Genitourinary toxicity after pelvic radiation: Prospective review of complex urological presentations
Rowan V. Davidab*(),Asif Islama,John Millera,Michael E. O'Callaghanab,Arman A. Kahokehrab
aDepartment of Urology, Lyell McEwin Hospital, Elizabeth Vale, Adelaide, Australia bCollege of Medicine and Public Health, Flinders University, Bedford Park South Australia, Adelaide, Australia
Objective: Recent randomised controlled trials underestimated the incidence of genitourinary (GU) complications occurring more than 5 years following pelvic radiotherapy. This study aimed to determine the burden of treatment at a single institution from late GU complications after pelvic radiotherapy.
Methods: A prospective study of all presentations for GU complications following pelvic radiotherapy at a tertiary urology department between November 2018 and November 2019 was performed. Subgroup analyses was performed on patients with prostate cancer (PCa) with late toxicity to compare patient demographics, radiotherapy, complications, and management factors.
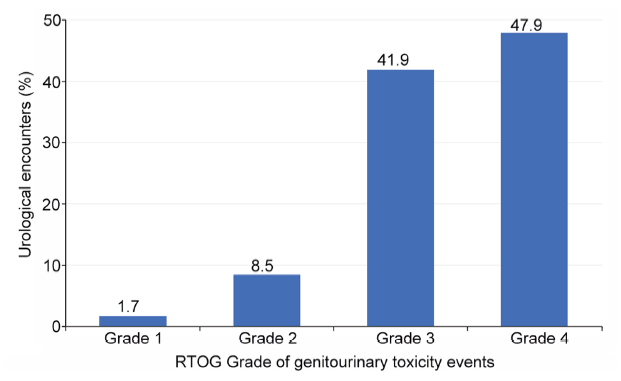
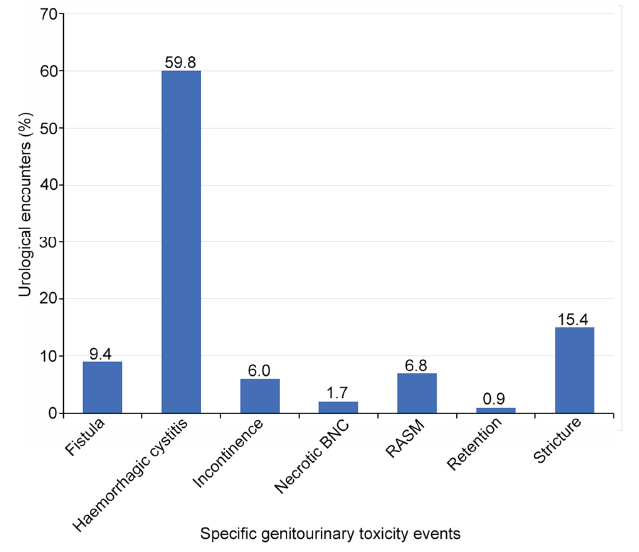
Results: There were 117 hospital encounters involving 46 patients with a 56.4% repeat encounter rate. Patients with PCa were the predominant group (n=39, 84.8%). External beam radiotherapy was the most common treatment modality (n=41, 89.1%). The median time from radiotherapy to encounter was 8 (range 0-23) years. Radiation-induced haemorrhagic cystitis was the most common presentation (n=70, 59.8%). Forty-four (42.7%) encounters for GU toxicity were managed operatively and 33 (32.0%) involved a non-operative procedure. Nine patients required packed red cell transfusion, with a total of 154 units transfused. Patients with PCa who presented with late GU toxicity had higher median Radiotherapy Oncology Group grades (p=0.020), proportion of emergency admissions (p=0.047), and frequency of clot urinary retention (p<0.001).
Conclusion: There is a high burden of elective and emergency urology workload attributed to late pelvic radiation toxicity. Late GU toxicity occurring ≥5 years after radiotherapy is common and often more severe.
. [J]. Asian Journal of Urology, 2024, 11(4): 633-641.
Rowan V. David, Asif Islam, John Miller, Michael E. O'Callaghan, Arman A. Kahokehr. Genitourinary toxicity after pelvic radiation: Prospective review of complex urological presentations. Asian Journal of Urology, 2024, 11(4): 633-641.
Sheets NC, Goldin GH, Meyer AM, Wu Y, Chang Y, Sturmer T, et al. Intensity-modulated radiation therapy, proton therapy, or conformal radiation therapy and morbidity and disease control in localized prostate cancer. JAMA 2012; 307:1611-20.
doi: 10.1001/jama.2012.460
pmid: 22511689
[2]
Bekelman JE, Mitra N, Efstathiou J, Liao K, Sunderland R, Yeboa DN, et al. Comparative effectiveness of intensity modulated (IMRT) versus 3D conformal (CRT) radiotherapy for non-metastatic prostate cancer. Int J Radiat Oncol Biol Phys 2010; 78:S77. https://doi.org/10.1016/j.ijrobp.2010.07.211.
[3]
de la Taille A, Zerbib M. [Urologic complications of radiotherapy]. Ann Urol 2003; 37:345-57. [Article in French].
pmid: 14717037
[4]
Wallis CJD, Glaser A, Hu JC, Huland H, Lawrentschuk N, Moon D, et al. Survival and complications following surgery and radiation for localized prostate cancer: an international collaborative review. Eur Urol 2018; 73:11-20.
doi: S0302-2838(17)30495-5
pmid: 28610779
[5]
Boysen WR, Inouye B, Peterson AC. Admissions for radiation cystitis are increasing among cancer survivors in the United States: analysis of the health care cost and utilization project (HCUP). J Urol 2020; 203(Suppl 4):e600-1. https://doi.org/10.1097/JU.0000000000000890.015.
