aDepartment of Urology, Zhongnan Hospital of Wuhan University, Wuhan, China bDepartment of Urology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China
Objective: To describe and evaluate the technique using bilateral Boari flap ureteroneocystostomy (BBFUNC) for bilateral mid-lower ureteral strictures.
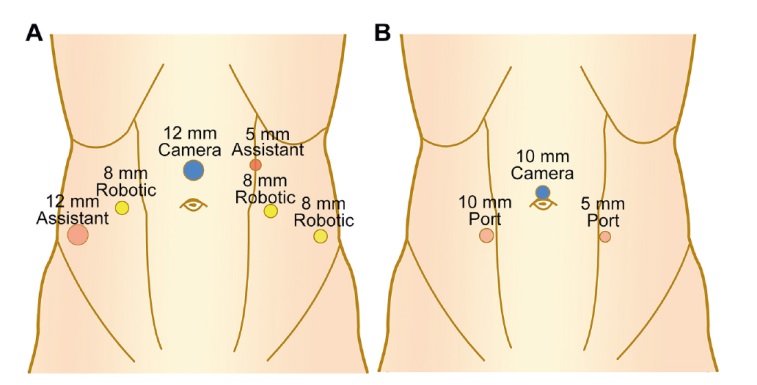
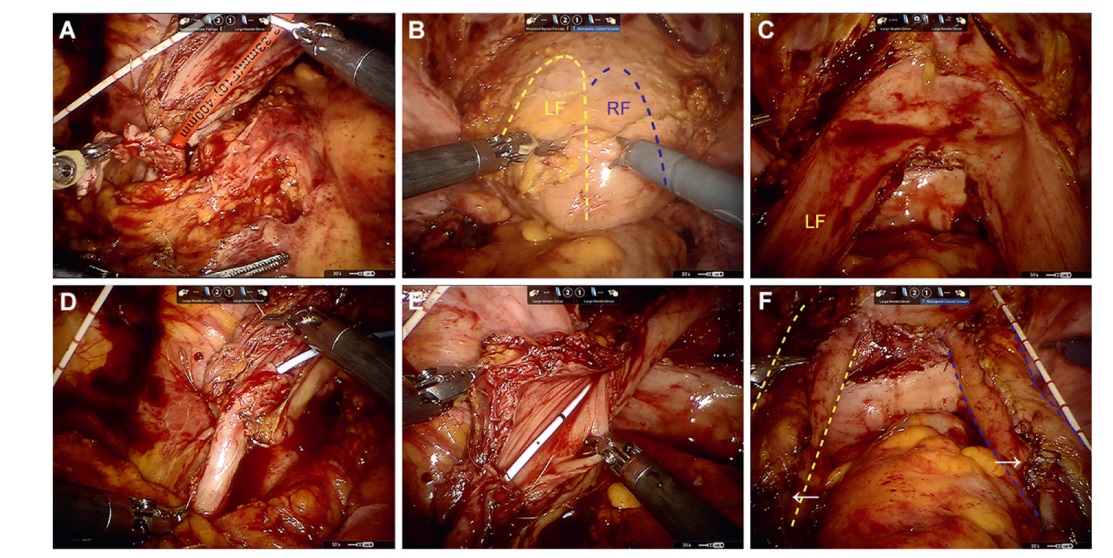
Methods: We retrospectively reviewed five patients who underwent minimally invasive BBFUNC in our institution (Union Hospital, Wuhan, China) between July 2019 and December 2021. The bilateral ureters were mobilized and transected above the stenotic segments. The bladder was isolated and incised longitudinally from the middle of the anterior wall. Then, an inverted U-shaped bladder flap was created on both sides, fixed onto the psoas tendon, and anastomosed to the ipsilateral distal normal ureter. Following double-J stenting, the Boari flaps were tubularized, and the bladder was closed with continuous sutures. The patients' perioperative data and follow-up outcomes were collected, and a descriptive statistical analysis was performed.
Results: No case converted to open surgery, and no intraoperative complication occurred. The median surgical time was 230 (range 203-294) min. The median length of the bladder flaps was 6.2 (range 4.3-10.0) cm on the left and 5.5 (range 4.7-10.5) cm on the right side. All patients had not developed recurrent ureteral stenosis during the median follow-up time of 17 (range 16-45) months and had a normal maximum flow rate after surgery. The median post-void residual was 7 (range 0-19) mL. The maximal bladder capacity was decreased in one (20%) patient.
Conclusion: The present study demonstrates that minimally invasive BBFUNC is feasible and safe in treating bilateral mid-lower ureteral strictures, and the impact on lower urinary tract function is limited.
