Proposal and clinical validation of a perioperative algorithm enhancing antimicrobial stewardship in substitution urethroplasty
Phillip Marksa,Benedikt Kranzbühlerab,Luis A. Kluthc,Christian P. Meyerd,Clemens M. Rosenbaume,Tim A. Ludwiga,Liucheng Dingaf,Lennart Kühnkea,Frederik Königa,Roland Dahlema,Margit Fischa,Malte W. Vetterleina*(),on behalf of the Trauma and Reconstructive Urology Working Party of the European Association of Urology Young Academic Urologists
aDepartment of Urology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany bDepartment of Urology, University Hospital Zürich, Zürich, Switzerland cDepartment of Urology, University Hospital Frankfurt am Main, Frankfurt am Main, Germany dDepartment of Urology, Ruhr-University Bochum, Campus OWL, Herford, Germany eDepartment of Urology, Asklepios Hospital Barmbek, Hamburg, Germany fDepartment of Urology, The Second Affiliated Hospital of Nanjing Medical University, Nanjing, China
Objective: To evaluate the impact of a standardized antibiotic stewardship protocol on three subsequent endpoints in patients undergoing urethroplasty.
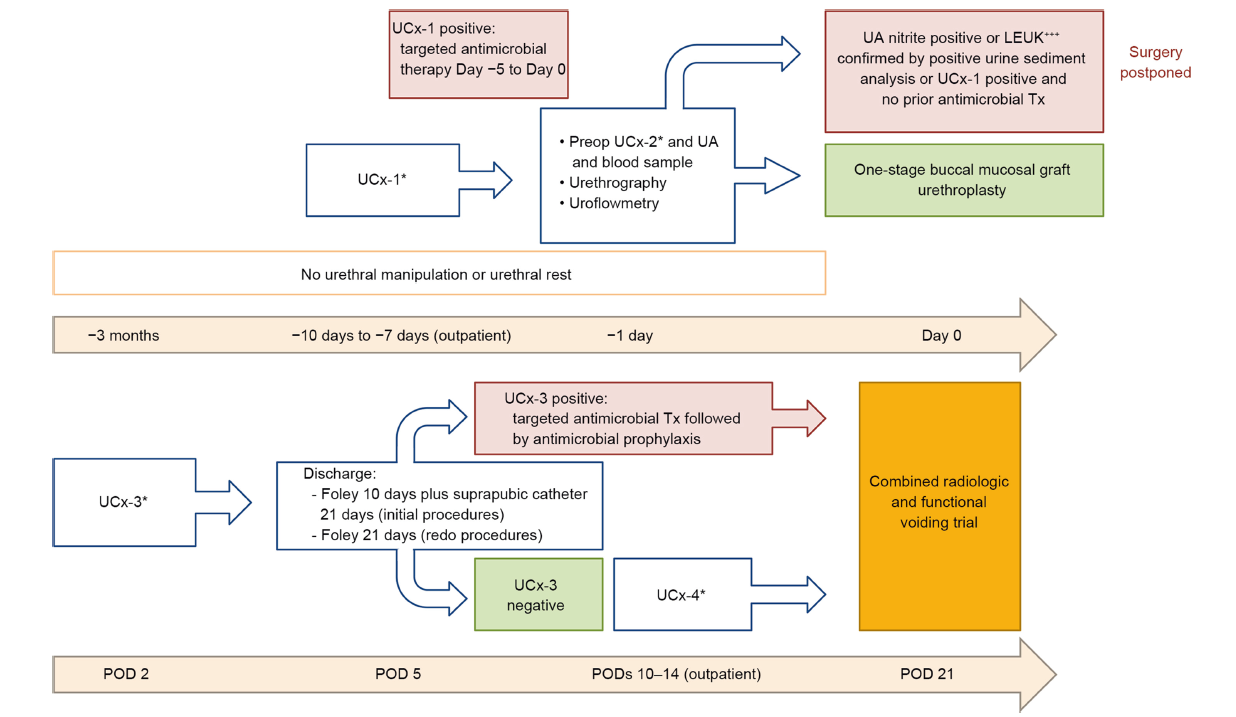
Methods: Men undergoing bulbar substitution urethroplasty between January 2009 and December 2016 were stratified by urine culture (UCx) at the time of surgery (sterile vs. non-sterile) and were subjected to a standardized algorithm for urinalysis and antimicrobial therapy. We performed quantitative and qualitative exploration of UCx results and the microbial spectrum. The ability of the algorithm to improve antibiotic stewardship was tested by three endpoints: (a) immediate (UCx 2 days postoperatively), (b) short-term (21-day infectious complications), and (c) long-term (retreatment-free survival [RFS]). Statistical analyses included bivariate comparisons. The Kaplan-Meier estimators were used to compare RFS between the groups. The multivariable Cox regression was used to evaluate the independent effect of UCx status at the time of surgery on RFS.
