aDepartment of Urology, Xiangya Hospital, Central South University, Changsha, China bNational Clinical Research Center for Geriatric Disorders, Xiangya Hospital, Central South University, Changsha, China
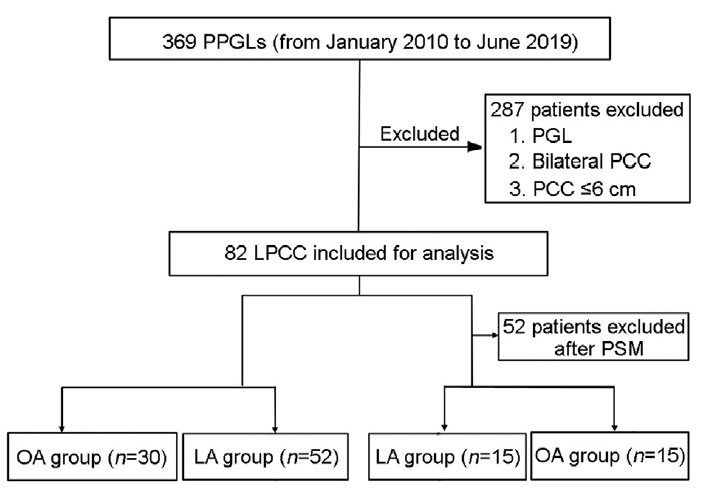
Objective: Clinical practice guidelines recommend open adrenalectomy (OA) for large pheochromocytoma (LPCC) > 6 cm in size. Although laparoscopic adrenalectomy (LA) for the treatment of LPCC has been reported, its role remains unclear. This study aimed to compare the effectiveness of LA and OA, and summary the surgical treatment experience. Methods: Data concerning LPCC, from January 2010 to June 2019 of a single institution, were retrospectively reviewed. Altogether 82 patients with a tumor larger than 6 cm were included (52 patients in LA group and 30 patients in OA group). Groups were balanced by propensity score matching (PSM) into 15 pairs. Patients’ demographics, preoperative characteristics, and prognosis were analyzed. Results: Before PSM, the OA group had larger tumor sizes (median [interquartile range, IQR]: 8.9 [7.3-10.3] vs. 7.2 [6.7-8.0] cm; p=0.000) and higher vanillylmandelic acid level (median [IQR]: 114.3 [67.8-326.4] vs. 66.6 [37.8-145.8] μmol/24 h; p =0.004) and needed a higher cumulative dose of prazosin (median [IQR]: 83.5 [37.0-154.0] vs. 38.0 [21.0-81.0] mg; p=0.028). After PSM, the baseline data showed no significant differences between both groups. The LA group had relatively more stable blood pressure in surgery, with a lower fluctuation of systolic blood pressure (mean±standard deviation [SD]: 70.9±25.1 vs. 107.4±46.2 mmHg, p=0.012) and a lower percentage of hemodynamic instability (46.7% vs. 86.7%, p=0.020). The LA group had shorter postoperative hospital stays (mean±SD: 6.4±2.7 vs. 10.1±3.4 days; p=0.003) than the OA group. Differences regarding metastasis rate (6.7% vs. 0, p=1.000) were not statistically significant between LA and OA groups. The median (IQR) follow-up time of 82 patients was 72.5 (47.0-103.5) months. Binary logistic regression showed that right-side tumors or those >8 cm in size were independent risk factors of OA. Conclusion: LA is a safe, minimally invasive procedure for LPCC and has relatively better perioperative characteristics in large medical centers. Patients with tumors on the right side or larger than 8 cm are more likely to undergo OA initially.
