|
|
|
| Contemporary techniques and outcomes of surgery for locally advanced renal cell carcinoma with focus on inferior vena cava thrombectomy: The value of a multidisciplinary team |
Riccardo Campia,b,*( ),Paolo Barzaghia,a,Alessio Pecoraroa,Maria Lucia Galloa,Damiano Straccia,Alberto Mariottia,Saverio Giancanea,Simone Agostinic,Vincenzo Li Marzia,Arcangelo Sebastianellia,Pietro Spataforaa,Mauro Gaccia,Graziano Vignolinia,Francesco Sessaa,b,Paolo Muiesand,e,Sergio Sernia,b ),Paolo Barzaghia,a,Alessio Pecoraroa,Maria Lucia Galloa,Damiano Straccia,Alberto Mariottia,Saverio Giancanea,Simone Agostinic,Vincenzo Li Marzia,Arcangelo Sebastianellia,Pietro Spataforaa,Mauro Gaccia,Graziano Vignolinia,Francesco Sessaa,b,Paolo Muiesand,e,Sergio Sernia,b
|
aUnit of Urological Robotic Surgery and Renal Transplantation, University of Florence, Careggi Hospital, Florence, Italy
bDepartment of Experimental and Clinical Medicine, University of Florence, Florence, Italy
cDepartment of Radiology, Unit of Urogenital, Nephrological and Kidney Transplantation Imaging, Careggi Hospital, University of Florence, Florence, Italy
dHepatobiliary Unit, Department of Clinical and Experimental Medicine, University of Florence, AOU Careggi, Florence, Italy
eLiver Unit, Queen Elizabeth Hospital, Birmingham, UK |
|
|
|
|
Abstract Objective: To report the outcomes of surgery for a contemporary series of patients with locally advanced non-metastatic renal cell carcinoma (RCC) treated at a referral academic centre, focusing on technical nuances and on the value of a multidisciplinary team.
Methods: We queried our prospective institutional database to identify patients undergoing surgical treatment for locally advanced (cT3-T4 N0-1 M0) renal masses suspected of RCC at our centre between January 2017 and December 2020.
Results: Overall, 32 patients were included in the analytic cohort. Of these, 12 (37.5%) tumours were staged as cT3a, 8 (25.0%) as cT3b, 5 (15.6%) as cT3c, and 7 (21.9%) as cT4; 6 (18.8%) patients had preoperative evidence of lymph node involvement. Nine (28.1%) patients underwent nephron-sparing surgery while 23 (71.9%) received radical nephrectomy. A template-based lymphadenectomy was performed in 12 cases, with evidence of disease in 3 (25.0%) at definitive histopathological analysis. Four cases of RCC with level IV inferior vena cava thrombosis were successfully treated using liver transplant techniques without the need for extracorporeal circulation. While intraoperative complications were recorded in 3 (9.4%) patients, no postoperative major complications (Clavien-Dindo ≥3) were observed. At histopathological analysis, 2 (6.2%) patients who underwent partial nephrectomy harboured oncocytoma, while the most common malignant histotype was clear cell RCC (62.5%), with a median Leibovich score of 6 (interquartile range 5-7).
Conclusion: Locally advanced RCC is a complex and heterogenous disease posing several challenges to surgical teams. Our experience confirms that provided careful patient selection, surgery in experienced hands can achieve favourable perioperative, oncological, and functional outcomes.
