The role of quick Sepsis-related Organ Failure Assessment score as simple scoring system to predict Fournier gangrene mortality and the correlation with Fournier's Gangrene Severity Index: Analysis of 69 patients
Bambang S. Noegroho*(),Kuncoro Adi,Akhmad Mustafa*(),Rais Syaeful Haq,Zola Wijayanti,Jason Liarto
Urology Department, Hasan Sadikin Academic Medical Center, Universitas Padjadjaran, Bandung, Indonesia
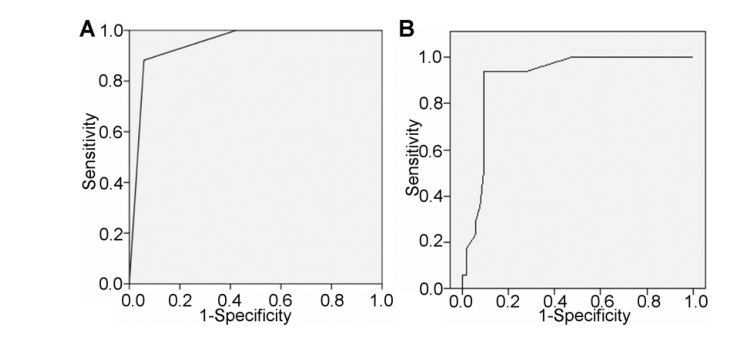
Objective: Fournier's gangrene is a rare but life-threatening infection disease with high mortality rate. The quick Sepsis-related Organ Failure Assessment (qSOFA) is a new and simpler scoring system that may identify patients with suspected infection who are at greater risk for a poor outcome. The purpose of this study was to find out role of qSOFA in determining prognosis of Fournier's gangrene patients. Methods: This study is a case control with retrospective review of Fournier's gangrene patients treated at Hasan Sadikin Hospital from January 2013 to December 2017 who met inclusion criteria. Participants were divided into two groups according to qSOFA score as high qSOFA (2-3) and low qSOFA (0-1). Results: From 69 patients, the mortality rate was 24.6%. The sensitivity of qSOFA score to predict mortality was 88.2%; the specificity was 94.2%; positive predictive value was 83.3%; negative predictive value was 96.1%; positive likelihood ratio was 15.2; negative likelihood ratio was 0.12; and the area under the receiver operating characteristic curve of qSOFA was 94.2%. There was significant association between qSOFA scale and mortality with p-value of 0.0001. The qSOFA score has strong positive correlation with Fournier's Gangrene Severity Index (p<0.0001, r=0.704). Conclusion: qSOFA scoring system has a high prognostic value and can be used to determine prognosis of Fournier's gangrene patients.
. [J]. Asian Journal of Urology, 2023, 10(2): 201-207.
Bambang S. Noegroho,Kuncoro Adi,Akhmad Mustafa,Rais Syaeful Haq,Zola Wijayanti,Jason Liarto. The role of quick Sepsis-related Organ Failure Assessment score as simple scoring system to predict Fournier gangrene mortality and the correlation with Fournier's Gangrene Severity Index: Analysis of 69 patients. Asian Journal of Urology, 2023, 10(2): 201-207.
