aDepartment of Urology, The Affiliated Ganzhou Hospital of Nanchang University, Ganzhou, Jiangxi, China bXie Urology, Margate, FL, USA cLiaobu Township Community Health Service Center, Dongguan, Guangdong, China dGan County District Dermatology Institute, Ganzhou, Jiangxi, China
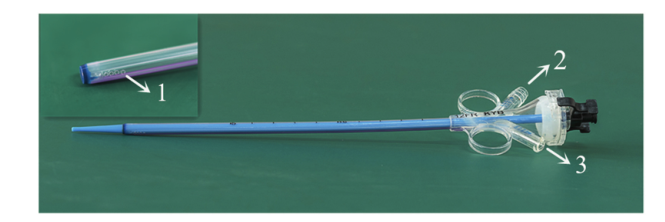
Objective: The purpose of the study was to assess the clinical efficacy and safety of a combined perfusion suction platform with pressure feedback control function and an ureteroscopic suction sheath that can measure the ureteropelvic pressure in implementing lithotripsies. Methods: Fifty-two patients who underwent lithotripsy under intelligent monitoring of ureteral intraluminal pressure from June 2016 to January 2018 were retrospectively recruited. The inclusion standard was stone diameter >1.5 cm but <2.5 cm. After the 12/14 Fr suction sheath was placed, manometer interface and suction interface of the sheath were connected to the platform via the pressure sensor and suction tube, respectively. The ureteroscope was connected to the platform perfusion pump, and the crushed stones were aspirated out under negative pressure. Results: According to the location of the stone, 21 (40.4%) cases were classified as upper ureteral stones, 19 (36.5%) were midureteral stones, and 12 (23.1%) were lower ureteral stones. Forty-seven patients underwent successful primary sheath placement and lithotripsy with a mean operative time of 34.5 (standard deviation 18.3) min. Retrograde stone migration did not occur. There were eight patients with hematuria postoperatively. Serious complication was 1.9% with one case of ureteral perforation. Stone clearance was 95.7% at Day 1-2 postoperatively, and 100% at Day 30 postoperatively. Conclusion: Ureteroscopic lithotripsy with intelligent pressure control using our device improved the efficiency of the lithotripsy and rate of stone clearance. The safety of the operation can be ensured. It is worth popularization and application in clinical practice.
Complication (Clavien-Dindo categorization), n (%)
Hematuria (Clavien Grade I)
8 (17.0)
Stone upward migration (Clavien Grade III)
0
Ureteral extravasation (Trexer Grade III)
1 (2.1)
Postoperative hospitalization duration, mean±SD, day
2.1±1.1
[1]
Türk C, Neisius A, Pet?ík A, Seitz C, Skolarikos A, Somani B, et al. EAU guidelines on urolithiasis. Available at: https://uroweb.org/guideline/urolithiasis.[Accessed 27 October 2017].
[2]
Taguchi K, Cho S, Ng A, Usawachintachit M, Tan Y, Deng Y, et al. The Urological Association of Asia clinical guideline for urinary stone disease. Int J Urol 2019; 26:688-709.
doi: 10.1111/iju.13957
pmid: 31016804
[3]
Takayasu H, Aso Y. Recent development for pyelouretero- scopy: guide tube method for its introduction into the ureter. J Urol 1974; 112:176-8.
doi: 10.1016/s0022-5347(17)59675-5
pmid: 4843325
[4]
Santos JMR. Ureteroscopy from the recent past to the near future. Urolithiasis 2018; 46:31-7.
doi: 10.1007/s00240-017-1016-8
pmid: 29188308
[5]
Zeng G, Wang D, Zhang T, Wan S. Modified access sheath for continuous flow ureteroscopic lithotripsy: a preliminary report of a novel concept and technique. J Endourol 2016; 30:992-6.
[6]
Zhu X, Song L, Xie D, Peng Z, Guo S, Deng X, et al. Animal experimental study to test application of intelligent pressure control device in monitoring and control of renal pelvic pressure during flexible ureteroscopy. Urology 2016; 91: 242.e11-5. https://doi.org/10.1016/j.urology.2016.02.022.
doi: 10.1016/j.urology.2016.02.022
[7]
Deng X, Song L, Xie D, Fan D, Zhu L, Yao L, et al. A novel flexible ureteroscopy with intelligent control of renal pelvic pressure: an initial experience of 93 cases. J Endourol 2016; 30:1067-72.
pmid: 27558001
[8]
Chen H, Qiu X, Du C, Xie D, Liu T, Wang G, et al. The com-parison study of flexible ureteroscopic suctioning lithotripsy with intelligent pressure control versus minimally invasive percutaneous suctioning nephrolithotomy in treating renal calculi of 2 to 3 cm in size. Surg Innovat 2019; 26:528-35.