|
|
Received: 03 February 2022
Available online: 20 July 2022
|
|
Corresponding Authors:
Riccardo Campi
E-mail: riccardo.campi@gmail.com
|
|
|
|
|
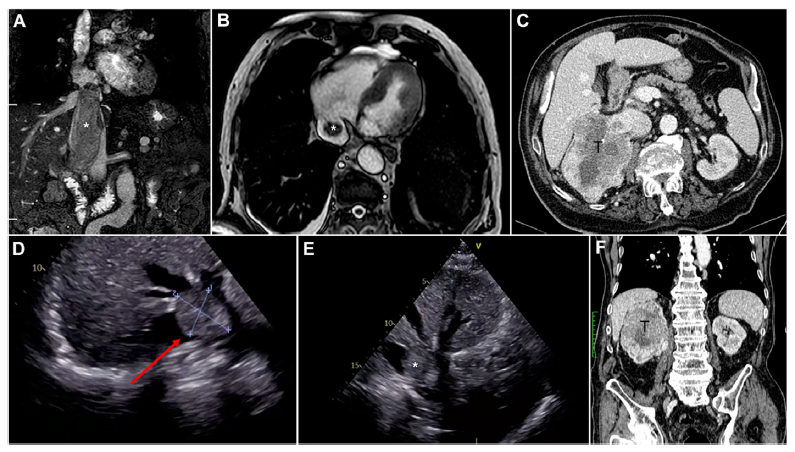
Overview of preoperative imaging techniques to diagnose, characterise, and stage locally-advanced RCC. (A and B) Coronal and axial magnetic resonance images showing a case of RCC with level IV IVC thrombosis; (C) Axial contrast-enhanced computed tomography images showing a right-sided RCC with level II IVC thrombosis; (D and E) Selected snapshots from preoperative trans-oesophageal echocardiography showing a case of RCC with level III IVC thrombosis; (F) Coronal contrast-enhanced computed tomography images showing a right-sided RCC with level II IVC thrombosis. RCC, renal cell carcinoma; IVC, inferior vena cava. T, tumour. Arrow, level III IVC thrombosis showed during trans-oesophageal echocardiography.? Thrombus.
|

|
|
Intraoperative snapshots showing the main steps of open surgery for locally advanced RCC. (A) Skin incision (modified Makuuchi incision) routinely performed at our institution for cases of RCC with suspected IVC thrombosis/infiltration, and/or suspected involvement of adjacent organs; (B) Overview of the operative field after placement of the Rochard retractor; (C) Intraoperative snapshot showing the final surgical result after radical nephrectomy with IVC thrombectomy and placement of a Gore-Tex prosthesis; (D) Exposure of a right-sided large RCC; (E) Exposure of the IVC and right renal loggia after retroperitoneal lymph node dissection; (F) Intraoperative snapshot showing the Pringle manoeuvre; (G) Intraoperative snapshot showing the operative field after left radical nephrectomy plus retroperitoneal lymph node dissection involving paraaortic and inter-aorto-caval templates. RCC, renal cell carcinoma; IVC, inferior vena cava.
|

|
|
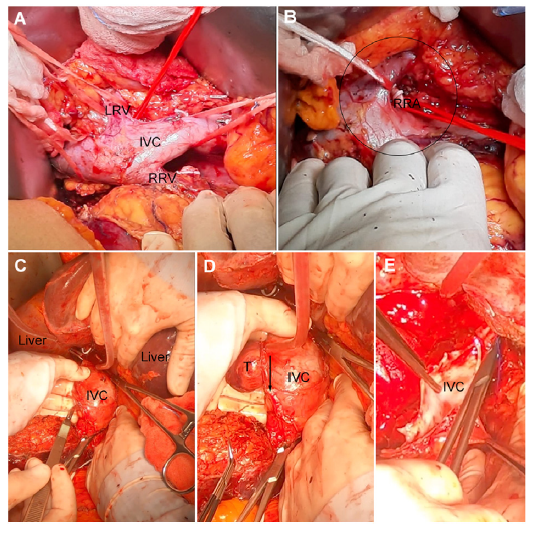
Technical nuances of radical nephrectomy and IVC thrombectomy for locally-advanced RCC. (A) Exposure and complete mobilisation of the IVC and left or right renal veins; (B) Intraoperative snapshot showing the early ligation of the right renal artery in the inter-aorto-caval space; (C, D and E) Step-by-step overview of IVC thrombectomy for a RCC with level III thrombus; (C) Cavotomy with cold knife; (D) Caudal extension of the cavotomy to progressively remove the tumour thrombus; (E) Closure of the IVC with running Prolene sutures. RCC, renal cell carcinoma; IVC, inferior vena cava; LRV, left renal vein; RRV, right renal vein; RRA, right renal artery; T, tumour. Arrow, the incision direction on inferior cava vein (venotomy). Circle, the renal hilum.