Nozaki T, Iida H, Morii A, Fujiuchi Y, Okumura A, Fuse H. Laparoscopic resection of adrenal and extra-adrenal pheochromocytoma. J Endourol 2013; 27:862e8.
doi: 10.1089/end.2012.0745
[2]
Neumann HPH, Young Jr WF, Eng C. Pheochromocytoma and Paraganglioma. N Engl J Med 2019; 381:552e65.
doi: 10.1056/NEJMra1806651
[3]
LiM, Wang C, Liu P, Qi L, Chen X, Fan B, et al. Clinical and genetic features of pediatric PCCs/PGLs patients: a single-center experience in China. Transl Androl Urol 2020; 9:267e75.
doi: 10.21037/tau.2020.02.14
[4]
Castinetti F, De Freminville JB, Guerin C, Cornu E, Sarlon G, Amar L. Controversies about the systematic preoperative pharmacological treatment before pheochromocytoma or paraganglioma surgery. Eur J Endocrinol 2022; 186:D17e24. https://doi.org/10.1530/EJE-21-0692.
doi: 10.1530/EJE-21-0692
pmid: 35230260
[5]
Zawadzka K, Wieckowski K, Malczak P, Wysocki M, Major P, Pedziwiatr M, et al. Selective vs. non-selective alpha-blockade prior to adrenalectomy for pheochromocytoma: systematic review and meta-analysis. Eur J Endocrinol 2021; 184:751e60.
doi: 10.1530/EJE-20-1301
[6]
Nguyen DN, Qureshi JM, Singh H, Tran CD, Cothron K. Large malignant pheochromocytoma causing cardiac failure and metastasis:a case report with review of literature. Curr Probl Diagn Radiol 2021; 50:961e6.
[7]
Ma L, Shen L, Zhang X, Huang Y. Predictors of hemodynamic instability in patients with pheochromocytoma and paraganglioma. J Surg Oncol 2020; 122:803e8.
doi: 10.1002/jso.26079
[8]
Zhu W, Wang S, Du G, Liu H, Lu J, Yang W. Comparison of retroperitoneal laparoscopic versus open adrenalectomy for large pheochromocytoma: a single-center retrospective study. World J Surg Oncol 2019; 17:111. https://doi.org/10.1186/s12957-019-1649-x.
doi: 10.1186/s12957-019-1649-x
[9]
Shiraishi K, Kitahara S, Ito H, Oba K, Ohmi C, Matsuyama H. Transperitoneal versus retroperitoneal laparoscopic adrenalectomy for large pheochromocytoma: comparative outcomes. Int J Urol 2019; 26:212e6.
doi: 10.1111/iju.13838
pmid: 30430653
[10]
Calissendorff J, Juhlin CC, Bancos I, Falhammar H. Pheochromocytomas and abdominal paragangliomas: a practical guidance. Cancers 2022; 14:917. https://doi.org/10.3390/cancers14040917.
doi: 10.3390/cancers14040917
[11]
Lenders JW, Duh QY, Eisenhofer G, Gimenez-Roqueplo AP, Grebe SK, Murad MH, et al. Pheochromocytoma and paraganglioma: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 2014; 99: 1915e42.
[12]
Dimas S, Roukounakis N, Kafetzis I, Bethanis S, Anthi S, Michas S, et al. Feasibility of laparoscopic adrenalectomy for large pheochromocytomas. J Soc Laparoendosc Surg 2007; 11:30e3.
[13]
Indupur RR, Nerli RB, Reddy MN, Siddappa SN, Thakkar R. Laparoscopic adrenalectomy for large pheochromocytoma. BJU Int 2007; 100:1126e9.
pmid: 17784884
[14]
Ippolito G, Palazzo FF, Sebag F, Thakur A, Cherenko M, Henry JF. Safety of laparoscopic adrenalectomy in patients with large pheochromocytomas: a single institution review. World J Surg 2008; 32:840e4; discussion 5e6.
doi: 10.1007/s00268-007-9327-5
[15]
Perry KA, El Youssef R, Pham TH, Sheppard BC. Laparoscopic adrenalectomy for large unilateral pheochromocytoma: experience in a large academic medical center. Surg Endosc 2010; 24:1462e7.
doi: 10.1007/s00464-009-0801-z
pmid: 20033709
[16]
Agarwal G, Sadacharan D, Aggarwal V, Chand G, Mishra A, Agarwal A, et al. Surgical management of organ-contained unilateral pheochromocytoma: comparative outcomes of laparoscopic and conventional open surgical procedures in a large single-institution series. Langenbecks Arch Surg 2012; 397:1109e16.
doi: 10.1007/s00423-011-0879-3
[17]
Conzo G, Musella M, Corcione F, De Palma M, Avenia N, Milone M, et al. Laparoscopic treatment of pheochromocytomas smaller or larger than 6 cm. A clinical retrospective study on 44 patients. Laparoscopic adrenalectomy for pheochromocytoma. Ann Ital Chir 2013; 84:417e22.
