|
|
|
| Validation of Vesical Imaging Reporting and Data System score for the diagnosis of muscle-invasive bladder cancer: A prospective cross-sectional study |
Kumawat Ghanshyam,Vyas Nachiket,Sharma Govind,Priyadarshi Shivam,Gupta Bhagwan Sahay,Singla Mohit( ),Kumar Ashok ),Kumar Ashok
|
| Department of Urology, Sawai Man Singh Medical College and Hospital, Jaipur, Rajasthan, India |
|
|
|
|
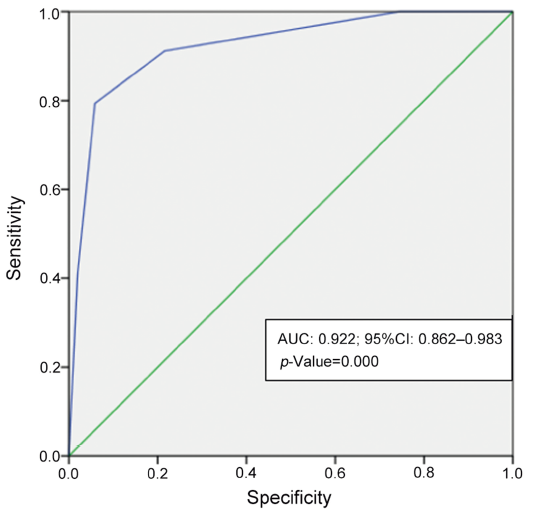
Abstract Objective: Vesical Imaging Reporting and Data System (VIRADS) score was developed to standardize the reporting and staging of bladder tumors on pre-operative multiparametric magnetic resonance imaging. It helps in avoiding unnecessary repeat transurethral resection of bladder tumor in high-risk non-muscle-invasive bladder cancer patients. This study was done to determine the validity of VIRADS score prospectively for the diagnosis of muscle-invasive bladder cancer. Methods: This study was conducted from March 2019 to March 2020 at Sawai Man Singh Medical College and Hospital, Jaipur, Rajasthan, India. Patients admitted with the provisional diagnosis of bladder tumor were included as participants. All these patients underwent a 3 Tesla mpMRI to obtain a VIRADS score before they underwent transurethral resection of bladder tumor and these data were analyzed to evaluate the correlation of pre-operative VIRADS score with muscle invasiveness of the tumor in final biopsy report. Results: A cut-off of VIRADS ≥4 for prediction of detrusor muscle invasion yielded a sensitivity of 79.4%, specificity of 94.2%, positive predictive value of 90.0%, negative predictive value of 87.5%, and diagnostic accuracy of 86.4%. A cut off of VIRADS ≥3 for prediction of detrusor muscle invasion yielded a sensitivity of 91.2%, specificity of 78.8%, positive predictive value of 73.8%, negative predictive value of 93.2%, and accuracy of 83.7%. The receiver operating curve showed the area under the curve to be 0.922 (95% confidence interval: 0.862-0.983). Conclusion: VIRADS score appears to be an excellent and effective pre-operative radiological tool for the prediction of detrusor muscle invasion in bladder cancer.
|
|
Received: 23 May 2020
Available online: 20 October 2022
|
|
Corresponding Authors:
Singla Mohit
E-mail: singlahome@gmail.com
|
|
|

|
|
Protocol of the study. MRI, magnetic resonance imaging; TURBT, transurethral resection of bladder tumor; TUR, transurethral resection; TCC, transitional cell carcinoma; VIRADS, Vesical Imaging Reporting and Data System; Cis, carcinoma in situ; HPE, histopathological examination; Re-TURBT, repeat TURBT.
|

| VIRADS score | Likelihood of muscle invasion | | 1 | High unlikely muscle-invasive tumor and <1 cm in size. | | 2 | Unlikely to be a muscle-invasive tumor | | 3 | Equivocal, there is no clear-cut evidence of muscle invasion | | 4 | Likely detrusor invasion but no extravesical extension | | 5 | High likely tumor invading detrusor with extension into extravesical fat |
|
|
Interpretation of VIRADS score.