|
|
|
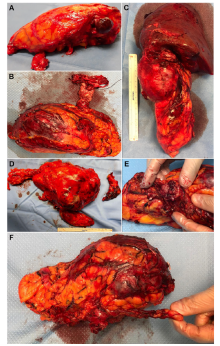
Postoperative pictures showing a variety of specimens after radical nephrectomy for locally-advanced RCC. (A and B) RCC with level II IVC thrombosis; (C) pT4 RCC infiltrating the liver (in this case, en-bloc radical nephrectomy plus liver segmentectomy was needed); (D) RCC with level III IVC thrombosis (in this case, radical nephrectomy plus adrenalectomy was performed for suspected metastasis of the right adrenal at preoperative imaging; final stage pT3c pM1); (E and F) RCC with level II IVC thrombosis. RCC, renal cell carcinoma; IVC, inferior vena cava.
|

| Characteristic | Value (n=32) | | Age, median (IQR), year | 68 (55-75) | | BMI, median (IQR), kg/m2 | 25.0 (23.5-26.0) | | Male, n (%) | 20 (62.5) | | Symptomatic patient at diagnosis, n (%) | 18 (56.2) | | Smoking exposure, n (%) | | No smoker | 15 (46.9) | | Current smoker | 10 (31.2) | | Former smoker | 7 (21.9) | | Diabetes mellitus, n (%) | 4 (12.5) | | ASA physical status classification, median (IQR) | 2 (2-3) | | CCI (age-adjusted), median (IQR) | 2 (1-3) | | Previous abdominal surgery, n (%) | 17 (53.1) | | Preoperative hemoglobin, median (IQR), g/dL | 13.4 (11.5-14.7) | | Preoperative creatinine, median (IQR), mg/dL | 1.0 (0.9-1.1) | | Preoperative eGFR (CKD-EPI), median (IQR), mL/min/1.73 m2 | 72.0 (58.0-89.0) | | Kidney side, n (%) | | Right | 18 (56.3) | | Left | 13 (40.6) | | Bilateral | 1 (3.1) | | Tumour diameter at preoperative imaging, median (IQR), cm | 8 (5-10) | | PADUA score | | Overall score, median (IQR) | 11 (9-12) | | Risk groups, n (%) | | Low (6-7) | 1 (3.1) | | Intermediate (8-9) | 11 (34.4) | | High (≥10) | 20 (62.5) | | SPARE score | | Overall score, media (IQR) | 7 (4-8) | | Risk groups, n (%) | | Low (0-3) | 4 (12.5) | | Intermediate (4-7) | 19 (59.4) | | High (≥8) | 9 (28.1) | | Clinical T stage, n (%) | | T3a | 12 (37.5) | | T3b | 8 (25.0) | | T3c | 5 (15.6) | | T4 | 7 (21.9) | | Clinical N stage, n (%) | | N0 | 26 (81.2) | | N1 | 6 (18.8) |
|
|
Preoperative baseline patients' and tumours' characteristics.
|
| Characteristic | Value | | Operative time, median (IQR), min | 185 (150-210) | | Type of surgery, n (%) | | Partial nephrectomy | 9 (28.1) | | Radical nephrectomy | 23 (71.9) | | Surgical approach, n (%) | | Open | 13 (40.6) | | Robot-assisted | 19 (59.4) | | Warm ischaemia timea, median (IQR), min | 18 (14-22) | | Lymph nodes dissection, n (%) | 12 (37.5) | | Hilar dissection | 2 (6.2) | | Periaortic dissection | 2 (6.2) | | Hilar, pericaval and periaortic dissection | 6 (18.8) | | Iliac and pericaval dissection | 1 (3.1) | | Iliac and hilar dissection | 1 (3.1) | | Ipsilateral adrenalectomy, n (%) | 4 (12.5) | | Metastasis dissection, n (%) | 1 (3.1) | | Intraoperative adverse incident classification, n (%) | | Grade 0 | 0 (0) | | Grade 1b | 3 (9.4) | | Grade 2 | 0 (0) | | Grade 3 | 0 (0) | | Grade 4 | 0 (0) | | Grade 5 | 0 (0) |
|
|
Intraoperative outcomes in patients undergoing surgery for locally-advanced renal cell carcinoma in our series.
