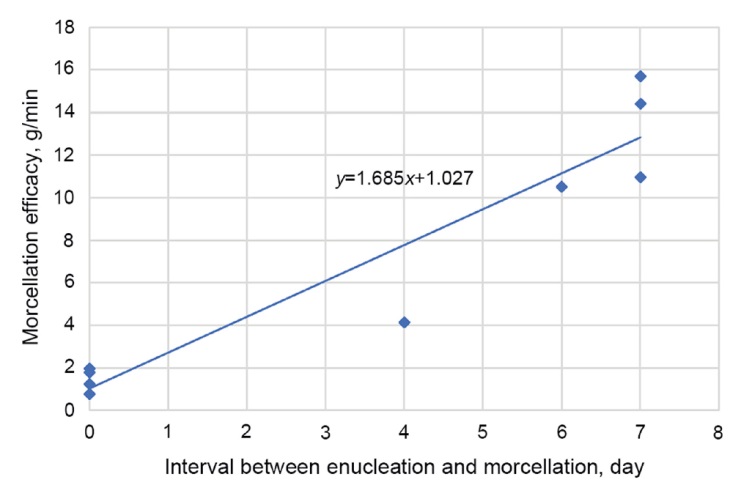
Relationship between morcellation efficiency and surgical interval. The morcellation efficiency was strongly correlated with the number of days. For case #2, data on the first morcellation were used for analysis.
|
| Case | Interval to morcellation, day | Enucleated weigh, g | Enucleation time, min | Enucleation efficiency, g/min | Morcellation time, min | Morcellation efficiency, g/min | Beach ball | | 1 | 0 | 222 | 100 | 2.22 | 180 | 1.23 | Present | | 2 | 0 | 171 | 62 | 5.52 | 226 | 0.76 | Present | | 7 | 171 | - | - | 14 | 12.21 | None | | 3 | 7 | 432 | 74 | 5.84 | 30 | 14.40 | None | | 4 | 7 | 220 | 102 | 2.16 | 14 | 15.71 | Present | | 5 | 4 | 361 | 62 | 5.82 | 87 | 4.15 | Present | | 6 | 0 | 234 | 98 | 2.39 | 131 | 1.79 | Present | | 7 | 7 | 252 | 104 | 2.42 | 23 | 10.96 | None | | 8 | 0 | 276 | 41 | 6.73 | 140 | 1.97 | Present | | 9 | 6 | 210 | 83 | 2.53 | 20 | 10.50 | Present |
|
|
Surgical parameters and the presence of beach balls.
|
|
|
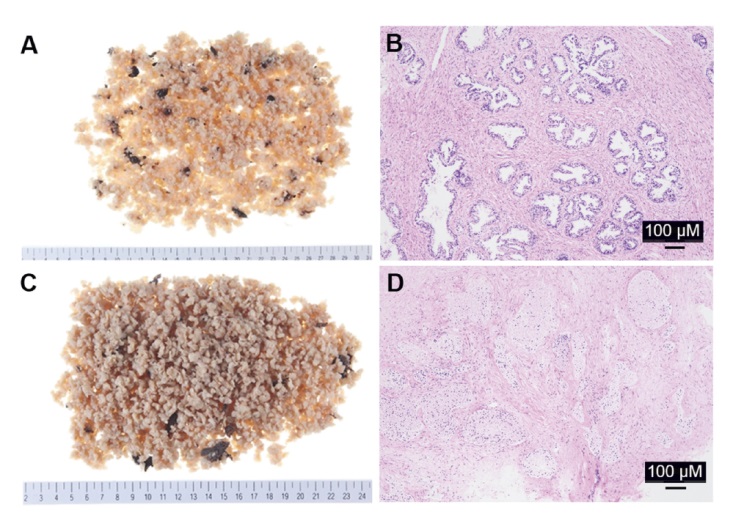
Pathological findings after surgery in case #2, in which surgery was interrupted due to hypothermia and two morcellation procedures were performed. (A and B) Immediately after surgery: gross appearance following fixation (A) and microscopic findings with hematoxylin and eosin staining (B); (C and D) Day 7 after surgery: gross appearance following fixation (C) and microscopic findings with hematoxylin and eosin staining (D). There was little change in appearance immediately and on Day 7, but microscopic findings showed that epithelial cells were degraded by necrosis in the delayed specimens.
|
| [1] |
Lerner LB, McVary KT, Barry MJ, Bixler BR, Dahm P, Das AK, et al. Management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA guideline part Idinitial work-up and medical management. J Urol 2021; 206:806-17.
|
| [2] |
Berry SJ, Coffey DS, Walsh PC, Ewing LL. The development of human benign prostatic hyperplasia with age. J Urol 1984; 132:474e9.