[6]
Bekelman JE, Mitra N, Efstathiou J, Liao K, Sunderland R, Yeboa DN, et al. Outcomes after intensity-modulated versus conformal radiotherapy in older men with nonmetastatic prostate cancer. Int J Radiat Oncol Biol Phys 2011; 81:e325-34. https://doi.org/10.1016/j.ijrobp.2011.02.006.
[7]
Wilt TJ, MacDonald R, Rutks I, Shamliyan TA, Taylor BC, Kane RL. Systematic review: comparative effectiveness and harms of treatments for clinically localized prostate cancer. Ann Intern Med 2008; 148:435-48.
doi: 10.7326/0003-4819-148-6-200803180-00209
pmid: 18252677
[8]
Hummel S, Paisley S, Morgan A, Currie E, Brewer N. Clinical and cost-effectiveness of new and emerging technologies for early localised prostate cancer: a systematic review. Health Technol Assess 2003; 7(iii, ixex):1-157. https://doi.org/10.3310/hta7330.
[9]
Bentzen SM. Randomized controlled trials in health technology assessment: overkill or overdue? Radiother Oncol 2008; 86:142-7.
doi: 10.1016/j.radonc.2008.01.012
pmid: 18237799
[10]
Ma JL, Hennessey DB, Newell BP, Bolton DM, Lawrentschuk N. Radiotherapy-related complications presenting to a urology department: a more common problem than previously thought? BJU Int 2018; 121:28-32.
[11]
Kneebone A, Gysen KV. Is radiotherapy the work of the devil? BJU Int 2018; 121:6-7.
[12]
Hoffmann R, Islam A, Kahokehr A. Radiation cystitis and burden of careda snapshot study. BJU Int 2019; 123(S2): 50. https://doi.org/10.1111/bju.14724.
[13]
Choi EC, Kim YB, Kim JY, Kim YS, Chun M, Park W, et al. Risk factors of radiation-related secondary malignancy in pelvis after radiotherapy for cervical cancer: multi-institutional study in korea. Int J Radiat Oncol Biol Phys 2017; 99:E287. https://doi.org/10.1016/j.ijrobp.2017.06.1287.
[14]
Gladdy RA, Qin LX, Moraco N, Edgar MA, Antonescu CR, Alektiar KM, et al. Do radiation-associated soft tissue sarcomas have the same prognosis as sporadic soft tissue sarcomas? J Clin Oncol 2010; 28:2064-9.
doi: 10.1200/JCO.2009.25.1728
pmid: 20308666
[15]
Cox JD, Stetz J, Pajak TF. Toxicity criteria of the radiation therapy oncology group (RTOG) and the European organization for research and treatment of cancer (EORTC). Int J Radiat Oncol Biol Phys 1995; 31:1341-6.
[16]
Handmer M, Martin J, Tiu A. Costing urologic complications following pelvic radiation therapy. Urology 2020; 140:64-9.
doi: S0090-4295(20)30270-3
pmid: 32194089
[17]
Mazzone E, Mistretta FA, Knipper S, Palumbo C, Tian Z, Pecoraro A, et al. Long-term incidence of secondary bladder and rectal cancer in patients treated with brachytherapy for localized prostate cancer: a large-scale population-based analysis. BJU Int 2019; 124:1006-13.
doi: 10.1111/bju.14841
pmid: 31144770
[18]
Zelefsky MJ, Pei X, Teslova T, Kuk D, Magsanoc JM, Kollmeier M, et al. Secondary cancers after intensitymodulated radiotherapy, brachytherapy and radical prostatectomy for the treatment of prostate cancer: incidence and cause-specific survival outcomes according to the initial treatment intervention. BJU Int 2012; 110:1696-701.
doi: 10.1111/j.1464-410X.2012.11385.x
pmid: 22889401
[19]
Moschini M, Zaffuto E, Karakiewicz PI, Andrea DD, Foerster B, Abufaraj M, et al. External beam radiotherapy increases the risk of bladder cancer when compared with radical prostatectomy in patients affected by prostate cancer: a population-based analysis. Eur Urol 2019; 75:319-28.
doi: S0302-2838(18)30722-X
pmid: 30293908
[20]
Michalski JM, Yan Y, Watkins-Bruner D, Bosch WR, Winter K, Galvin JM, et al. Preliminary toxicity analysis of 3-dimensional conformal radiation therapy versus intensity modulated radiation therapy on the high-dose arm of the Radiation Therapy Oncology Group 0126 prostate cancer trial. Int J Radiat Oncol Biol Phys 2013; 87:932-8.
[21]
Koper PC, Stroom JC, van Putten WL, Korevaar GA, Heijmen BJ, Wijnmaalen A, et al. Acute morbidity reduction using 3DCRT for prostate carcinoma: a randomized study. Int J Radiat Oncol Biol Phys 1999; 43:727-34.
[22]
Morris DE, Emami B, Mauch PM, Konski AA, Tao ML, Ng AK, et al. Evidence-based review of three-dimensional conformal radiotherapy for localized prostate cancer: an ASTRO outcomes initiative. Int J Radiat Oncol Biol Phys 2005; 62:3-19.
Luis G. Medina, Randall A. Lee, Valeria Celis, Veronica Rodriguez, Jaime Poncel, Aref S. Sayegh, Rene Sotelo. Robotic management of urinary fistula[J]. Asian Journal of Urology, 2024, 11(3): 357
-365
.