|
| Characteristic | Value | | Early postoperative outcome | | Overall length of hospitalization, median (IQR), day | 4 (4-6) | | Length of stay in ICU, median (IQR), day | 0 (0-1) | | Patients with postoperative complications, n (%) | 14 (43.8) | | Hemoglobin, median (IQR), g/dL | | POD 1 | 11.6 (10.3-13.2) | | POD 3 | 10.9 (9.8-12.0) | | eGFR (CKD-EPI), median (IQR), mL/min/1.73 m2 | | POD 1 | 55.8 (41.5-74.5) | | POD 3 | 52.3 (42.3-68.7) | | At discharge | 55.8 (42.3-82.5) | | Highest grade postoperative surgical complicationa, n (%) | | Grade 0 | 18 (56.2) | | Grade 1 | 3 (9.4) | | Grade 2 | | Overall | 11 (34.4) | | Transfusions | 5 (15.6) | | Grade 3a | 0 (0) | | Grade 3b | 0 (0) | | Grade 4a | 0 (0) | | Grade 4b | 0 (0) | | Grade 5 | 0 (0) | | Comprehensive complication index, median (IQR) | 0.0 (0.0-20.9) | | Histopathology outcome | | Benign histology, n (%) | 2 (6.2) | | Histological subtypes, n (%) | | Clear RCC | 20 (62.5) | | Papillary RCC | 5 (15.6) | | Chromophobe RCC | 3 (9.4) | | Other malignant tumour | 2 (6.2) | | Benign tumour | 2 (6.2) | | ISUP grade ≥3 (n=26)b, n (%) | 21 (80.8) | | Pathological T stage (n=28)b, n (%) | | T1a | 0 (0) | | T1b | 2 (7.1) | | T2a | 3 (10.7) | | T2b | 0 (0) | | T3a | 14 (50.0) | | T3b | 8 (28.6) | | T3c | 1 (3.6) | | T4 | 0 (0) | | pN stage (n=12)b, n (%) | | N0 | 9 (75.0) | | N1 | 3 (25.0) | | pM1 stage (n=30)b,c, n (%) | 1 (3.3) | | Diameter of the tumour at pathologic evaluation, median (IQR), cm | 7 (5-10) | | Leibovich score (n=20 clear cell RCC)d | | Overall score, median (IQR) | 6 (5-7) | | Risk groupsc | | Low (0-2) | 3 (15.0) | | Intermediate (3-5) | 5 (25.0) | | High (≥6) | 12 (60.0) |
|
|
Postoperative outcomes and histopathologic results in patients undergoing surgery for locally-advanced RCC in our series.
|
| Characteristic | Value | | Follow-up, median (IQR), month | 24 (18-37) | | Cancer related death at last follow-up, n (%) | 2 (6.2) | | Hospital re-admission (at least one episode) after renal surgery, n (%)a | | Surgery for another urologic tumour | 1 (3.3) | | Surgery for RCC recurrence | 1 (3.3) | | Other causes not related to surgery/recurrence | 6 (20.0) | | Patients with recurrence at last follow-up, n (%)a | | Recurrence in the ipsilateral remanent kidney after partial nephrectomy | 1 (3.3) | | Recurrence in ipsilateral renal fossa and lymph nodes | 1 (3.3) | | Multiple recurrence in intra-abdominal soft tissues or organs | 4 (13.3) | | Distant recurrence | 2 (6.7) | | Treatment of recurrence (n=8), n (%) | | Palliative treatment | 1 (12.5) | | Surgery | 1 (12.5) | | Systemic therapy | 4 (50.0) | | Multiple treatment | 2 (25.0) | | eGFR at last follow-up (CKD-EPI), median (IQR), mL/min/1.73 m2 | 57.0 (46.0-69.0) |
|
|
Follow-up data in patients undergoing surgery for locally-advanced RCC in our series.
|
| [1] |
Ferlay J, Colombet M, Soerjomataram I, Dyba T, Randi G, Bettio M, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries and 25 major cancers in 2018. Eur J Cancer 2018; 103:356e87.
doi: S0959-8049(18)30955-9
pmid: 30100160
|
| [2] |
Capitanio U, Bensalah K, Bex A, Boorjian SA, Bray F, Coleman J, et al. Epidemiology of renal cell carcinoma. Eur Urol 2019; 75:74e84.
doi: S0302-2838(18)30633-X
pmid: 30243799
|
| [3] |
Levi F, Ferlay J, Galeone C, Lucchini F, Negri E, Boyle P, et al. The changing pattern of kidney cancer incidence and mortality in Europe. BJU Int 2008; 101:949e58.
