|
|
|
| Boswellia resin extract and propolis derived polyphenols in patients with type III chronic prostatitis/chronic pelvic pain syndrome: An Italian prospective multicenter study |
Fabrizio Presiccea,*( ),Francesco Barresea,Andrea Cantianib,Alessio Filianotia,Domenico Tuzzoloc,Paolo Di Palmad,Stefano Laurettie,Stefano Brunorif,Marco Martinia ),Francesco Barresea,Andrea Cantianib,Alessio Filianotia,Domenico Tuzzoloc,Paolo Di Palmad,Stefano Laurettie,Stefano Brunorif,Marco Martinia
|
a San Filippo Neri Hospital, Department of Urology, Rome, Italy
b Sant’Eugenio Hospital, Department of Urology, Rome, Italy
c Casa del Sole Clinic, Department of Urology, Formia, Italy
d Fabrizio Spaziani Hospital, Department of Urology, Frosinone, Italy
e Santa Caterina della Rosa Clinic, Department of Urology, Rome, Italy
f Villa Stuart Clinic, Department of Urology, Rome, Italy |
|
|
|
|
Abstract Objective: To assess the efficacy and safety of a treatment regimen based on rectal administration of Boswellia resin extract and propolis derived polyphenols in patients with type IIIa and type IIIb chronic prostatitis and chronic pelvic pain syndrome (CP/CPPS). Methods: Patients with type IIIa and type IIIb CP/CPPS received one rectal suppository a day for 15 days per month for 3 consecutive months. Participants were evaluated with National Institutes of Health-Chronic Prostatitis Symptom Index (NIH-CPSI), the International Prostate Symptom Scores (IPSS), International Index of Erectile Function (IIEF), four-glass test, uroflowmetry, and prostate-specific antigen assessments at baseline and at Week 4, and Week 12. Primary endpoints were improvement in pain domain of NIH-CPSI and improvement of NIH-CPSI total score. Secondary outcomes included improvement of micturition and quality of life (QoL) domains of NIH-CPSI questionnaire. Results: A total of 61 males were enrolled. No adverse events were reported. Significant improvements from baseline to Day 30 were reported for NIH-CPSI total score (mean difference: -9.2; p<0.01), NIH-CPSI pain domain (mean difference: -5.5; p<0.01), NIH-CPSI micturition domain, NIH-CPSI QoL domain, and IPSS total score (mean difference: -5.6; p<0.01). No significant changes from baseline in terms of IIEF score or maximum flow rate were observed. At final follow-up (Day 90), further significant improvements in terms of NIH-CPSI total score (mean difference: -12.2; p<0.01), NIH-CPSI pain domain (mean difference: -6.6; p<0.01), NIH-CPSI micturition domain, NIH-CPSI QoL domain, and IPSS total score were reported. Conclusion: Rectal administration of Boswellia resin extract and propolis derived polyphenols is well tolerated and delivers a significant symptomatic improvement in most patients with type IIIa and type IIIb CP/CPPS.