|
| [3] |
Zell MA, Abdul-Muhsin H, Navaratnam A, Cumsky J, Girardo M, Cornella J, et al. Holmium laser enucleation of the prostate for very large benign prostatic hyperplasia (≥200cc). World J Urol 2021; 39:129-34.
|
| [4] |
Franz J, Suarez-Ibarrola R, Pütz P, Sigle A, Lusuardi L, Netsch C, et al. Morcellation after endoscopic enucleation of the prostate: efficiency and safety of currently available devices. Eur Urol Focus 2022; 8:532-44.
|
| [5] |
McAdams S, Nunez-Nateras R, Martin CJ, Cha S, Humphreys MR. Morcellation efficiency in holmium laser enucleation of the prostate: oscillating morcellator outperforms reciprocating morcellator with no apparent learning curve. Urology 2017; 106:173e7.
|
| [6] |
Jun JH, Chung MH, Kim EM, Jun IJ, Kim JH, Hyeon JS, et al. Effect of pre-warming on perioperative hypothermia during holmium laser enucleation of the prostate under spinal anesthesia: a prospective randomized controlled trial. BMC Anesthesiol 2018; 18:201. https://doi.org/10.1186/s12871-018-0668-4
doi: https://doi.org/10.1186/s12871-018-0668-4
|
| [7] |
Elshal AM, Eldemerdash Y, Mekkawy R, Taha DE, Laymon M, El- Nahas AR, et al. Prostate tissue retrieval after holmium laser enucleation of the prostate; assessment of non-morcellation approaches. Arab J Urol 2016; 14:147-55.
|
| [8] |
Endo F, Shiga Y, Minagawa S, Iwabuchi T, Fujisaki A, Yashi M, et al. Anteroposterior dissection HoLEP: a modification to prevent transient stress urinary incontinence. Urology 2010; 76:1451e5.
|
| [9] |
Ishikawa R, Shitara T, Wakatabe Y, Kubo S, Hirayama T, Fujita T, et al. [Relationship between morcellation efficacy and enucleated tissue weight in holmium laser enucleation of the prostate (HoLEP) for patients with benign prostatic hyperplasia]. Nihon Hinyokika Gakkai Zasshi 2011; 102:675-8. [Article in Japanese].
|
| [10] |
Morishige S, Ohyama T, Fujita N, Kameda M, Yonekura Y, Endo F, et al. Risk factors for intraoperative hypothermia during holmium laser enucleation of the prostate. Urol Int 2023; 107:672e7.
|
| [11] |
Kawamura S, Takata K, Yoshida I, Matsui S. [A case of giant prostatic hypertrophy]. Hinyokika Kiyo 1984; 30:1861-6. [Article in Japanese].
|
| [12] |
Maliakal J, Mousa EE, Menon V. Giant prostatic hyperplasia: fourth largest prostate reported in medical literature. Sultan Qaboos Univ Med J 2014; 14:e253-6. PMID: 24790752.
|
| [13] |
Domínguez A, Gual J, Mu?oz-Rodríguez J, Abad C, Garcia- Rojo D, Hannaoui N, et al. Giant prostatic hyperplasia:case report of 3987 mL. Urology 2016; 88:e3e4.https://doi.org/10.1016/j.urology.2015.11.016
doi: https://doi.org/10.1016/j.urology.2015.11.016
|
| [14] |
Elzayat EA, Habib EI, Elhilali MM. Holmium laser enucleation of the prostate: a size-independent new "gold standard". Urology 2005; 66(Suppl. 5):108-13. https://doi.org/10.1016/j.urology.2005.06.006
doi: https://doi.org/10.1016/j.urology.2005.06.006
|
| [15] |
Gopee EL, Hong MK, Pham T. Holmium laser enucleation of the prostate in a 400 cc prostate: case report. J Endourol Case Rep 2016; 2:21e3.
|
| [16] |
Castellani D, Gasparri L, Faloia L, Veccia D, Giampieri M, Dellabella M. Fluid overload syndrome: a potentially lifethreatening complication of thulium laser enucleation of the prostate. Andrologia 2021; 53:e13807. https://doi.org/10.1111/and.13807
doi: https://doi.org/10.1111/and.13807
|
| [17] |
Ritter M, Krombach P, Bolenz C, Mrtinschek A, Bach T, Haecker A, et al. Standardized comparison of prostate morcellators using a new ex-vivo model. J Endourol 2012; 26:697-700.
|
| [18] |
Ohwaki K, Endo F, Shimbo M, Fujisaki A, Hattori K. Comorbidities as predictors of incidental prostate cancer after holmium laser enucleation of the prostate: diabetes and high-risk cancer. Aging Male 2017; 20:257-60.
|
| No related articles found! |
|
|
|
|