doi: 10.1111/j.1464-410X.2008.07451.x
|
| [4] |
Ljungberg B, Albiges L, Bedke J, Bex A, Capitanio U, Gile RH, et al. European Association of Urology (EAU) Guidelines on renal cell carcinoma. Arnhem, The Netherlands: EAU Guidelines Office; 2022. Available at: https://uroweb.org/guideline/renal-cell-carcinoma/#1. , version 2022. [Accessed 28 February 2022].
|
| [5] |
Campbell SC, Clark PE, Chang SS, Karam JA, Souter L, Uzzo RG. Renal mass and localized renal cancer: evaluation, management, and follow-up: AUA guideline: Part I. J Urol 2021; 206:199e208.
|
| [6] |
Bex A, van Thienen JV, Schrier M, Graafland N, Kuusk T, Hendricksen K, et al. A Phase II, single-arm trial of neoadjuvant axitinib plus avelumab in patients with localized renal cell carcinoma who are at high risk of relapse after nephrectomy (NEOAVAX). Future Oncol 2019; 15: 2203e9.
|
| [7] |
Borregales LD, Adibi M, Thomas AZ, Wood CG, Karam JA. The role of neoadjuvant therapy in the management of locally advanced renal cell carcinoma. Ther Adv Urol 2016; 8:130e41.
doi: 10.1177/1756287215612962
|
| [8] |
Choueiri TK, Tomczak P, Park SH, Venugopal B, Ferguson T, Chang YH, et al. Adjuvant pembrolizumab after nephrectomy in renal-cell carcinoma. N Engl J Med 2021; 385:683e94.
doi: 10.1056/NEJMoa2106391
|
| [9] |
Campi R, Tellini R, Sessa F, Mari A, Cocci A, Greco F, et al. Techniques and outcomes of minimally-invasive surgery for nonmetastatic renal cell carcinoma with inferior vena cava thrombosis: a systematic review of the literature. Minerva Urol Nefrol 2019; 71:339e58.
|
| [10] |
Blute ML, Leibovich BC, Lohse CM, Cheville JC, Zincke H. The Mayo Clinic experience with surgical management, complications and outcome for patients with renal cell carcinoma and venous tumour thrombus. BJU Int 2004; 94:33e41.
doi: 10.1111/j.1464-410X.2004.04897.x
|
| [11] |
Nesbitt JC, Soltero ER, Dinney CP, Walsh GL, Schrump DS, Swanson DA, et al. Surgical management of renal cell carcinoma with inferior vena cava tumour thrombus. Ann Thorac Surg 1997; 63:1592e600.
pmid: 9205155
|
| [12] |
Lardas M, Stewart F, Scrimgeour D, Hofmann F, Marconi L, Dabestani S, et al. Systematic review of surgical management of nonmetastatic renal cell carcinoma with vena caval thrombus. Eur Urol 2016; 70:265e80.
doi: 10.1016/j.eururo.2015.11.034
|
| [13] |
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro 3rd AF, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med 2009; 150:604e12.
doi: 10.7326/0003-4819-150-9-200905050-00006
|
| [14] |
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chron Dis 1987; 40:373e83.
doi: 10.1016/0021-9681(87)90171-8
|
| [15] |
Daabiss M. American Society of Anaesthesiologists physical status classification. Indian J Anaesth 2011; 55:111e5.
doi: 10.4103/0019-5049.79879
|
| [16] |
Biyani CS, Pecanka J, Roupreˆt M, Jensen JB, Mitropoulos D. Intraoperative adverse incident classification (EAUiaiC) by the European Association of Urology ad hoc complications guidelines Panel. Eur Urol 2020; 77:601e10.
doi: 10.1016/j.eururo.2019.11.015
|
| [17] |
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a newproposalwith evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004; 240:205e13.
doi: 10.1097/01.sla.0000133083.54934.ae
|
| [18] |
Slankamenac K, Graf R, Barkun J, Puhan MA, Clavien PA. The comprehensive complication index: a novel continuous scale to measure surgical morbidity. Ann Surg 2013; 258:1e7.
doi: 10.1097/SLA.0b013e318296c732
pmid: 23728278
|
| [19] |
Sobin LH, Gospodarowicz MK, Wittekind C. TNM classification of malignant tumours. 7th ed. Chichester, West Sussex, UK: Wiley-Blackwell; 2009. p. 255e7.