|
|
Received: 11 December 2020
Available online: 20 April 2022
|
|
Corresponding Authors:
Fabrizio Presicce
E-mail: fabriziopresicce@libero.it
|
|
|

| Variable | Overall (n=61) | IIIaa (n=31) | IIIbb (n=30) | | Agec, year | 61.0 (52.5-64.0) | 59.0 (45.0-63.0) | 61.0 (53.7-66.5) | | PSAc, ng/mL | 2.9 (1.6-3.5) | 2.9 (1.1-3.9) | 2.5 (1.6-3.2) | | IPSS totalc, year | 18.0 (12.0-23.5) | 22.0 (18.0-25.0) | 15.5 (11.7-20.0) | | Voiding | 5.0 (3.0-6.0) | 5.0 (4.0-6.0) | 4.0 (3.0-7.0) | | Storage | 12.0 (8.0-16.5) | 15.0 (12.0-20.0) | 11.0 (8.0-14.0) | | IIEF scorec | 18.0 (15.0-21.0) | 19.0 (17.0-22.0) | 15.5 (12.0-20.0) | | NIH-CPSI total scorec | 21.0 (18.0-24.0) | 23.0 (21.0-29.0) | 19.5 (18.0-21.0) | | Pain | 9.0 (8.0-10.0) | 10.0 (8.0-12.0) | 9.0 (8.0-10.0) | | Micturition | 5.0 (4.0-6.0) | 6.0 (5.0-7.0) | 4.0 (2.7-6.0) | | Quality of life | 7.0 (5.0-9.0) | 9.0 (6.0-10.0) | 6.0 (5.0-7.0) | | Prostate volumec, mL | 44.0 (33.0-48.5) | 40.0 (33.0-47.0) | 45.0 (33.0-56.2) | | Leukocytes in VB3cd | 20.0 (8.0-25.0) | 33.0 (12.0-45.0) | 8.0 (7.0-8.0) | | Residual urine volumec, mL | 30.0 (5.0-50.0) | 30.0 (20.0-45.0) | 25.0 (0-50.0) | | Maximum flow ratec, mL/s | 14.0 (11.2-18.0) | 12.0 (10.0-14.2) | 16.0 (14.0-19.0) | | Mean flow ratec, mL/s | 8.8 (7.0-10.0) | 8.9 (7.0-9.6) | 8.5 (7.0-10.0) |
|
|
Characteristics of the enrolled population at baseline.
|
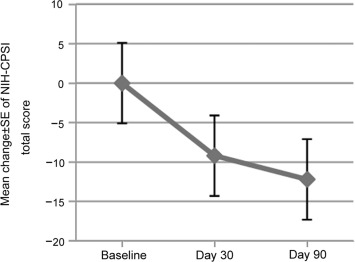
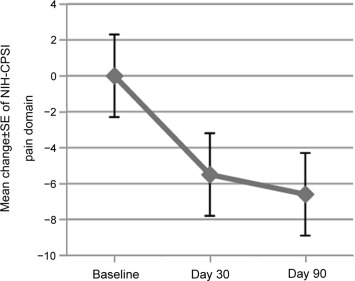
| Variable | Mean value at Day 30 (percentage of change from baseline) | Mean change±SE at Day 30 | Mean value at Day 90 (percentage of change from baseline) | Mean change±SE at Day 90 | | PSA, ng/mL | Not evaluated | Not evaluated | 2.3 (-20.7) | -0.6±0.9 | | IPSS total score | 12.4 (-31.1) | -5.6±5.9 | 10.1 (-43.9) | -7.9±6.5 | | IIEF score | 18.5 (2.8) | 0.5±1.5 | 18.9 (5.0) | 0.9±2.1 | | NIH-CPSI total score | 11.8 (-43.8) | -9.2±5.1 | 8.8 (58.1) | -12.2±6.3 | | Pain | 3.5 (-61.1) | -5.5±2.3 | 2.4 (-73.3) | -6.6±2.6 | | Micturition | 3.5 (-30.0) | -1.5±1.7 | 2.8 (-44.0) | -2.2±2.3 | | Quality of life | 5 (-28.6) | -2.0±2.2 | 3.8 (-45.7) | -3.2±2.7 | | Leukocytes in VB3a | Not evaluated | Not evaluated | 4.1 (-79.5) | -15.9±4.5 | | Maximum flow rate, mL/s | 15 (7.1) | 1.0±2.2 | 15.3 (9.2) | 1.3±2.3 |
|
|
Clinical evolution after treatment in the enrolled population.
|
|
|
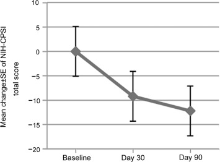
Mean change ±SE from baseline in NIH-CPSI total score at Day 30 and Day 90 of treatment, respectively. NIH-CPSI, National Institutes of Health-Chronic Prostatitis Symptom Index; SE, standard error.
|
|
|
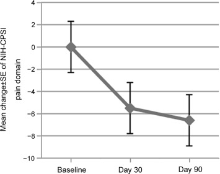
Mean change ±SE from baseline in NIH-CPSI pain domain at Day 30 and Day 90 of treatment, respectively. NIH-CPSI, National Institutes of Health-Chronic Prostatitis Symptom Index; SE, standard error.