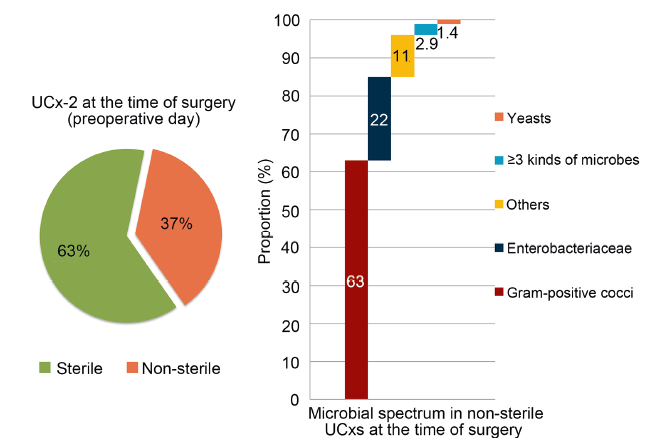
Results: Of 374 men, 235 (63%) had a sterile and 139 (37%) a non-sterile culture at the time of surgery. The proportion of sterile cultures at the time of surgery (63%) was significantly improved to 82% 2 days postoperatively (p<0.001). There were 16 (4.3%) patients with infectious complications with no difference between patients with sterile versus non-sterile culture (p=0.6). At median follow-up of 29 months, there was no difference in RFS (84%) between patients with sterile versus non-sterile culture (p=0.3). Positive UCx was not a predictor of recurrence after multivariable adjustment (p=0.5).
Conclusion: A standardized protocol such as the one introduced improves antibiotic stewardship through frequent testing and culture-specific treatment. This is crucial in avoiding unnecessary antimicrobial treatment, and reducing infectious events and adverse effects of a positive UCx on long-term stricture recurrence.
. [J]. Asian Journal of Urology, 2024, 11(4): 604-610.
Phillip Marks, Benedikt Kranzbühler, Luis A. Kluth, Christian P. Meyer, Clemens M. Rosenbaum, Tim A. Ludwig, Liucheng Ding, Lennart Kühnke, Frederik König, Roland Dahlem, Margit Fisch, Malte W. Vetterlein, on behalf of the Trauma and Reconstructive Urology Working Party of the European Association of Urology Young Academic Urologists. Proposal and clinical validation of a perioperative algorithm enhancing antimicrobial stewardship in substitution urethroplasty. Asian Journal of Urology, 2024, 11(4): 604-610.
Santucci RA, Joyce GF, Wise M. Male urethral stricture disease. J Urol 2007; 177:1667-74.
doi: 10.1016/j.juro.2007.01.041
pmid: 17437780
[2]
Lumen N, Campos-Juanatey F, Greenwell T, Martins FE, Osman NI, Riechardt S, et al. European Association of Urology guidelines on urethral stricture disease (part 1): management of male urethral stricture disease. Eur Urol 2021; 80:190-200.
doi: 10.1016/j.eururo.2021.05.022
pmid: 34059397
[3]
Wessells H, Morey A, Souter L, Rahimi L, Vanni A. Urethral stricture disease guideline amendment (2023). J Urol 2023; 210:64-71.
[4]
Campos-Juanatey F, Osman NI, Greenwell T, Martins FE, Riechardt S, Waterloos M, et al. European Association of Urology guidelines on urethral stricture disease (part 2): diagnosis, perioperative management, and follow-up in males. Eur Urol 2021; 80:201-12.
doi: 10.1016/j.eururo.2021.05.032
pmid: 34103180
[5]
McDonald ML, Buckley J. Antimicrobial practice patterns for urethroplasty: opportunity for improved stewardship. Urology 2016; 94:237-45.
doi: 10.1016/j.urology.2016.03.051
pmid: 27138266
[6]
Hoare DT, Doiron RC, Rourke KF. Determining perioperative practice patterns in urethroplasty: a survey of genitourinary reconstructive surgeons. Urology 2021; 156:263-70.
doi: 10.1016/j.urology.2021.05.067
pmid: 34186137
[7]
Maffucci F, Chang C, Simhan J, Cohn JA. Is there any benefit to the use of antibiotics with indwelling catheters after urologic surgery in adults. Antibiotics (Basel) 2023; 12:156. https://doi.org/10.3390/antibiotics12010156.
[8]
Bia?ek ?, Rydzińska M, VetterleinMW, Dobruch J, Skrzypczyk MA; Trauma and Reconstructive Urology Working Party of the European Association of Urology Young Academic Urologists. A systematic review on postoperative antibiotic prophylaxis after pediatric and adult male urethral reconstruction. J Clin Med 2023; 12:6162. https://doi.org/10.3390/jcm12196162.