|
| [20] |
Delahunt B, Cheville JC, Martignoni G, Humphrey PA, Magi-Galluzzi C, McKenney J, et al. The International Society of Urological Pathology (ISUP) grading system for renal cell carcinoma and other prognostic parameters. Am J Surg Pathol 2013; 37:1490e504.
doi: 10.1097/PAS.0b013e318299f0fb
pmid: 24025520
|
| [21] |
Leibovich BC, Blute ML, Cheville JC, Lohse CM, Frank I, Kwon ED, et al. Prediction of progression after radical nephrectomy for patients with clear cell renal cell carcinoma: a stratification tool for prospective clinical trials. Cancer 2003; 97:1663e71.
pmid: 12655523
|
| [22] |
Ficarra V, Novara G, Secco S, Macchi V, Porzionato A, De Caro R, et al. Preoperative aspects and dimensions used for an anatomical (PADUA) classification of renal tumours in patients who are candidates for nephron-sparing surgery. Eur Urol 2009; 56:786e93.
doi: 10.1016/j.eururo.2009.07.040
|
| [23] |
Ficarra V, Porpiglia F, Crestani A, Minervini A, Antonelli A, Longo N, et al. The Simplified PADUA REnal (SPARE) nephrometry system: a novel classification of parenchymal renal tumours suitable for partial nephrectomy. BJU Int 2019. https://doi.org/10.1111/bju.14772.
|
| [24] |
Winters DA, Soukup T, Sevdalis N, Green JSA, Lamb BW. The cancer multidisciplinary team meeting: in need of change? History, challenges and future perspectives. BJU Int 2021; 128:271e9.
|
| [25] |
Klatte T, Ficarra V, Gratzke C, Kaouk J, Kutikov A, Macchi V, et al. A literature review of renal surgical anatomy and surgical strategies for partial nephrectomy. Eur Urol 2015; 68: 980e92.
doi: 10.1016/j.eururo.2015.04.010
|
| [26] |
Campi R, Sessa F, Di Maida F, Greco I, Mari A, Taká_cová T, et al. Templates of lymph node dissection for renal cell carcinoma: a systematic review of the literature. Front Surg 2018; 5:76. https://doi.org/10.3389/fsurg.2018.00076.
doi: 10.3389/fsurg.2018.00076
|
| [27] |
Ciancio G, Hawke C, Soloway M. The use of liver transplant techniques to aid in the surgical management of urological tumors. J Urol 2000; 164:665e72.
doi: 10.1097/00005392-200009010-00012
pmid: 10953122
|
| [28] |
Ciancio G, Livingstone AS, Soloway M. Surgical management of renal cell carcinoma with tumor thrombus in the renal and inferior vena cava: the University of Miami experience in using liver transplantation techniques. Eur Urol 2007; 51:988e95.
doi: 10.1016/j.eururo.2006.11.055
|
| [29] |
Ciancio G, Vaidya A, Savoie M, Soloway M. Management of renal cell carcinoma with level III thrombus in the inferior vena cava. J Urol 2002; 168:1374e7.
doi: 10.1016/S0022-5347(05)64452-7
|
| [30] |
CiancioG, Gonzalez J, Shirodkar SP, Angulo JC, Soloway MS. Liver transplantation techniques for the surgical management of renal cell carcinoma with tumor thrombus in the inferior vena cava: step-by-step description. Eur Urol 2011; 59(3):401e6.
doi: 10.1016/j.eururo.2010.07.028
|
| [31] |
Ciancio G, Soloway MS. Renal cell carcinoma with tumor thrombus extending above diaphragm: avoiding cardiopulmonary bypass. Urology 2005; 66:266e70.
doi: 10.1016/j.urology.2005.03.039
|
| [32] |
Cerwinka WH, Ciancio G, Salerno TA, Soloway MS. Renal cell cancer with invasive atrial tumor thrombus excised off-pump. Urology 2005; 66:1319. https://doi.org/10.1016/j.urology.2005.06.098.
|
| [33] |
Swierzewski DJ, Swierzewski MJ, Libertino JA. Radical nephrectomy in patients with renal cell carcinoma with venous, vena caval, and atrial extension. Am J Surg 1994; 168:205e9.