|
| Patients, characteristic | Value | VIRADS 1 | VIRADS 2 | VIRADS 3 | VIRADS 4 | VIRADS 5 | | Sex, n (%) | | Male | 67 (77.91) | 10 (11.63) | 24 (27.91) | 10 (11.63) | 12 (13.95) | 11 (12.79) | | Female | 19 (22.09) | 4 (4.65) | 6 (6.98) | 2 (2.33) | 3 (3.49) | 4 (4.65) | | Diameter of tumor, n (%) | | ≤3 cm | 47 (54.65) | 14 (16.28) | 23 (26.74) | 5 (5.81) | 3 (3.49) | 2 (2.33) | | >3 cm | 39 (45.35) | 0 | 7 (8.14) | 7 (8.14) | 12 (13.95) | 13 (15.12) | | Grade of tumor, n (%) | | High | 48 (55.81) | 1 (1.16) | 10 (11.63) | 8 (9.30) | 14 (16.28) | 15 (17.44) | | Low | 38 (44.19) | 13 (15.12) | 20 (23.26) | 4 (4.65) | 1 (1.16) | 0 (0) | | Non muscle invasive, n (%) | 52 (60.47) | 14 (16.28) | 27 (31.40) | 8 (9.3) | 2 (2.32) | 1 (1.16) | | Muscle invasive, n (%) | 34 (39.53) | 0 | 3 (3.49) | 4 (4.65) | 13 (15.12) | 14 (16.28) |
|
|
Results of the present study.
|

|
|
The receiver operating curve. AUC, area under curve; CI, confidence interval.
|

|
|
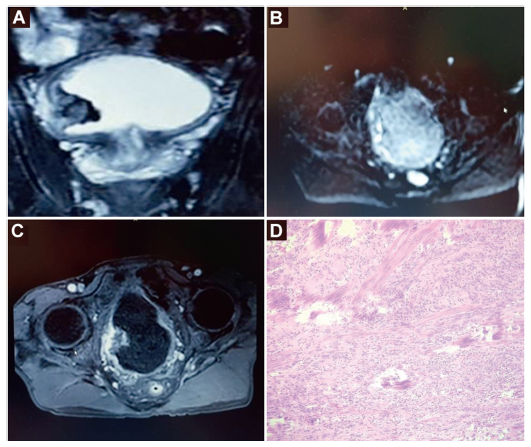
mpMRI images of different sequences and HPE picture of a case of VIRADS 4 (in a 64-year-old male patient with right posterior-lateral urinary bladder wall mass). (A) T2WI (axial) showing a tumor with intermediate signal intensity arising from the right postero-lateral bladder wall; (B) DWI (b=1000 s/mm2) showing the tumor as having hyperintense signal intensity with an irregular outline; (C) DCEI showing tumor enhancement with contrast; (D) HPE (100×) after TURBT showing high grade transitional cell carcinoma infiltrating the muscularis propria of the urinary bladder. DCEI, dynamic contrast-enhanced image; DWI, diffusion weighted image; T2WI, T2 weighted image; TURBT, transurethral resection of bladder tumor; VIRADS, Vesical Imaging Reporting and Data System; mpMRI, multiparametric magnetic resonance imaging; HPE, histopathological examination.
|
| [1] |
Svatek RS, Hollenbeck BK, Holm?ng S, Lee R, Kim SP, Stenzl A, et al. The economics of bladder cancer: costs and considerations of caring for this disease. Eur Urol 2014; 66:253e62.
|
| [2] |
Antoni S, Ferlay J, Soerjomataram I, Znaor A, Jemal A, Bray F. Bladder cancer incidence and mortality: a global overview and recent trends. Eur Urol 2017; 71:96e108.
|
| [3] |
Leow JJ, Cole AP, Seisen T, Bellmunt J, Mossanen M, Menon M, et al. Variations in the costs of radical cystectomy for bladder cancer in the USA. Eur Urol 2018; 73:374e82.
|
| [4] |
Soukup V, _Capoun O, Cohen D, Hernández V, Babjuk M, Burger M, et al. Prognostic performance and reproducibility of the 1973 and 2004/2016 World Health Organization grading classification systems in non-muscle-invasive bladder cancer: a European Association of Urology non-muscle invasive bladder cancer guidelines panel systematic review. Eur Urol 2017; 72:801e13.
|
| [5] |
Linton KD, Rosario DJ, Thomas F, Rubin N, Goepel JR, Abbod MF, et al. Disease specific mortality in patients with low risk bladder cancer and the impact of cystoscopic surveillance. J Urol 2013; 189:828e33.
|
| [6] |
Josephson D, Pasin E, Stein JP. Superficial bladder cancer: part 2. Management. Expert Rev Anticancer Ther 2007; 7:567e81.
|
| [7] |
Sherif A, Jonsson MN, Wiklund NP. Treatment of muscleinvasive bladder cancer. Expert Rev Anticancer Ther 2007; 7: 1279e83.