[18]
Aggeli C, Nixon AM, Parianos C, Vletsis G, Papanastasiou L, Markou A, et al. Surgery for pheochromocytoma: a 20-year experience of a single institution. Hormones (Basel) 2017; 16: 388e95.
[19]
Conzo G, Gambardella C, Candela G, Sanguinetti A, Polistena A, Clarizia G, et al. Single center experience with laparoscopic adrenalectomy on a large clinical series. BMC Surg 2018; 18:2. https://doi.org/10.1186/s12893-017-0333-8.
doi: 10.1186/s12893-017-0333-8
[20]
Wang W, Li P, Wang Y, Wang Y, Ma Z, Wang G, et al. Effectiveness and safety of laparoscopic adrenalectomy of large pheochromocytoma: a prospective, nonrandomized, controlled study. Am J Surg 2015; 210:230e5.
doi: 10.1016/j.amjsurg.2014.11.012
[21]
Bai S, Yao Z, Zhu X, Li Z, Jiang Y, Wang R, et al. Comparison of transperitoneal laparoscopic versus open adrenalectomy for large pheochromocytoma: a retrospective propensity scorematched cohort study. Int J Surg 2019; 61:26e32.
doi: 10.1016/j.ijsu.2018.11.018
[22]
Li J, Wang Y, Chang X, Han Z. Laparoscopic adrenalectomy (LA) vs. open adrenalectomy (OA) for pheochromocytoma (PHEO): a systematic review and meta-analysis. Eur J Surg Oncol 2020; 46:991e8.
doi: 10.1016/j.ejso.2020.02.009
[23]
Scholten A, Vriens MR, Cromheecke GJ, Borel Rinkes IH, Valk GD. Hemodynamic instability during resection of pheochromocytoma in MEN versus non-MEN patients. Eur J Endocrinol 2011; 165:91e6.
doi: 10.1530/EJE-11-0148
pmid: 21498631
[24]
Korevaar TI, Grossman AB. Pheochromocytomas and paragangliomas: assessment of malignant potential. Endocrine 2011; 40:354e65.
doi: 10.1007/s12020-011-9545-3
pmid: 22038451
[25]
Wang Y, Li M, Deng H, Pang Y, Liu L, Guan X. The systems of metastatic potential prediction in pheochromocytoma and paraganglioma. Am J Cancer Res 2020; 10:769e80.
[26]
Gunseren KO, Cicek MC, Vuruskan H, Kordan Y, Yavascaoglu I. Challenging risk factors for right and left laparoscopic adrenalectomy: a single centre experience with 272 cases. Int Braz J Urol 2019; 45:747e53.
doi: 10.1590/S1677-5538.IBJU.2019.0131
pmid: 31136115
[27]
Rieder JM, Nisbet AA, Wuerstle MC, Tran VQ, Kwon EO, Chien GW. Differences in left and right laparoscopic adrenalectomy. J Soc Laparoendosc Surg 2010; 14:369e73.
doi: 10.4293/108680810X12924466007520
[28]
Kokorak L, Soltes M, Vladovic P, Marko L. Laparoscopic left and right adrenalectomy from an anterior approachdis there any difference? Outcomes in 176 consecutive patients. Wideochir Inne Tech Maloinwazyjne 2016; 11:268e73.
[29]
Chung HS, Kim MS, Yu HS, Hwang EC, Kim SO, Oh KJ, et al. Laparoscopic adrenalectomy using the lateral retroperitoneal approach: is it a safe and feasible treatment option for pheochromocytomas larger than 6 cm? Int J Urol 2018; 25:414e9.
doi: 10.1111/iju.13524
pmid: 29478297
[30]
Vidal O, Saavedra-Perez D, Martos JM, de la Quintana A, Rodriguez JI, Villar J, et al. Risk factors for open conversion of lateral transperitoneal laparoscopic adrenalectomy: retrospective cohort study of the Spanish Adrenal Surgery Group (SASG). Surg Endosc 2020; 34:3690e5.
doi: 10.1007/s00464-019-07264-1