Prospective randomized study correlating intra-operative urethral mucosal injury with early period after transurethral resection of the prostate stricture urethra: A novel concept
Suresh B. Patankar,Mayur M. Narkhede*(),Gururaj Padasalagi,Kashinath Thakare
Department of Urology, Ace Hospital, Pune, ASP Medical Foundation, Sripad Medisearch PVT LTD, India
Objective: To investigate the incidence of urethral stricture during the early period after transurethral resection of the prostate (TURP) and correlate its incidence with intra-operative urethral mucosal injury during TURP. Also to compare the other established risk factors affecting the development of urethral stricture among patients undergoing monopolar or bipolar TURP over a period of 6 months follow-up as the prospective randomized study.
Methods: One hundred and fifty men older than 50 years with lower-urinary tract symptoms associated with benign prostatic hyperplasia were randomized to undergo either standard monopolar TURP with glycine as the irrigation fluid or bipolar TURP with normal saline as irrigant. The prostate size, operative time, intra-operative mucosal rupture, catheter time, catheter traction duration, uroflowmetry, and post-operative stricture rate were compared.
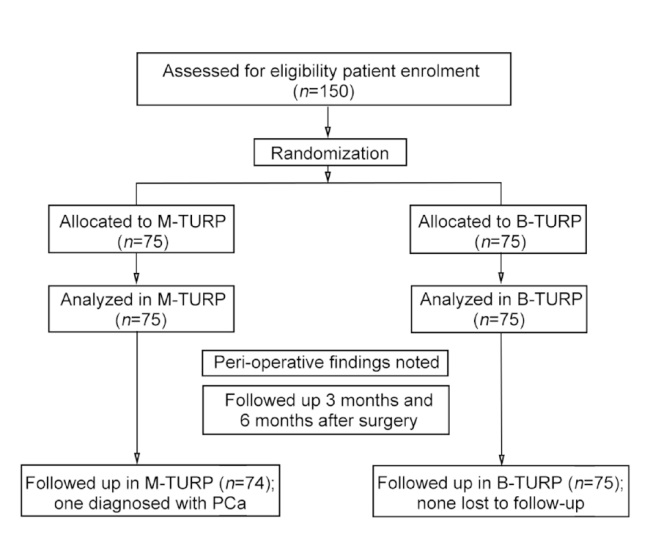
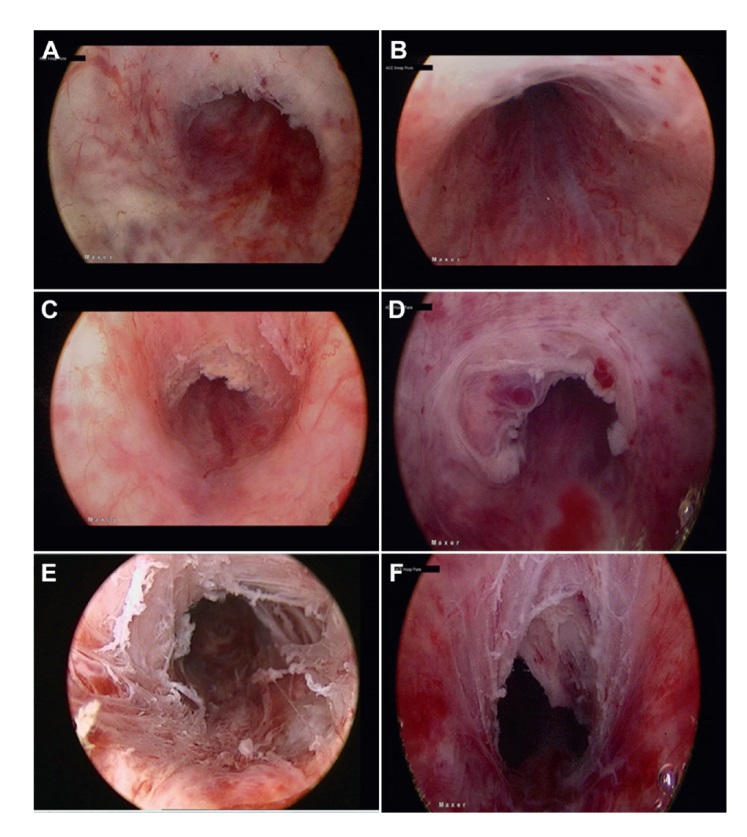
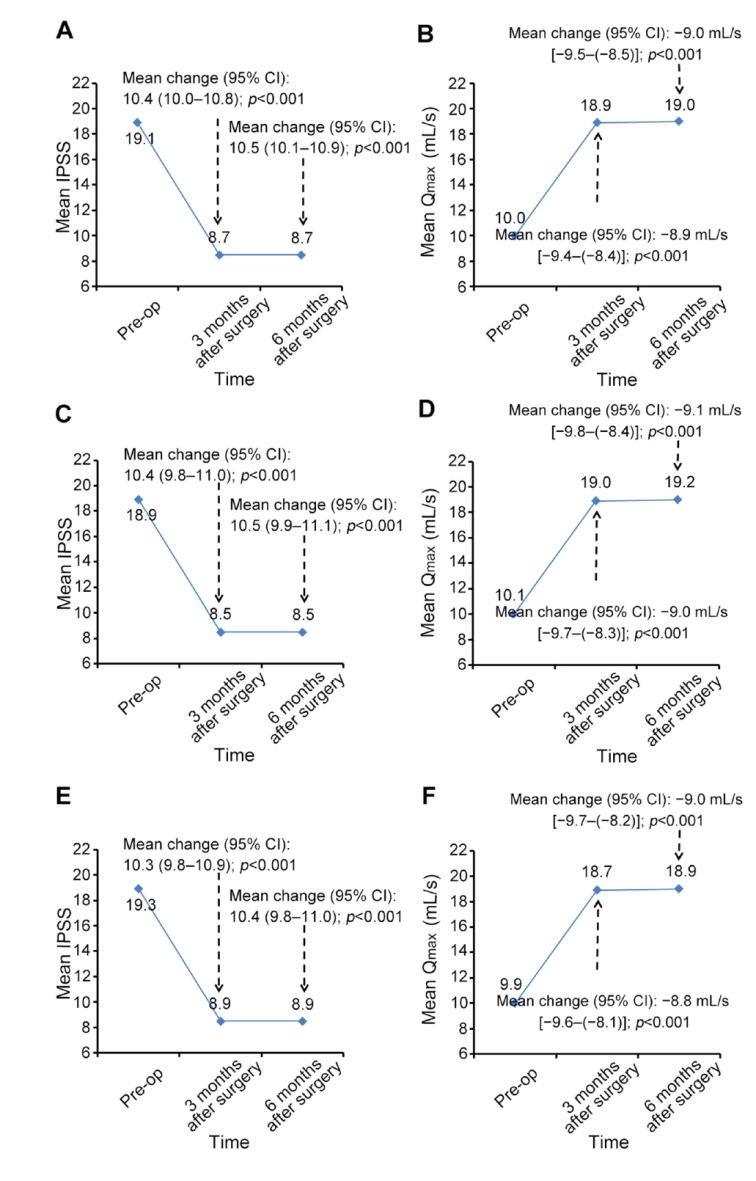
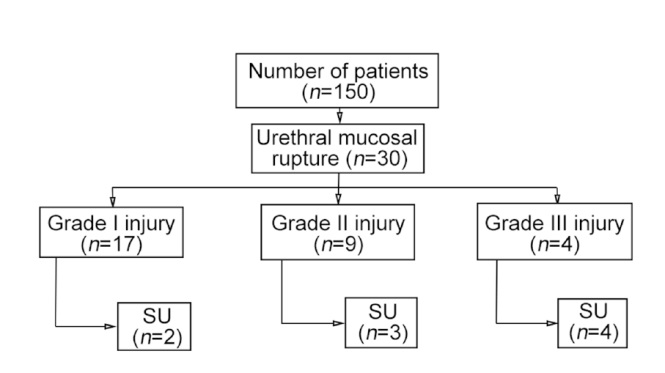
