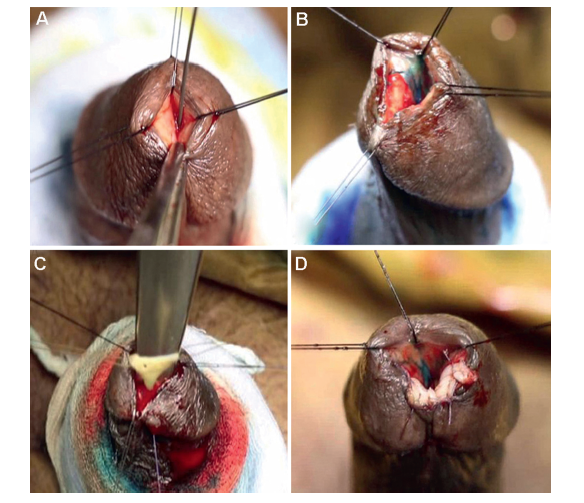
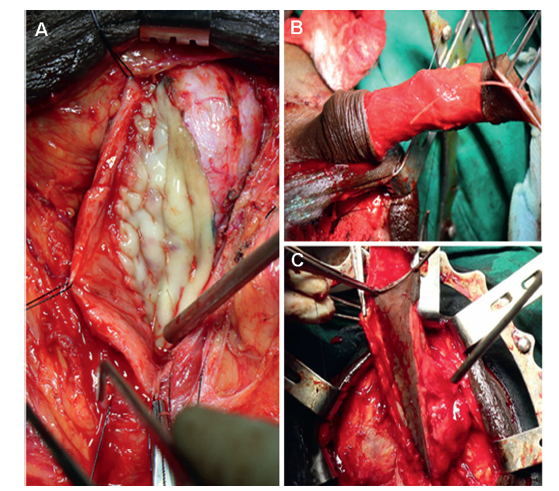
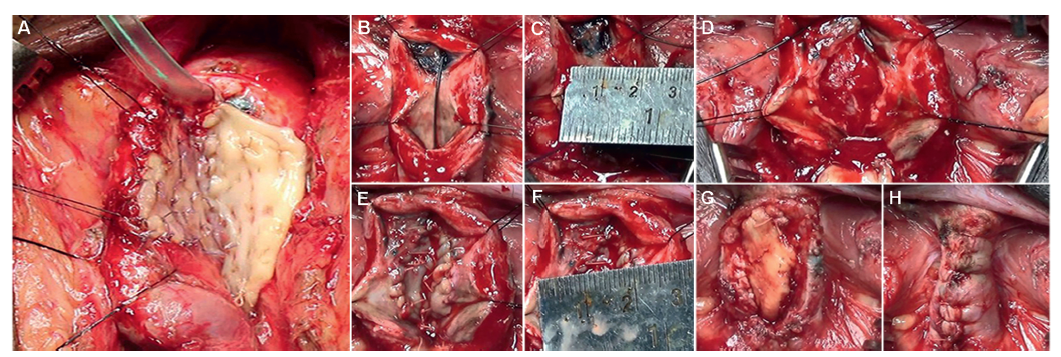
Objective: Urethral stricture disease after endo-urological treatment of benign prostatic hyperplasia (BPH) is a sparsely described complication. We describe management of five categories of these strictures in this retrospective observational case series. Methods: One hundred and twenty-one patients presenting with symptoms of bladder outflow obstruction after endo-urological intervention for BPH from February 2016 to March 2019 were evaluated. Among them, 76 were eligible for this study and underwent reconstructive surgery. Preoperative and postoperative assessments were done with symptom scores, uroflowmetry, ultrasound for post-void residue, and urethrogram. Any intervention during follow-up was classed as a failure. The recurrence and 95% confidence interval for recurrence percentage were calculated. Results: The following five categories of patients were identified: Bulbo-membranous (33 [43.4%]), navicular fossa (21 [27.6%]), penile/peno-bulbar (8 [10.5%]), bladder neck stenosis (6 [7.9%]), and multiple locations (8 [10.5%]). The average age was 69 years (range: 60-84 years). Overall average symptom score, flow rate, and post-void residue changed from 21 to 7, 6 mL/s to 19 mL/s, and 210 mL to 20 mL, respectively. The average follow-up was 34 months (range: 12-58 months). Overall recurrence and complication rates were 10.5% and 9.2%, respectively. The recurrence in each category was seen in 3, 1, 2, 1, and 1 patient, respectively. Overall 95% confidence interval for recurrence percentage was 4.66-19.69. Conclusion: Urethral stricture disease is a major long-term complication of endo-urological treatment of BPH. The bulbo-membranous strictures need continence preserving approach. Navicular fossa strictures require minimally invasive and cosmetic consideration. Peno-bulbar strictures require judicious use of grafts and flaps. Bladder neck stenosis in this cohort could be treated with endoscopic measures. Multiple locations need treatment based on their sites in single-stage as far as possible.