|
|
|
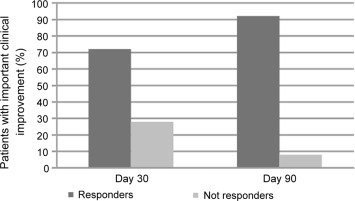
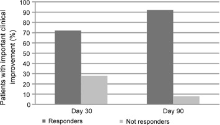
Patients with important clinical improvement (decrease of 25% or 6 points in National Institutes of Health-Chronic Prostatitis Symptom Index total score) at Day 30 and Day 90 of treatment, respectively.
|
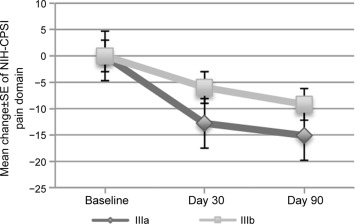
| Variable | Mean value at Day 30 (percentage of change from baseline) | Mean change±SE at Day 30 | Mean value at Day 90 (percentage of change from baseline) | Mean change±SE at Day 90 | | IIIa | IIIb | IIIa | IIIb | IIIa | IIIb | IIIa | IIIb | | PSA, ng/mL | Not evaluated | Not evaluated | Not evaluated | Not evaluated | 2.2 (-24.1) | 2.1 (-16.0) | -0.7±0.9 | -0.4±1.0 | | IPSS total score | 12.1 (-45.1) | 13.6 (-12.2) | -9.9±6.0 | -1.9±2.3 | 10.2 (-53.6) | 11.3 (-27.1) | -11.8±7.1 | -4.2±2.4 | | IIEF | 20.2 (6.3) | 15.6 (0.6) | 1.2±1.2 | 0.1±1.6 | 20.6 (8.4) | 15.6 (0.6) | 1.6±1.8 | 0.1±2.1 | | NIH-CPSI total score | 10.2 (-55.6) | 13.5 (-30.8) | -12.8±4.6 | -6.0±3.0 | 7.9 (-65,6) | 10.3 (-47.2) | -15.1±7.0 | -9.2±3.7 | | Pain | 4.5 (-55.0) | 5.7 (-36.7) | -5.5±2.3 | -3.3±2.0 | 3.4 (-66.0) | 4.6 (-48.9) | -6.6±2.1 | -4.4±2.2 | | Micturition | 3.4 (-43.3) | 3.4 (-15.1) | -2.6±1.7 | -0.6±1.0 | 2.5 (-58.3) | 3.1 (-22.5) | -3.5±2.5 | -0.9±1.1 | | Quality of life | 5.5 (-38.9) | 5.2 (-13.3) | -3.5±2.0 | -0.8±1.4 | 4.5 (-50.0) | 4.0 (-33.3) | -4.5±2.9 | -2.0±1.6 | | Leukocytes in VB3a | Not evaluated | Not evaluated | Not evaluated | Not evaluated | 6.8 (-79.4) | 3.0 (-62.5) | -26.2±5.2 | -5.0±2.3 | | Maximum flow rate, mL/s | 13.5 (12.5) | 16.5 (3.1) | 1.5±3.0 | 0.5±0.9 | 14.1 (17.5) | 16.6 (3.8) | 2.1±2.9 | 0.6±1.1 |
|
|
Clinical evolution after treatment in the enrolled population according the category of type III CP/CPPS.
|
|
|
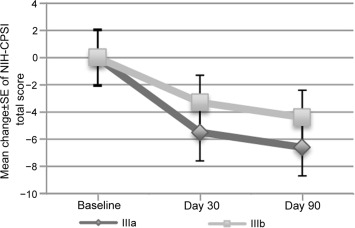
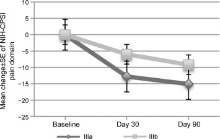
Mean change±SE from baseline in NIH-CPSI total score at Day 30 and Day 90 of treatment in patients with type IIIa and type IIIb chronic prostatitis/chronic pelvic pain syndrome, respectively. NIH-CPSI, National Institutes of Health-Chronic Prostatitis Symptom Index; SE, standard error.