Nausea, vomiting, and urinary urgency and frequency
None
Left flank pain
Bilateral flank pain
-
Stricture locationa
Left
S3
S2
S3
S2
L5
-
Right
S3
S1
S2
S2
L5
-
Preoperative hydronephrosisb
Left
Grade 3
Grade 2
Grade 4
Grade 2
Grade 3
-
Right
Grade 3
Grade 3
Grade 2
Grade 4
Grade 3
-
Preoperative SRF, mL/min
Left
33.7
46.3
9.6
55.6
47.4
46.3 (9.6-55.6)
Right
35.7
21.4
74.6
45.0
49.8
45.0 (21.4-74.6)
Perioperative and follow-up results
Case 1
Case 2
Case 3
Case 4
Case 5
Median (range)
Procedure
L-BBFUNC
RA-BBFUNC
L-BBFUNC
RA-BBFUNC
L-BBFUNC
-
Operative time, min
237
210
294
203
230
230 (203-294)
Flap length, cm
Left
5.2
8.3
4.3
6.2
10.0
6.2 (4.3-10.0)
Right
4.7
9.8
5.5
5.5
10.5
5.5 (4.7-10.5)
Estimated blood loss, mL
40
150
110
80
50
80 (40-150)
Intraoperative complication
None
None
None
None
None
-
Postoperative hospitalization, day
7
6
6
6
7
6 (6-7)
Postoperative hydronephrosis
Left
Grade 0
Grade 0
Grade 1
Grade 1
Grade 2
-
Right
Grade 0
Grade 1
Grade 2
Grade 1
Grade 2
-
Postoperative SRF, mL/min
Left
30.2
45.4
12.9
49.6
68.4
45.4 (12.9-68.4)
Right
49.5
23.1
82.1
42.9
59.8
49.5 (23.1-82.1)
Symptoms after surgerya
3 months
FPV
FPV and FU
FPV
FPV and FU
None
-
6 months
None
None
None
None
None
-
LUT function assessment after surgeryb
Post-void residual, mL
0
3
7
19
10
7 (0-19)
Qmax, mL/s
44.5
27.8
18.2
19.5
26.9
26.9 (18.2-44.5)
Maximal bladder capacity, mL
405
517
282
530
488
488 (282-530)
Follow-up time, month
45
18
17
17
16
17 (16-45)
[1]
Engel O, Rink M, Fisch M. Management of iatrogenic ureteral injury and techniques for ureteral reconstruction. Curr Opin Urol 2015; 25:331-5.
[2]
Lee Z, Waldorf BT, Cho EY, Liu JC, Metro MJ, Eun DD. Robotic ureteroplasty with buccal mucosa graft for the management of complex ureteral strictures. J Urol 2017; 198:1430-5.
[3]
Liang C, Wang J, Hai B, Xu Y, Zeng J, Chai S, et al. Lingual mucosal graft ureteroplasty for long proximal ureteral stricture: 6 years of experience with 41 cases. Eur Urol 2022; 82:193-200.
[4]
Fernbach SK, Maizels M, Conway JJ. Ultrasound grading of hydronephrosis: introduction to the system used by the Society for Fetal Urology. Pediatr Radiol 1993; 23:478-80.
[5]
Musch M, Hohenhorst L, Pailliart A, Loewen H, Davoudi Y, Kroepfl D. Robot-assisted reconstructive surgery of the distal ureter: single institution experience in 16 patients. BJU Int 2013; 111:773-83.
[6]
Stolzenburg JU, Rai BP, Do M, Dietel A, Liatsikos E, Ganzer R, et al. Robot-assisted technique for Boari flap ureteric reimplantation: replicating the techniques of open surgery in robotics. BJU Int 2016; 118:482-4.
[7]
El Abd AS, El-Abd SA, El-Enen MA, Tawfik AM, Soliman MG, Farha MA, et al. Immediate and late management of iatrogenic ureteric injuries: 28 years of experience. Arab J Urol 2015; 13:250-7.
[8]
Slawin J, Patel NH, Lee Z, Dy GW, Kim D, Asghar A, et al. Ureteral reimplantation via robotic nontransecting side-toside anastomosis for distal ureteral stricture. J Endourol 2020; 34:836-9.
[9]
Armatys SA, Mellon MJ, Beck SD, Koch MO, Foster RS, Bihrle R. Use of ileum as ureteral replacement in urological reconstruction. J Urol 2009; 181:177-81.
Kocot A, Kalogirou C, Vergho D, Riedmiller H. Long-term results of ileal ureteric replacement: a 25-year single-centre experience. BJU Int 2017; 120:273-9.
[12]
Elbers JR, Rodriguez Socarras M, Rivas JG, Autran AM, Esperto F, Tortolero L, et al. Robotic repair of ureteral strictures: techniques and review. Curr Urol Rep 2021; 22:39. https://doi.org/10.1007/s11934-021-01056-8
doi: https://doi.org/10.1007/s11934-021-01056-8
pmid: 34105032
[13]
Ficarra V, Rossanese M, Crestani A, Caloggero S, Alario G, Novara G, et al. A contemporary case series of complex surgical repair of surgical/endoscopic injuries to the abdominal ureter. Eur Urol Focus 2021; 7:1476-84.
[14]
Li Y, Li C, Yang S, Song C, Liao W, Xiong Y. Reconstructing fulllength ureteral defects using a spiral bladder muscle flap with vascular pedicles. Urology 2014; 83:1199-204.
[15]
Sanadizadeh SM, McCague NJ. Repair of lower ureteral injuries using bladder flap. J Urol 1967; 98:81-5.
[16]
Thompson IM, Karow WF, Ross G Jr. Long-term results of ureteral reimplantation for trauma. J Urol 1969; 102:308-15.
[17]
Sagalovich D, Garisto J, Bertolo R, Yerram N, Dagenais J, Chavali JS, et al. Minimally invasive management of ureteral distal strictures: robotic ureteroneocystostomy with a bilateral boari flap. Urology 2018; 120:268. https://doi.org/10.1016/j.urology.2018.06.023
doi: https://doi.org/10.1016/j.urology.2018.06.023
pmid: 30077539
[18]
Lee Z, Moore B, Giusto L, Eun DD. Use of indocyanine green during robot-assisted ureteral reconstructions. Eur Urol 2015; 67:291-8.