. [J]. Asian Journal of Urology, 2023, 10(2): 137-143.
Rajiv N. Kore. Management of urethral strictures and stenosis caused by the endo-urological treatment of benign prostatic hyperplasia—a single-center experience. Asian Journal of Urology, 2023, 10(2): 137-143.
Average number of interventions prior to treatment
Recurrence after treatment, n (%)
95% CI for recurrence percentage
Bulbo-membranous
33 (43.4)
4
3 (9.1)
(1.92, 24.33)
Navicular fossa
21 (27.6)
2
1 (4.8)
(0.12, 23.82)
Penile
8 (10.5)
2
2 (25.0)
(3.19, 65.09)
BNS
6 (7.9)
1
1 (16.7)
(0.42, 64.12)
Multiple locations
8 (10.5)
2
1 (12.5)
(0.32, 52.65)
Total
76
11
8 (10.5)
(4.66, 19.69)
[1]
Michielsen DP, Coomans D. Urethral strictures and bipolar transurethral resection in saline of the prostate: fact or fiction. J Endourol 2010; 24:1333-7.
doi: 10.1089/end.2009.0575
pmid: 20583960
[2]
Hillary CJ, Osman NI, Chapple CR. Current trends in urethral stricture management. Asian J Urol 2014; 1:46-54.
doi: 10.1016/j.ajur.2015.04.005
pmid: 29511637
[3]
Barbagli G, Kulkarni SB, Joshi PM, Nikolavsky D, Montorsi F, Sansalone S, et al. Repair of sphincter urethral strictures preserving urinary continence: surgical technique and outcomes. World J Urol 2019; 37:2473-9.
doi: 10.1007/s00345-019-02686-x
pmid: 30798381
Rassweiler J, Teber D, Kuntz R, Hofmann R. Complications of transurethral resection of the prostate (TURP)dincidence, management, and prevention. Eur Urol 2006; 50:969-80.
doi: 10.1016/j.eururo.2005.12.042
pmid: 16469429
[7]
Tefekli A, Muslumanoglu AY, Baykal M, Binbay M, Tas A, Altunrende F. A hybrid technique using bipolar energy in transurethral prostate surgery: a prospective, randomized comparison. J Urol 2005; 174:1339-43.
doi: 10.1097/01.ju.0000173075.62504.73
pmid: 16145415
[8]
Seckiner I, Yesilli C, Akduman B, Altan K, Mungan NA. A prospective randomized study for comparing bipolar plasma kinetic resection of the prostate with standard TURP. Urol Int 2006; 76:139-43.
doi: 10.1159/000090877
pmid: 16493215
[9]
Falahatkar S, Mokhtari G, Moghaddam KG, Asadollahzade A, Farzan A, Shahab E, et al. Bipolar transurethral vaporization: a superior procedure in benign prostatic hyperplasia: a prospective randomized comparison with bipolar TURP. Int Braz J Urol 2014; 40:346-55.
doi: 10.1590/S1677-5538.IBJU.2014.03.08
pmid: 25010300
[10]
Reich O, Gratzke C, Stief CG. Techniques and long-term results of surgical procedures for BPH. Eur Urol 2006; 49:970-8.