Results: A total of 150 patients underwent TURP, including 74 patients undergoing monopolar TURP (one patient was excluded as his post-operative histopathological examination report was of adenocarcinoma prostate) and 75 patients undergoing bipolar-TURP, all of which were performed using a 26 Fr sheath resectoscope. The mean International Prostate Symptom Score and maximum urinary flow rate score at post-operative 3 months and 6 months were comparable between the groups. Out of 149 patients, nine patients (6.0%) developed urethral stricture. The severity of the injury (urethral mucosal injury) correlated with the likelihood of developing a subsequent complication (stricture urethra). Patients with stricture had significantly larger prostate volume than patients without stricture (65.0 mL vs. 50.0 mL; p=0.030). Patients with stricture had longer operative time than patients without stricture (55.0 min vs. 40.0 min; p=0.002). In both procedures, formation of post-operative stricture urethra was independently associated with intra-operative mucosal injury.
Conclusion: Intra-operative recognition of urethral mucosal injury helps in prediction of stricture urethra formation in early post-operative period.
. [J]. Asian Journal of Urology, 2024, 11(3): 466-472.
Suresh B. Patankar, Mayur M. Narkhede, Gururaj Padasalagi, Kashinath Thakare. Prospective randomized study correlating intra-operative urethral mucosal injury with early period after transurethral resection of the prostate stricture urethra: A novel concept. Asian Journal of Urology, 2024, 11(3): 466-472.
Madersbacher S, Alivizatos G, Nordling J, Sanz CR, Emberton M, de la Rosette JJ. EAU 2004 guidelines on assessment, therapy and follow-up of men with lower urinary tract symptoms suggestive of benign prostatic obstruction (BPH guidelines). Eur Urol 2004 ; 46:547-54.
