|
|
|
| Outcomes of surgical correction of Peyronie's disease with plaque excision and grafting: Comparison of testicular tunica vaginalis graft versus bovine pericardium graft |
Ali Eslahia,b,Faisal Ahmedc,*( ),Mohammad Reza Askarpoura,Hossein-Ali Nikbakhtd,Iman Shamohammadia,Payam Ghasemia,Hanieh Alimardania,Bahareh Ebrahimib ),Mohammad Reza Askarpoura,Hossein-Ali Nikbakhtd,Iman Shamohammadia,Payam Ghasemia,Hanieh Alimardania,Bahareh Ebrahimib
|
aDepartment of Urology, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran
bShiraz Geriatric Research Center, Shiraz University of Medical Sciences, Shiraz, Iran
cUrology Research Center, Al-Thora General Hospital, Department of Urology, School of Medicine, Ibb University of Medical Sciences, Ibb, Yemen
dSocial Determinants of Health Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran |
|
|
|
|
Abstract Objective: Peyronie's disease (PD) is an abnormal wound healing in the penile tunica albuginea. After fibrotic plaque excision, different graft materials have been used to repair the defects, but the optimal graft remains unknown. This study aimed to compare the functional outcomes of testicular tunica vaginalis grafts and bovine pericardium grafts in patients with severe PD. Methods: A retrospective comparative study was conducted on 33 PD patients undergoing partial plaque excision and grafting from September 2015 to May 2021. The patients were divided into two groups depending on the type of graft used. For 15 patients in Group B, testicular tunica vaginalis grafts were used to repair the defect, while for 18 patients in Group A, bovine pericardium grafts were used. Data of the patient's age, comorbidities, sexual function, penile curvature, postoperative complications, need for further treatment, change in penile length, and satisfaction were gathered and compared between the groups. Sexual function was evaluated using the 5-item version of the International Index of Erectile Function (IIEF-5), and a functional less than 20-degree penile curvature after surgery was considered a successful intervention. Results: There was no difference in age, comorbidities, degree of curvature, perioperative IIEF-5, operative time, plaque size, or complication rates. After surgery, a statistically significant improvement in curvature degree (p<0.05) and satisfactory penile appearance (p<0.05) were seen in both groups without any superiority between the two groups (p=0.423 and p=0.840, respectively). With a 30-month follow-up, the IIEF-5 was consistent in both groups, with no statistical significance between the groups (p=0.492). The main change in penile length during the operation was increased and still positive in the last follow-up in both groups without statistical significance (p=0.255 and p=0.101, respectively). Conclusion: Partial plaque excision and corporoplasty with both testicular tunica vaginalis or bovine pericardium grafts are equally effective in treating males with clinically significant PD.
|
|
Received: 05 October 2022
Available online: 20 July 2024
|
|
Corresponding Authors:
*E-mail address: fmaaa2006@yahoo.com (F. Ahmed).
|
|
|
|
|
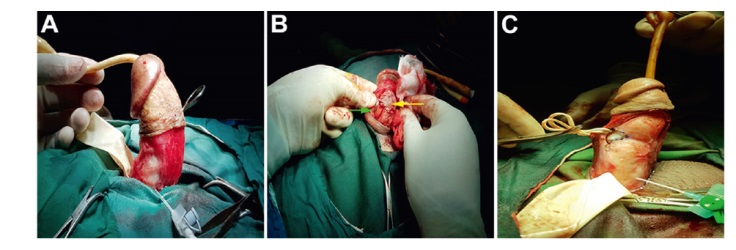
Intraoperative photos of pericardium bovina grafting. (A) Degloving the penis and degree of curvature; (B) Peyronie's plaque removal and grafting over the corpora cavernosa (yellow arrow), and dissection of the neurovascular bundle from the tunica albuginea (green arrow); (C) Penile appearance after curvature correction.
|
|
|
Intraoperative photos of testicular tunica vaginalis grafting. (A) Degloving the penis and degree of curvature; (B) Testicular tunica vaginalis dissection; (C) Penile appearance after curvature correction after Peyronie plaque removal, grafting over the corpora cavernosa and fixation (yellow arrow), and dissection of the neurovascular bundle from the tunica albuginea (green arrow).
|

| Variable | Group A (n=18) | Group B (n=15) | p-Value | | Agea, year | 56.00±10.00 | 56.00±9.65 | 1.000 | | Comorbidity, n (%) | | | 0.693 | | Diabetes mellitus | 7 (38.9) | 8 (53.3) | | | Hypertension | 2 (11.1) | 1 (6.7) | | | Using PDE5-Is, n (%) | 3 (16.7) | 2 (13.3) | 1.000 | | Plaque sizea, mm | 23.13±1.88 | 23.11±1.74 | 0.970 | | Change of penile length during operationa, mm | 21.05±5.57 | 23.46±6.36 | 0.255 |
|
|
Demographic characteristics and operative findings of the patients.