pmid: 8053528
|
| [34] |
Skinner DG, Pritchett TR, Lieskovsky G, Boyd SD, Stiles QR. Vena caval involvement by renal cell carcinoma. Surgical resection provides meaningful long-term survival. Ann Surg 1989; 210:387e94.
pmid: 2774709
|
| [35] |
Mueller-Lisse UG, Mueller-Lisse UL. Imaging of advanced renal cell carcinoma. World J Urol 2010; 28:253e61.
doi: 10.1007/s00345-010-0557-z
pmid: 20458484
|
| [36] |
Vuong NS, Ferriere JM, Michiels C, Calen L, Tesi L, Capon G, et al. Robot-assisted versus open surgery for radical nephrectomy with level 1-2 vena cava tumor thrombectomy: a French monocenter experience (UroCCR study #73). Minerva Urol Nephrol 2021; 73:498e508.
|
| [37] |
Wang B, Huang Q, Liu K, Fan Y, Peng C, Gu L, et al. Robot-assisted level III-IV inferior vena cava thrombectomy: initial series with step-by-step procedures and 1-yr outcomes. Eur Urol 2020; 78:77e86.
doi: 10.1016/j.eururo.2019.04.019
|
| [38] |
Capitanio U, Suardi N, Matloob R, Roscigno M, Abdollah F, Di Trapani E, et al. Extent of lymph node dissection at nephrectomy affects cancer-specific survival and metastatic progression in specific sub-categories of patients with renal cell carcinoma (RCC). BJU Int 2014; 114:210e5.
doi: 10.1111/bju.12508
pmid: 24854206
|
| [39] |
Capitanio U, Leibovich BC. The rationale and the role of lymph node dissection in renal cell carcinoma. World J Urol 2017; 35: 497e506.
doi: 10.1007/s00345-016-1886-3
pmid: 27364520
|
| [40] |
Bhindi B, Wallis CJD, Boorjian SA, Thompson RH, Farrell A, Kim SP, et al. The role of lymph node dissection in the management of renal cell carcinoma: a systematic review and meta-analysis. BJU Int 2018; 121:684e98.
doi: 10.1111/bju.14127
pmid: 29319926
|
| [41] |
Karmali RJ, Suami H, Wood CG, Karam JA. Lymphatic drainage in renal cell carcinoma: back to the basics. BJU Int 2014; 114: 806e17.
doi: 10.1111/bju.12814
pmid: 24841690
|
| [42] |
Moschini M, Dell’Oglio P, Larcher A, Capitanio U. Lymph node dissection for renal cell carcinoma: what are we missing? Curr Opin Urol 2016; 26:424e31.
doi: 10.1097/MOU.0000000000000312
pmid: 27262140
|
| [1] |
Michele Marchioni,Daniele Amparore,Igino Andrea Magli,Riccardo Bertolo,Umberto Carbonara,Selcuk Erdem,Alexandre Ingels,Constantijn H.J. Muselaers,Onder Kara,Marco Mascitti,Tobias Klatte,Maximilian Kriegmair,Nicola Pavan,Eduard Roussel,Angela Pecoraro,Laura Marandino,Riccardo Campi,Luigi Schips,on behalf of the European Association of Urology (EAU) Young Academic Urologists (YAU) Renal Cancer group . Potential benefit of lymph node dissection during radical nephrectomy for kidney cancer: A review and critical analysis of current literature[J]. Asian Journal of Urology, 2022, 9(3): 215-226. |
| [2] |
Umberto Carbonara,Daniele Amparore,Cosimo Gentile,Riccardo Bertolo,Selcuk Erdem,Alexandre Ingels,Michele Marchioni,Constantijn H.J. Muselaers,Onder Kara,Laura Marandino,Nicola Pavan,Eduard Roussel,Angela Pecoraro,Fabio Crocerossa,Giuseppe Torre,Riccardo Campi,Pasquale Ditonno. Current strategies to diagnose and manage positive surgical margins and local recurrence after partial nephrectomy[J]. Asian Journal of Urology, 2022, 9(3): 227-242. |
| [3] |
Daniele Amparore,Angela Pecoraro,Federico Piramide,Paolo Verri,Enrico Checcucci,Sabrina De Cillis,Alberto Piana,Mariano Burgio,Michele Di Dio,Matteo Manfredi,Cristian Fiori,Francesco Porpiglia. Three-dimensional imaging reconstruction of the kidney's anatomy for a tailored minimally invasive partial nephrectomy: A pilot study[J]. Asian Journal of Urology, 2022, 9(3): 263-271. |