[9]
Zeng G, Zhong W, Li X, Chen W, He Y, He Z, et al. The influ- ence of minimally invasive percutaneous nephrolithotomy on renal pelvic pressure in vivo. Surg Laparosc Endosc Percuta- neous Tech 2007; 17:307-10.
[10]
Zhong W, Zeng G, Wu K, Li X, Chen W, Yang H. Does a smaller tract in percutaneous nephrolithotomy contribute to high renal pelvic pressure and postoperative fever? J Endourol 2008; 22:2147-51.
doi: 10.1089/end.2008.0001
pmid: 18811571
[11]
Tokas T, Herrmann TRW, Skolarikos A, Nagele U. Pressure matters: intrarenal pressures during normal and pathological conditions, and impact of increased values to renal physiology. World J Urol 2018; 33:1-7.
[12]
Thomsen HS. Pyelorenal backflow. Clinical and experimental investigations. Radiologic, nuclear, medical and pathoana- tomic studies. Dan Med Bull 1984; 31:438-57.
pmid: 6394220
[13]
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004; 240: 205-13.
doi: 10.1097/01.sla.0000133083.54934.ae
pmid: 15273542
[14]
Traxer O, Thomas A. Prospective evaluation and classification of ureteral wall injuries resulting from the insertion of a ureteral access sheath during, retrograde intra-renal surgery (RIRS). J Urol 2012; 189:580-4.
doi: 10.1016/j.juro.2012.08.197
[15]
Young HH, McKay RW. Congenital valvular obstruction of the posterior urethra. Surg Gynecol Obstet 1929; 48:509-35.
doi: 10.1097/00006254-199307000-00028
[16]
Heers H, Turney BW. Trends in urological stone disease: a 5- year update of hospital episode statistics. BJU Int 2016; 118: 785-9.
doi: 10.1111/bju.2016.118.issue-5
[17]
Tokas T, Herrmann TRW, Skolarikos A, Nagele U; Training and Research in Urological Surgery and Technology (T.R.U.S.T.)- Group. Pressure matters: intrarenal pressures during normal and pathological conditions, and impact of increased values to renal physiology. World J Urol 2019; 37:125-31.
doi: 10.1007/s00345-018-2378-4
pmid: 29915945
[18]
Kallidonis P, Ntasiotis P, Knoll T, Sarica K, Papatsoris A, Somani BK, et al. Minimally invasive surgical ureterolithotomy versus ureteroscopic lithotripsy for large ureteric stones: a systematic review and meta-analysis of the literature. Eur Urol Focus 2017; 3:554-66.
doi: S2405-4569(17)30108-6
pmid: 28753887
[19]
Kumar A, Vasudeva P, Nanda B, Niraj Kumar N, Kumar SJ, Singh H. A prospective randomized comparison between laparoscopic ureterolithotomy and semirigid ureteroscopy for upper ureteral stones >2 cm: a single-center experience. J Endourol 2015; 29:1248-52.
doi: 10.1089/end.2013.0791
pmid: 25177768
[20]
Kadyan B, Sabale V, Mane D, Satav V, Mulay A, Thakur N, et al. Large proximal ureteral stones: ideal treatment modality? Urol Ann 2016; 8:189-92.
doi: 10.4103/0974-7796.157963
pmid: 27141190
[21]
Bozkurt IH, Yonguc T, Arslan B, Degirmenci T, Gunlusoy B, Aydogdu O, et al. Minimally invasive surgical treatment for large impacted upper ureteral stones: ureteroscopic litho-tripsy or percutaneous nephrolithotomy? Can Urol Assoc J 2015; 9:E122-5. https://doi.org/10.5489/cuaj.2280.
[22]
Deng X, Song L, Xie D, Zhu L, Peng Z. Suctioning flexible ure- teroscopy with automatic control of renal pelvic pressure. J Endourol 2015; 195:e782. https://doi.org/10.1016/j.juro.2016.02.813.
[23]
Peng G, Song L, Xie D, Huang J, Zhong Y, Tan W, et al. Suctioning flexible ureteroscopic lithotripsy in the oblique supine lithotomy position and supine lithotomy position: a comparative retrospective study. Minerva Urol Nefrol 2018; 70: 612-6.
doi: 10.23736/S0393-2249.18.03144-2
pmid: 30037207