|
| Variable | Group A (n=18) | Group B (n=15) | MD (95% CI) | p-Value | | IIEF-5 | | | | | | Before surgerya | 17.44±0.70 | 17.46±0.74 | ?0.02 (?0.53 to 0.49) | 0.937 | | In the last follow-upa | 17.11±0.75 | 16.93±0.73 | 0.18 (?0.34 to 0.70) | 0.492 | | MD (95% CI) | 0.33 (?0.18 to 0.84) | 0.53 (?0.005 to 1.04) | | | | p-Value | 0.189 | 0.058 | | | | Degree of curvature | | | | | | Before surgerya | 53.33±6.18 | 54.33±8.42 | ?1.00 (?6.19 to 4.19) | 0.697 | | After surgerya | 1.39±0.50 | 1.53±0.51 | ?0.14 (?0.50 to 0.21) | 0.423 | | MD (95% CI) | 51.94 (48.93-54.95) | 52.80 (47.96-57.63) | | | | p-Value | <0.001 | <0.001 | | |
|
|
Comparison of the international index of erectile function and degree of curvature between pericardium graft and tunica vaginalis graft.
|
| Variable | Group A (n=18) | Group B (n=15) | p-Value | | Complication, n (%) | | | | | Hypoesthesia | 3 (16.7) | 3 (20.0) | 0.876 | | Infection | 1 (5.6) | 0 | | | Follow-up after surgerya, month | 31.11±10.93 | 35.60±8.32 | 0.202 | | Change of penile length in the last follow-upa, mm | 15.27±4.40 | 18.20±5.54 | 0.101 | | Using PDE5-Is in the last follow-up, n (%) | 5 (27.8) | 6 (40.0) | 0.458 | | Satisfactory resolution, n (%) | | | | | Very satisfied | 14 (77.8) | 13 (86.7) | 0.84 | | Equally satisfied | 4 (22.2) | 2 (13.3) | |
|
|
Postoperative complications, follow-up duration, change in penile length, and satisfaction in both groups.
|
| [1] |
El-Sakka AI, Salabas E, Din?er M, Kadioglu A. The pathophysiology of Peyronie’s disease. Arab J Urol 2013; 11:272-7.
|
| [2] |
Ostrowski KA, Gannon JR, Walsh TJ. A review of the epidemiology and treatment of Peyronie’s disease. Res Rep Urol 2016; 8:61-70.
|
| [3] |
Chen R, McCraw C, Lewis R. Plication proceduresdexcisional and incisional corporoplasty and imbrication for Peyronie’s disease. Transl Androl Urol 2016; 5:318-33.
|
| [4] |
Fiorillo A, Droghetti M, Palmisano F, Bianchi L, Piazza P, Sadini P, et al. Long-term outcomes after plaque incision and grafting for Peyronie’s disease: comparison of porcine dermal and bovine pericardium grafts. Andrology 2021; 9:269-76.
|
| [5] |
Ragheb A, Eraky A, Osmonov D. A decade of grafting techniques as a sole treatment for Peyronie’s disease. Andrology 2020; 8:1651-9.
|
| [6] |
Chung E. Penile reconstructive surgery in Peyronie disease: challenges in restoring normal penis size, shape, and function. World J Mens Health 2020; 38:1-8.
|
| [7] |
Fabiani A, Fioretti F, Pavia MP, Lepri L, Principi E, Servi L. Buccal mucosa graft in surgical management of Peyronie’s disease: ultrasound features and clinical outcomes. Arch Ital Urol Androl 2021; 93:107-10.
|
| [8] |
Liu B, Li Q, Cheng G, Song N, Gu M, Wang Z. Surgical treatment of Peyronie’s disease with autologous tunica vaginalis of testis. BMC Urol 2016; 16:1. https://doi.org/10.1186/s12894-016-0120-3
doi: https://doi.org/10.1186/s12894-016-0120-3
|
| [9] |
Das S. Peyronie’s disease: excision and autografting with tunica vaginalis. J Urol 1980; 124:818-9.
|
| [10] |
Yuanyuan M, Ning S, Yang W, Xiaoming Y, Lijie Z, Ninghan F. Testicular tunica vaginalis patch grafting for the treatment of Peyronie’s disease. Cell Biochem Biophys 2015; 71:1117-21.
|
| [11] |
Rico L, Villasante N, Blas L, Bonnano N, Ameri C. Initial experience in the treatment of Peyronie’s disease using testicular vaginal tunica graft. J Clin Urol 2021; 5:1-7.
|
| [12] |
Choi JB, Lee DS. Efficacy of H-shaped incision with bovine pericardial graft in Peyronie’s disease: a 1-year follow-up using penile Doppler ultrasonography. Int J Impot Res 2021; 33:541-7.