|
|
|
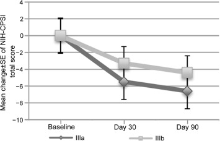
Mean change±SE from baseline in NIH-CPSI pain domain at Day 30 and Day 90 of treatment in patients with type IIIa and type IIIb chronic prostatitis/chronic pelvic pain syndrome. NIH-CPSI, National Institutes of Health-Chronic Prostatitis Symptom Index; SE, standard error.
|
| [1] |
Collins MM, Stafford RS, O’Leary MP, Barry MJ. How common is prostatitis? A national survey of physician visits. J Urol 1998; 159:1224-8.
pmid: 9507840
|
| [2] |
McNaughton Collins M, Meigs JB, Barry MJ, Walker Corkery E, Giovannucci E, Kawachi I. Prevalence and correlates of prostatitis in the health professionals follow-up study cohort. J Urol 2002; 167:1363-6.
pmid: 11832733
|
| [3] |
Suskind AM, Berry SH, Ewing BA, Elliott MN, Suttorp MJ, Clemens JQ. The prevalence and overlap of interstitial cystitis/ bladder pain syndrome and chronic prostatitis/chronic pelvic pain syndrome in men: Results of the RAND Interstitial Cystitis Epidemiology male study. J Urol 2013; 189:141-5.
doi: 10.1016/j.juro.2012.08.088
pmid: 23164386
|
| [4] |
Nickel JC, Nyberg LM, Hennenfent M. Research guidelines for chronic prostatitis: Consensus report from the First National Institutes of Health International Prostatitis Collaborative Network. Urology 1999; 54:229-33.
|
| [5] |
Wenninger K, Heiman JR, Rothman I, Berghuis JP, Berger RE. Sickness impact of chronic nonbacterial prostatitis and its correlates. J Urol 1996; 155:965-8.
pmid: 8583619
|
| [6] |
Morgia G, Mucciardi G, Galì A, Madonia M, Marchese F, Di Benedetto A, et al. Treatment of chronic prostatitis/chronic pelvic pain syndrome category IIIA with Serenoa repens plus selenium and lycopene (Profluss) versus S. repens alone: An Italian randomized multicenter-controlled study. Urol Int 2010; 84:400-6.
doi: 10.1159/000302716
pmid: 20332612
|
| [7] |
Franco JV, Turk T, Jung JH, Xiao YT, Iakhno S, Tirapegui FI, et al. Pharmacological interventions for treating chronic prostatitis/ chronic pelvic pain syndrome. Cochrane Database Syst Rev 2019; 10:CD012552. https://doi.org/10.1002/14651858.CD012552.pub2.
|
| [8] |
Litwin MS, McNaughton-Collins M, Fowler Jr FJ, Nickel JC, Calhoun EA, Pontari MA, et al. The National Institutes of Health chronic prostatitis symptom index: Development and validation of a new outcome measure. Chronic Prostatitis Collaborative Research Network. J Urol 1999; 162:369-75.
doi: 10.1016/s0022-5347(05)68562-x
pmid: 10411041
|
| [9] |
Togni S, Maramaldi G, Di Pierro F, Biondi M. A cosmeceutical formulation based on Boswellic acids for the treatment of erythematous eczema and psoriasis. Clin Cosmet Invest Dermatol 2014; 11:321-7.
doi: 10.2147/CCID.S160923
|
| [10] |
Abdel-Tawab M, Werz O, Schubert-Zsilavecz M. Boswellia serrata: An overall assessment of in vitro, preclinical, pharmacokinetic and clinical data. Clin Pharmacokinet 2011; 50:349-69.
doi: 10.2165/11586800-000000000-00000
pmid: 21553931
|
| [11] |
Ichikawa H, Satoh K, Tobe T, Yasuda I, Ushio F, Matsumoto K, et al. Free radical scavenging activity of propolis. Redox Rep 2002; 7:47-50.