[2]
Mamoulakis C, Trompetter M, de La Rosette J. Bipolar transurethral resection of the prostate: the “golden standard” reclaims its leading position. Curr Opin Urol 2009; 19:26-32.
[3]
Michielsen DP, Coomans D, Engels B, Braeckman JG. Bipolar versus monopolar technique for palliative transurethral prostate resection. Arch Med Sci 2010; 6:780-6.
[4]
Rassweiler J, Teber D, Kuntz R, Hofmann R. Complications of transurethral resection of the prostate (TURP)dincidence, management, and prevention. Eur Urol 2006; 50:969-79.
[5]
Tan GH, Shah SA, Ali NM, Goh EH, Singam P, Ho CCK, et al. Urethral strictures after bipolar transurethral resection of prostate may be linked to slow resection rate. Investig Clin Urol 2017; 58:186-91.
[6]
Issa MM. Technological advances in transurethral resection of the prostate: bipolar versus monopolarturp. J Endourol 2008; 22:1587-95.
[7]
Doluoglu OG, Gokkaya CS, Aktas BK, Oztekin CV, Bulut S, Memis A, et al. Impact of asymptomatic prostatitis on re- operations due to urethral stricture or bladder neck contracture developed after TUR-P. Int Urol Nephrol 2012; 44:1085-90.
[8]
Michielsen DP, Coomans D. Urethral strictures and bipolartrans urethral resection in saline of the prostate: fact or fiction? J Endourol 2010; 24:1333-7.
[9]
Eri LM, Thomassen H, Brennhovd B, Ha°heim LL. Accuracy and repeatability of prostate volume measurements by transrectal ultrasound. Prostate Cancer Prostatic Dis 2002; 5:273-8.
[10]
Reich O, Gratzke C, Stief CG. Techniques and long-term results of surgical procedures for BPH. Eur Urol 2006; 49:970-8.
[11]
Mamoulakis C, Ubbink DT, de la Rosette JJ. Bipolar versus monopolar transurethral resection of the prostate: a systematic review and meta-analysis of randomized controlled trials. Eur Urol 2009; 56:798-809.
[12]
Sciarra A, Salciccia S, Albanesi L, Cardi A, D’Eramo G, Di Silverio F. Use of cyclooxygenase-2 inhibitor for prevention of urethral strictures secondary to transurethral resection of the prostate. Urology 2005; 66:1218-22.
[13]
Park JK, Lee SK, Han SH, Kim SD, Choi KS, Kim MK. Is warm temperature necessary to prevent urethral stricture in combined transurethral resection and vaporization of prostate? Urology 2009; 74:125-9.
[14]
Villaa P, Ugaldea MS, Martínb ML, Pe?a FM. Risk factors for developing urethral stricture in patients that underwent transurethral resection of the prostate. Rev Mex Urol 2013; 73:166-74.
[15]
Hoffmann R. [Transurethrale resektion (TURP) und transurethrale inzision (TUIP) der prostata]. In: HoffmannR, editor. EndoskopischeUrologie. Heidelberg: Springer; 2005. p. 50-84. [Book in German].
[16]
Lentz HC Jr, Mebust WK, Foret JD, Melchior J. Urethral strictures following transurethral prostatectomy: review of 2223 resections. J Urol 1977; 117:194-6.
[17]
Varkarakis J, Bartsch G, Horninger W. Long-term morbidity and mortality of transurethral prostatectomy: a 10-year follow-up. Prostate 2004; 58:248-51.
[18]
Wang JW, Man LB. Transurethral resection of the prostate stricture management. Asian J Androl 2020; 22:140-4.
[19]
Mundy AR, Andrich DE. Urethral strictures. BJU Int 2011; 107:6-26.
[20]
Komura K, Inamoto T, Takai T, Uchimoto T, Saito K, Tanda N, et al. Incidence of urethral stricture after bipolar transurethral resection of the prostate using TURis: results from a randomized trial. BJU Int 2015; 115:644-52.
[21]
Smith TG. Current management of urethral stricture disease. Indian J Urol 2016; 32:27-33.
[22]
Sarier M, Duman I, Kilic S, Yuksel Y, Demir M, Aslan M, et al. Comparative results of transurethral incision with transurethral resection of the prostate in renal transplant recipients with benign prostate hyperplasia. Urol J 2018; 15:209-13.
[23]
Sarier M, Duman I, Demir M, Yuksel Y, Emek M, Kukul E. The outcomes of transurethral incision/resection of the prostate (TUIP/TURP) performed early after renal transplantation. Turk Uroloji Dergisi/Turkish. J Urol 2018; 44:172-7.
[24]
Kulkarni SB, Joglekar O, Alkandari M, Joshi PM. Management of post TURP strictures. World J Urol 2019; 37:589-94.