|
| [13] |
Hosseini J, Hosseini S, Hosseini MA, Rezaei Y. Pericardium in reconstructive urologic surgeries: a systematic review and meta-analysis. Urol Int 2019; 102:131-44.
|
| [14] |
Egydio PH, Lucon AM, Arap S. Treatment of Peyronie’s disease by incomplete circumferential incision of the tunica albuginea and plaque with bovine pericardium graft. Urology 2002; 59:570-4.
|
| [15] |
Chow AK, Sidelsky SA, Levine LA. Surgical outcomes of plaque excision and grafting and supplemental tunica albuginea plication for treatment of Peyronie’s disease with severe compound curvature. J Sex Med 2018; 15:1021-9.
|
| [16] |
Taylor FL, Abern MR, Levine LA. Predicting erectile dysfunction following surgical correction of Peyronie’s disease without inflatable penile prosthesis placement: vascular assessment and preoperative risk factors. J Sex Med 2012; 9:296-301.
|
| [17] |
Cormio L, Mancini V, Massenio P, d’Altilia N, Selvaggio O, Di Fino G, et al. Combined plaque incision, buccal mucosa grafting, and additional tunica albuginea plication for Peyronie’s disease. Sex Med 2019; 7:48-53.
|
| [18] |
Segal RL, Burnett AL. Surgical management for Peyronie’s disease. World J Mens Health 2013; 31:1-11.
|
| [19] |
Silva-Garretón A, Santillán D, Chávez D, Gioielli A, Rey- Valzacchi G, Layús O, et al. Satisfaction of patients with Peyronie’s disease after plaque surgery and bovine pericardium graft. Actas Urol Esp 2017; 41:103-8.
|
| [20] |
Ainayev Y, Zhanbyrbekuly U, Gaipov A, Kissamedenov N, Zhaparov U, Suleiman M, et al. Autologous testicular tunica vaginalis graft in Peyronie’s disease: a prospective evaluation. Int Urol Nephrol 2022; 54:1545-50.
|
| [21] |
Gundogdu G, Okhunov Z, Starek S, Veneri F, Orabi H, Holzman SA, et al. Evaluation of Bi-layer silk fibroin grafts for penile tunica albuginea repair in a rabbit corporoplasty model. Front Bioeng Biotechnol 2021; 9:791119. https://doi.org/10.3389/fbioe.2021.791119
doi: https://doi.org/10.3389/fbioe.2021.791119
|
| [22] |
Harper L, Michel JL, Sauvat F. Preliminary experience using a tunica vaginalis flap as the dorsal component of Bracka’s urethroplasty. BJU Int 2017; 119:470-3.
|
| [23] |
Helal MA, Lockhart JL, Sanford E, Persky L. Tunica vaginalis flap for the management of disabling Peyronie’s disease: surgical technique, results, and complications. Urology 1995; 46:390-2.
|
| [24] |
Thiel DD, Broderick GA, Wu KJ. Inclusion cyst and graft contraction in Tutoplast human cadeveric pericardium following Peyronie’s grafting: a previously unreported complication. Int J Impot Res 2005; 17:550-2.
|
| [25] |
Flores S, Choi J, Alex B, Mulhall JP. Erectile dysfunction after plaque incision and grafting: short-term assessment of incidence and predictors. J Sex Med 2011; 8:2031-7.
|
| [26] |
Chung E, Clendinning E, Lessard L, Brock G. Five-year followup of Peyronie’s graft surgery: outcomes and patient satisfaction. J Sex Med 2011; 8:594-600.
|
| [27] |
Kalsi J, Minhas S, Christopher N, Ralph D. The results of plaque incision and venous grafting (Lue procedure) to correct the penile deformity of Peyronie’s disease. BJU Int 2005; 95:1029-33.
|
| [28] |
Taylor FL, Levine LA. Surgical correction of Peyronie’s disease via tunica albuginea plication or partial plaque excision with pericardial graft: long-term follow up. J Sex Med 2008; 5:2221-30.
|
| [29] |
Rice PG, Somani BK, Rees RW. Twenty years of plaque incision and grafting for Peyronie’s disease: a review of literature. Sex Med 2019; 7:115-28.
|
| [30] |
Chierigo F, Bettocchi C, Campos-Juanatey F, Castiglione F, Kluth LA, Terrone C, et al. Use of grafting materials during penile prosthesis implantation in patients with Peyronie’s diseaseda systematic review. Int J Impot Res 2022; 34:534-42.
|
| [31] |
Sansalone S, Garaffa G, Djinovic R, Pecoraro S, Silvani M, Barbagli G, et al. Long-term results of the surgical treatment of Peyronie’s disease with Egydio’s technique: a European multicentre study. Asian J Androl 2011; 13:842-5.
|
| No related articles found! |
|
|
|
|