[9]
Kim S, Cheng KC, Alsikafi NF, Breyer BN, Broghammer JA, Elliott SP, et al. Minimizing antibiotic use in urethral reconstruction. J Urol 2022; 208:128-34.
[10]
Baas W, Parker A, Radadia K, Ogawa S, Vetter J, Paradis A, et al. Antibiotic duration after urethroplasty: an attempt at improving antibiotic stewardship. Urology 2021; 158:228-31.
doi: 10.1016/j.urology.2021.07.028
pmid: 34380052
[11]
Manjunath A, Chen L, Welty LJ, Wong VJ, Amarasekera C, Gonzalez CM, et al. Antibiotic prophylaxis after urethroplasty may offer no benefit. World J Urol 2020; 38:1295-301.
doi: 10.1007/s00345-019-02880-x
pmid: 31332512
[12]
Kim S, Cheng KC, Patell S, Alsikafi NF, Breyer BN, Broghammer JA, et al. Antibiotic stewardship and postoperative infections in urethroplasties. Urology 2021; 152:142-7.
doi: 10.1016/j.urology.2020.10.065
pmid: 33373707
[13]
Fichtner J, Filipas D, Fisch M, Hohenfellner R, Thuroff JW. Longterm outcome of ventral buccal mucosa onlay graft urethroplasty for urethral stricture repair. Urology 2004; 64:648-50.
doi: 10.1016/j.urology.2004.05.011
pmid: 15491691
[14]
Vetterlein MW, Loewe C, Zumstein V, Rosenbaum CM, Engel O, Dahlem R, et al. Characterization of a standardized postoperative radiographic and functional voiding trial after 1- stage bulbar ventral onlay buccal mucosal graft urethroplasty and the impact on stricture recurrence-free survival. J Urol 2019; 201:563-72.
doi: 10.1016/j.juro.2018.09.041
pmid: 30240692
[15]
Vetterlein MW, Stahlberg J, Zumstein V, Engel O, Dahlem R, Fisch M, et al. The impact of surgical sequence on stricture recurrence after anterior 1-stage buccal mucosal graft urethroplasty: comparative effectiveness of initial, repeat and secondary procedures. J Urol 2018; 200:1308-14.
doi: S0022-5347(18)43470-2
pmid: 30126826
[16]
Anderson KT, Vanni AJ, Erickson BA, Myers JB, Voelzke B, Breyer BN, et al. Defining success after anterior urethroplasty: an argument for a universal definition and surveillance protocol. J Urol 2022; 208:135-43.
[17]
Dellit TH, Owens RC, McGowan JE Jr, Gerding DN, Weinstein RA, Burke JP, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis 2007; 44:159-77.
doi: 10.1086/510393
pmid: 17173212
[18]
Schuts EC, Hulscher M, Mouton JW, Verduin CM, Stuart J, Overdiek H, et al. Current evidence on hospital antimicrobial stewardship objectives: a systematic review and meta-analysis. Lancet Infect Dis 2016; 16:847-56.
doi: S1473-3099(16)00065-7
pmid: 26947617
[19]
Cai T, Mazzoli S, Mondaini N, Meacci F, Nesi G, D’Elia C, et al. The role of asymptomatic bacteriuria in young women with recurrent urinary tract infections: to treat or not to treat? Clin Infect Dis 2012; 55:771-7.
doi: 10.1093/cid/cis534
pmid: 22677710
[20]
Bonkat G, Bartoletti R, Bruyère F, Cai T, Geerlings SE, K?ves B, et al. EAU guidelines on urological infections. 2023. https://uroweb.org/guidelines/urological-infections. [Accessed 28 June 2023].
[21]
Hanasaki T, Kanematsu A, Yamamoto S. Proactive discontinuation of postoperative antibiotic prophylaxis after urethroplasty. Int J Urol 2022; 29:707-11.
doi: 10.1111/iju.14878
pmid: 35362117
[22]
Kim S, Cheng KC, Alsikafi NF, Breyer BN, Broghammer JA, Elliott SP, et al. Minimizing antibiotic use in urethral reconstruction. J Urol 2022; 208:128-34.
[23]
Bischoff S, Walter T, Gerigk M, Ebert M, Vogelmann R. Empiric antibiotic therapy in urinary tract infection in patients with risk factors for antibiotic resistance in a German emergency department. BMC Infect Dis 2018; 18:56. https://doi.org/10.1186/s12879-018-2960-9.
doi: 10.1186/s12879-018-2960-9
pmid: 29373965
Luis G. Medina, Randall A. Lee, Valeria Celis, Veronica Rodriguez, Jaime Poncel, Aref S. Sayegh, Rene Sotelo. Robotic management of urinary fistula[J]. Asian Journal of Urology, 2024, 11(3): 357
-365
.