doi: 10.1179/135100002125000181
|
| [12] |
Sibona M, Destefanis P, Agnello M, Lillaz B, Giuliano M, Cai T, et al. The association of Boswellia resin extract and propolis derived polyphenols can improve quality of life in patients affected by prostatitis-like symptoms. Arch Ital Urol Androl 2020; 91:251-5.
doi: 10.4081/aiua.2019.4.251
|
| [13] |
Galeone G, Spadavecchia R, Balducci MT, Pagliarulo V. [The role of Proxelan in the treatment of chronic prostatitis. Results of a randomized trial]. Minerva Urol Nefrol 2012; 64: 135-41. [Article in Italian].
pmid: 22617307
|
| [14] |
Di Vico T, Durante J, Polito C, Tognarelli A, Canale D, Caglieresi C, et al. Pumpkin seeds, Centella asiatica, Boswellia, Helichrysum, acetate vitamin E, Melaleuca alternifolia and hyaluronic acid phytocomplex monotherapy effects in patients with chronic pelvic pain syndrome. Minerva Urol Nefrol 2020; 72:236-42.
|
| [15] |
Propert KJ, Alexander RB, Nickel JC, Kusek JW, Litwin MS, Landis JR, et al. Chronic Prostatitis Collaborative Research Network. Design of a multicenter randomized clinical trial for chronic prostatitis/chronic pelvic pain syndrome. Urology 2002; 59:870-6.
doi: 10.1016/S0090-4295(02)01601-1
|
| [16] |
Nickel JC, Pontari M, Moon T, Gittelman M, Malek G, Farrington J, et al; Rofecoxib Prostatitis Investigator Team. A randomized, placebo controlled, multicenter study to evaluate the safety and efficacy of rofecoxib in the treatment of chronic nonbacterial prostatitis. J Urol 2003; 169: 1401-5.
doi: 10.1097/01.ju.0000054983.45096.16
|
| [17] |
Propert KJ, Litwin MS, Wang Y, Alexander RB, Calhoun E, Nickel JC, et al. Responsiveness of the national Institutes of health chronic prostatitis symptom index (NIH-CPSI). Qual Life Res 2006; 15:299-305.
pmid: 16468084
|
| [18] |
Wagenlehner FM, Schneider H, Ludwig M, Schnitker J, Bra¨hler E, Weidner W. A pollen extract (Cernilton) in patients with inflammatory chronic prostatitis-chronic pelvic pain syndrome: A multicentre, randomised, prospective, doubleblind, placebo-controlled phase 3 study. Eur Urol 2009; 56: 544-51.
doi: 10.1016/j.eururo.2009.05.046
pmid: 19524353
|
| [19] |
Pirozzi L, Sountoulides P, Castellan P, Presicce F, Lombardo R, Romero M, et al. Current pharmacological treatment for male LUTS due to BPH: Dutasteride or finasteride? Curr Drug Targets 2015; 16:1165-71.
doi: 10.2174/1389450116666150518101617
|
| [20] |
Morgia G, Russo GI, Urzì D, Privitera S, Castelli T, Favilla V, et al. A phase II, randomized, single-blinded, placebocontrolled clinical trial on the efficacy of Curcumina and Calendula suppositories for the treatment of patients with chronic prostatitis/chronic pelvic pain syndrome type III. Arch Ital Urol Androl 2017; 89:110-3.
doi: 10.4081/aiua.2017.2.110
|
| [21] |
Park SJ, Yoon HN, Shim BS. Prevention of relapse with the cranberry juice in chronic pelvic pain syndrome. Korean J Urol 2005; 46:63-7.
|
| [22] |
Shoskes DA, Zeitlin SI, Shahed A, Rajfer J. Quercetin in men with category III chronic prostatitis: A preliminary prospective, double-blind, placebo-controlled trial. Urology 1999; 54:960-3.
pmid: 10604689
|
| [23] |
Elist J. Effects of pollen extract preparation Prostat/Poltit on lower urinary tract symptoms in patients with chronic nonbacterial prostatitis/chronic pelvic pain syndrome: A randomized, double-blind, placebo-controlled study. Urology 2006; 67:60-3.