| [4] |
Reza Alaghehbandan,Christopher G. Przybycin,Virginie Verkarre,Rohit Mehra. Chromophobe renal cell carcinoma: Novel molecular insights and clinicopathologic updates[J]. Asian Journal of Urology, 2022, 9(1): 1-11. |
| [5] |
Yucong Zhang,Gongwei Long,Haojie Shang,Beichen Ding,Guoliang Sun,Wei Ouyang,Man Liu,Yuan Chen,Heng Li,Hua Xu,Zhangqun Ye. Comparison of the oncological, perioperative and functional outcomes of partial nephrectomy versus radical nephrectomy for clinical T1b renal cell carcinoma: A systematic review and meta-analysis of retrospective studies[J]. Asian Journal of Urology, 2021, 8(1): 117-125. |
| [6] |
Kulthe Ramesh Seetharam Bhat,Marcio Covas Moschovas,Fikret Fatih Onol,Travis Rogers,Shannon Roof,Vipul R. Patel,Oscar Schatloff. Robotic renal and adrenal oncologic surgery: A contemporary review[J]. Asian Journal of Urology, 2021, 8(1): 89-99. |
| [7] |
Paula Andrea Peña,Lynda Torres-Castellanos,Germán Patiño,Stefanía Prada,Luis Gabriel Villarraga,Nicolás Fernández. Minimally invasive nephrectomy for inflammatory renal disease[J]. Asian Journal of Urology, 2020, 7(4): 345-350. |
| [8] |
Michael C. Phung,Andrew R. Rouse,Jayce Pangilinan,Robert C. Bell,Erika R. Bracamonte,Sharfuddeen Mashi,Arthur F. Gmitro,Benjamin R. Lee. Investigation of confocal microscopy for differentiation of renal cell carcinoma versus benign tissue. Can an optical biopsy be performed?[J]. Asian Journal of Urology, 2020, 7(4): 363-368. |
| [9] |
Yoichiro Tohi,Shiori Murata,Noriyuki Makita,Issei Suzuki,Masashi Kubota,Yoshio Sugino,Koji Inoue,Hiroyuki Ueda,Mutsushi Kawakita. Absence of asymptomatic unruptured renal artery pseudoaneurysm on contrast-enhanced computed tomography after robot-assisted partial nephrectomy without parenchymal renorrhaphy[J]. Asian Journal of Urology, 2020, 7(1): 24-28. |
| [10] |
Dean Laganosky,Christopher P. Filson,Dattatraya Patil,Viraj A. Master. Survival benefit with extended lymphadenectomy for advanced renal malignancy: A population-based analysis[J]. Asian Journal of Urology, 2020, 7(1): 29-36. |
| [11] |
Guangju Ge,Zhenghui Wang,Mingchao Wang,Gonghui Li,Zuhao Xu,Yukun Wang,Shawpong Wan. Inadvertent insertion of nephrostomy tube into the renal vein following percutaneous nephrolithotomy: A case report and literature review[J]. Asian Journal of Urology, 2020, 7(1): 64-67. |
| [12] |
Ned Kinnear,Lina Hua,Bridget Heijkoop,Derek Hennessey,Daniel Spernat. The impact of intra-operative cell salvage during open nephrectomy[J]. Asian Journal of Urology, 2019, 6(4): 346-352. |
| [13] |
Ling Xie,Yifen Zhang,Chin-Lee Wu. Microphthalmia family of transcription factors associated renal cell carcinoma[J]. Asian Journal of Urology, 2019, 6(4): 312-320. |
| [14] |
Arun Ramdas Menon,T.P. Rajeev,Suresh Nivedita,Suraj Hegde. Mixed epithelial and stromal tumour with extension to vesicoureteric junction[J]. Asian Journal of Urology, 2019, 6(3): 302-304. |
| [15] |
Fangyuan Zhang,Gang Zhao,Pengjie Wu,Qi An,Yang Yang,Xin Chen,Jianye Wang,Dong Wei. Asynchronous abdominal wall and sigmoid metastases in clear cell renal cell carcinoma: A case report and literature review[J]. Asian Journal of Urology, 2019, 6(2): 210-214. |
|
|
|
|