|
| [8] |
Kulkarni GS, Hakenberg OW, Gschwend JE, Thalmann G, Kassouf W, Kamat A, et al. An updated critical analysis of the treatment strategy for newly diagnosed high-grade T1 (previously T1G3) bladder cancer. Eur Urol 2010; 57:60e70.
|
| [9] |
Gordon PC, Thomas F, Noon AP, Rosario DJ, Catto JWF. Longterm outcomes from re-resection for high-risk non-muscleinvasive bladder cancer: a potential to rationalize use. Eur Urol Focus 2019; 5:650e7.
|
| [10] |
Ark JT, Keegan KA, Barocas DA, Morgan TM, Resnick MJ, You C, et al. Incidence and predictors of understaging in patients with clinical T1 urothelial carcinoma undergoing radical cystectomy. BJU Int 2014; 113:894e9.
|
| [11] |
Brausi M, Collette L, Kurth K, van der Meijden AP, Oosterlinck W, Witjes JA, et al; EORTC Genito-Urinary Tract Cancer Collaborative Group. Variability in the recurrence rate at first follow-up cystoscopy after TUR in stage Ta T1 transitional cell carcinoma of the bladder: a combined analysis of seven EORTC studies. Eur Urol 2002; 41:523e31.
|
| [12] |
Tritschler S, Mosler C, Straub J, Buchner A, Karl A, Graser A, et al. Staging of muscle-invasive bladder cancer: can computerized tomography help us to decide on local treatment. World J Urol 2012; 30:827e31.
|
| [13] |
Paner GP, Montironi R, Amin MB. Challenges in pathologic staging of bladder cancer: proposals for fresh approaches of assessing pathologic stage in light of recent studies and observations pertaining to bladder histoanatomic variances. Adv Anat Pathol 2017; 24:113e27.
|
| [14] |
Woo S, Suh CH, Kim SY, Cho JY, Kim SH. Diagnostic performance of MRI for prediction of muscle-invasiveness of bladder cancer: a systematic review and meta-analysis. Eur J Radiol 2017; 95:46e55.
|
| [15] |
Huang L, Kong Q, Liu Z, Wang J, Kang Z, Zhu Y. The diagnostic value of MR imaging in differentiating T staging of bladder cancer: a meta-analysis. Radiology 2018; 286:502e11.
|
| [16] |
Panebianco V, Narumi Y, Altun E, Bochner BH, Efstathiou JA, Hafeez S, et al. Multiparametric magnetic resonance imaging for bladder cancer: development of VI-RADS (Vesical Imaging- Reporting and Data System). Eur Urol 2018; 74:294e306.
|
| [17] |
Kim SH. Validation of vesical imaging reporting and data system for assessing muscle invasion in bladder tumor. Abdom Radiol (NY) 2020; 45:491e8.
|
| [18] |
Barchetti G, Simone G, Ceravolo I, Salvo V, Campa R, Del Giudice F, et al. Multiparametric MRI of the bladder: interobserver agreement and accuracy with the Vesical Imaging- Reporting and Data System (VI-RADS) at a single reference center. Eur Radiol 2019; 29:5498e506.
|
| [19] |
Ueno Y, Takeuchi M, Tamada T, Sofue K, Takahashi S, Kamishima Y, et al. Diagnostic accuracy and interobserver agreement for the Vesical Imaging-Reporting and Data System for muscle-invasive bladder cancer: a multireader validation study. Eur Urol 2019; 76:54e6.
|
| [20] |
Wang H, Luo C, Zhang F, Guan J, Li S, Yao H, et al. Multiparametric MRI for bladder cancer: validation of VI-RADS for the detection of detrusor muscle invasion. Radiology 2019; 291:668e74.
|
| [21] |
Del Giudice F, Barchetti G, De Berardinis E, Pecoraro M, Salvo V, Simone G, et al. Prospective assessment of Vesical Imaging Reporting and Data System (VI-RADS) and its clinical impact on the management of high-risk non-muscle-invasive bladder cancer patients candidate for repeated transurethral resection. Eur Urol 2020; 77:101e9.
|
| [22] |
Marchioni M, Primiceri G, Delli Pizzi A, Basilico R, Berardinelli F, Mincuzzi E, et al. Could bladder multiparametric MRI be introduced in routine clinical practice? Role of the new VI-RADS score: results from a prospective study. Clin Genitourin Cancer 2020; 18:409e15.
|
| [23] |
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68:394e424.
|
| [24] |
Shariat SF, Palapattu GS, Karakiewicz PI, Rogers CG, Vazina A, Bastian PJ, et al. Discrepancy between clinical and pathologic stage: impact on prognosis after radical cystectomy. Eur Urol 2007; 51:137e51.
|
|
|
|