|
| [1] |
Liang G. Qu,Gregory Jack,Marlon Perera,Melanie Evans,Sue Evans,Damien Bolton,Nathan Papa. Impact of delay from transperineal biopsy to radical prostatectomy upon objective measures of cancer control[J]. Asian Journal of Urology, 2022, 9(2): 170-176. |
| [2] |
Braulio Omar Manzo,Jose David Cabrera,Esteban Emiliani,Hector Manuel Sánchez,Brian Howard Eisner,Jose Ernesto Torres. Impact of the adherence to medical treatment on the main urinary metabolic disorders in patients with kidney stones[J]. Asian Journal of Urology, 2021, 8(3): 275-279. |
| [3] |
Liang Dong,Richard C. Zieren,Wei Xue,Theo M. de Reijke,Kenneth J. Pienta. Metastatic prostate cancer remains incurable, why?[J]. Asian Journal of Urology, 2019, 6(1): 26-41. |
| [4] |
Allert M.de Vries*,John P.F.A.Heesakkers. Contemporary diagnostics and treatment options for female stress urinary incontinence[J]. Asian Journal of Urology, 2018, 5(3): 141-148. |
| [5] |
Darab Mehraban. Clinical value of intravesical prostatic protrusion in the evaluation and management of prostatic and other lower urinary tract diseases[J]. Asian Journal of Urology, 2017, 4(3): 174-180. |
| [6] |
Johan Braeckman, Louis Denis. Management of BPH then 2000 and now 2016-From BPH to BPO[J]. Asian Journal of Urology, 2017, 4(3): 138-147. |
| [7] |
Thomas Y. Hsueh, Allen W. Chiu. Narrow band imaging for bladder cancer[J]. Asian Journal of Urology, 2016, 3(3): 126-129. |
| [8] |
Kaiwen Li, Tianxin Lin, Chinese Bladder Cancer Consortium, Wei Xue, Xin Mu, Enci Xu, Xu Yang, Fubao Chen, Guangyong Li, Lulin Ma, Guoliang Wang, Chaozhao Liang, Haoqiang Shi, Ming Li, Mao Tang, Xueyi Xue, Yisong Lv, Yaoliang Deng, Chengyang Li, Zhiwen Chen, Xiaozhou Zhou, Fengshuo Jin, Xudong Liu, Jinxin Wei, Lei Shi, Xin Gou, Weiyang He, Liqun Zhou, Lin Cai, Liping Xie, Guanghou Fu, Xiangbo Kong, Hongyan Sun, Ye Tian, Lang Feng, Tiejun Pan, Yiyi Wu, Dongwen Wang, Hailong Hao, Benkang Shi, Yaofeng Zhu, Qiang Wei, Ping Han, Changli Wu, Dawei Tian, Zhangqun Ye, Zheng Liu, Zhiping Wang, Junqiang Tian, Lin Qi, Minfeng Chen, Wei Li, Jinchun Qi, Gongxian Wang, Longlong Fu, Zhaolin Sun, Guangheng Luo, Zhoujun Shen, Zhaowei Zhu, Jinchun Xing, Zhun Wu, Dong Wei, Xin Chen, Yanqun Na, Hongfeng Guo, Chunxi Wang, Zhihua Lu, Chuize Kong, Yang Liu, Jin Yang, Jianyun Hu, Xin Gao, Jielin Li, Changjun Yin, Pu Li, Shan Chen, Zhen Du, Jiongming Li, Yongji Yan, Xu Zhang, Shuang Huang, Fangjian Zhou, Zhiling Zhang, Yinghao Sun, Shuxiong Zeng, Song Cen, Jiaquan Zhou, Hanzhong Li, Jin Wen, Jian Huang. Current status of diagnosis and treatment of bladder cancer in China-Analyses of Chinese Bladder Cancer Consortium Database[J]. Asian Journal of Urology, 2015, 2(2): 63-69. |
|
|
|
|