doi: 10.1016/j.eururo.2005.12.072
pmid: 16481092
[11]
Naspro R, Bachmann A, Gilling P, Kuntz R, Madersbacher S, Montorsi F, et al. A review of the recent evidence (2006e2008) for 532-nm photoselective laser vaporization and holmium laser enucleation of the prostate. Eur Urol 2009; 55:1345-57.
doi: 10.1016/j.eururo.2009.03.070
[12]
Sall M, Bruskewitz RC. Prostatic urethral strictures after transurethral microwave thermal therapy for benign prostatic hyperplasia. Urology 1997; 50:983-5.
pmid: 9426738
[13]
Chen ML, Correa AF, Santucci RA. Urethral strictures and stenoses caused by prostate therapy. Rev Urol 2016; 18: 90-102.
doi: 10.3909/riu0685
pmid: 27601967
[14]
Tonkin JB, Jordan GH. Management of distal anterior urethral strictures. Nat Rev Urol 2009; 6:533-8.
doi: 10.1038/nrurol.2009.181
pmid: 19736550
[15]
Cohney BC. A penile flap procedure for the relief of meatal stricture. Br J Urol 1963; 35:182-3.
pmid: 14022148
Nikolavsky D, Abouelleil M, Daneshvar M. Transurethral ventral buccal mucosa graft inlay urethroplasty for reconstruction of fossa navicularis and distal urethral strictures: surgical technique and preliminary results. Int Urol Nephrol 2016; 48:1823-9.
pmid: 27470030
[18]
Barbagli G, Palminteri E, Guazzoni G, Cavalcanti A. Bulbar urethroplasty using the dorsal approach: current techniques. Int Braz J Urol 2003; 29:155-61.
pmid: 15745501
Gelman J, Siegel JA. Ventral and dorsal buccal grafting for 1- stage repair of complex anterior urethral strictures. Urology 2014; 83:1418-22.
doi: 10.1016/j.urology.2014.01.024
pmid: 24745799
[23]
Palminteri E, Manzoni G, Berdondini E, Di Fiore F, Testa G, Poluzzi M, et al. Combined dorsal plus ventral double buccal mucosa graft in bulbar urethral reconstruction. Eur Urol 2008; 53:81-9.
doi: 10.1016/j.eururo.2007.05.033
pmid: 17583417
[24]
Yadav SS, Singh VK, Tomar V, Agarwal N, Gulani A. Technique for single-stage reconstruction of obliterative or nearobliterative long urethral strictures in circumcised patients. Investig Clin Urol 2018; 59:213-9.
doi: 10.4111/icu.2018.59.3.213
pmid: 29744480
[25]
Lee YH, Chiu AW, Huang JK. Comprehensive study of bladder neck contracture after transurethral resection of prostate. Urology 2005; 65:498-503.
doi: 10.1016/j.urology.2004.10.082
[26]
Doluoglu OG, Gokkaya CS, Aktas BK, Oztekin CV, Bulut S, Memis A, et al. Impact of asymptomatic prostatitis on reoperations due to urethral stricture or bladder neck contracture developed after TUR-P. Int Urol Nephrol 2012; 44: 1085-90.
doi: 10.1007/s11255-012-0127-y
pmid: 22252218
Pansadoro V, Emiliozzi P. Iatrogenic prostatic urethral strictures: classification and endoscopic treatment. Urology 1999; 53:784-9.
pmid: 10197857
[29]
Kranz J, Reiss PC, Salomon G, Steffens J, Fisch M, Rosenbaum CM. Differences in recurrence rate and de novo incontinence after endoscopic treatment of vesicourethral stenosis and bladder neck stenosis. Front Surg 2017; 4:44. https://doi.org/10.3389/fsurg.2017.00044.
doi: 10.3389/fsurg.2017.00044
[30]
Sayedahmed K, El Shazly M, Olianas R, Kaftan B, Omar M. The outcome of Y-V plasty as a final option in patients with recurrent bladder neck sclerosis following failed endoscopic treatment. Cent European J Urol 2019; 72:408-12.
doi: 10.5173/ceju.2019.1977
pmid: 32015912