Respiratory rate, mean±SD, number of breaths per minute
21.27±2.88
26.94±5.34
0.001a
Comorbidity, n (%)
Chronic kidney disease
2 (3.8)
5 (29.4)
0.067c
Heart failure
3 (5.8)
3 (17.6)
0.101c
Diabetes
21 (40.4)
7 (41.2)
0.954c
Tuberculosis
2 (3.8)
0 (0)
0.412c
HIV
1 (1.9)
1 (5.9)
0.398c
Autoimmune
1 (1.9)
0 (0)
0.565c
Perianal abscess
16 (30.8)
9 (52.9)
0.099c
Carbuncle
19 (36.5)
6 (35.3)
0.926c
Urethral stricture
13 (25.0)
1 (5.9)
0.089c
Laboratory result, mean±SD
Hb, g/dL
11.47±3.11
10.52±2.99
0.262a
Leucocyte, number per mm3
17 423.14±9129.00
19 003.23±9696.00
0.545a
Thrombocyte, number per mm3
384 921.57±175 107.00
266 937.50±153 547.00
0.018a
Sodium, mEq/L
130.61±5.99
128.06±8.26
0.176a
Potassium, mmol/L
4.69±4.836
4.41±1.121
0.809a
BUN, mg/dL
67.43±59.94
92.94±49.98
0.095a
Creatinine, mg/dL
2.19±2.77
2.09±1.16
0.833a
HCO3?, mEq/L
22.70±13.48
26.68±12.27
0.136a
Random blood glucose, mg/dL
177.36±138.80
162.46±100.43
0.671a
Albumin, g/dL
2.383±0.894
1.730±0.404
0.017a
FGSI score, n (%)
<9
47 (90.4)
1 (5.9)
0.0001b
≥9
5 (9.6)
16 (94.1)
qSOFA score, n (%)
Low risk (0-1)
49 (94.2)
2 (11.8)
0.0001b
High risk (2-3)
3 (5.8)
15 (88.2)
Variable
qSOFA
FGSI
r-Value
p-Valuea
Sensitivity
88.2%
94.1%
0.704
0.0001
Specificity
94.2%
90.3%
Positive predictive value
83.3%
76.1%
Negative predictive value
96.1%
97.9%
Positive likelihood ratio
15.2
9.7
Negative likelihood ratio
0.12
0.065
Area under the curve
94.2%
91.2%
Author
Year
Location
Data collection duration, year
Number of patients (number of patients per year)
Mortality rate, %
Laor et al. [5]
1995
USA
15
30 (2)
43.3
Yilmazlar et al. [7]
2010
Turkey
16
120 (7)
20.5
Shukla et al. [11]
2016
India
4
57 (14)
22.5
Noegroho et al. [10]
2021
Turkey
16
120 (7)
20.5
Benjelloun et al. [12]
2013
Morocco
7
50 (7)
24.0
Yeniyol et al. [13]
2004
Turkey
5
25 (5)
24.0
Hejase et al. [14]
1996
Mexico
3
38 (3)
2.6
Tahmaz et al. [15]
2006
Turkey
15
33 (2)
6.0
Sallami et al. [31]
2012
Tunisia
15
40 (3)
17.5
McCormack et al. [32]
2015
Canada
12
26 (2)
19.2
Sánchez Mazzaferri et al. [33]
1999
Spain
10
9 (1)
22.5
[1]
Thwaini A, Khan A, Malik A, Cherian J, Barua J, Shergill I, et al. Fournier’s gangrene and its emergency management. Postgrad Med J 2006; 82:516-9.
doi: 10.1136/pgmj.2005.042069
pmid: 16891442
[2]
Heyns CF, Theron PD. Fournier’s gangrene. In: Hohenfellner M, Santucci RA, editors. Emergencies in urology. Berlin: Springer; 2007. p50-9.
[3]
Grabe M, Bartoletti R, Johansen TEB, Cai T, Cek M, Koves B, et al. Guidelines on urological infections. European Association of Urology Guidelines; 2017. https://uroweb.org/ guideline/urological-infections/.[Accessed 26 August 2020].
[4]
Singh A, Ahmed K, Aydin A, Khan MS, Dasgupta P. Fournier’s gangrene. A clinical review. Arch Ital Urol Androl 2016; 88: 157-64.
doi: 10.4081/aiua.2016.3.157
[5]
Laor E, Palmer LS, Tolia BM, Reid RE, Winter HI. Outcome prediction in patients with Fournier’s Gangrene. J Urol 1995; 154:89-92.
pmid: 7776464
[6]
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification. Crit Care Med 1985; 13: 818-29.
pmid: 3928249
[7]
Yilmazlar T, Ozturk E, Ozguc H, Ercan I, Vuruskan H, Oktay B. Fournier’s gangrene: an analysis of 80 patients and a novel scoring system. Tech Coloproctol 2010; 14:217-23.
doi: 10.1007/s10151-010-0592-1
pmid: 20559857
[8]
Seymour CW, Liu VX, Iwashyna TJ, Brunkhorst FM, Rea TD, Scherag A, et al. Assessment of clinical criteria for sepsis for the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). J Am Med Assoc 2016; 315: 762-74.
doi: 10.1001/jama.2016.0288
[9]
Doluo?lu ?G, Karag?z MA, K?l?n? MF, Karakan T, Yücetürk CN, Sar?c? H, et al. Overview of different scoring systems in Fournier’s gangrene and assessment of prognostic factors. Turk J Urol 2016; 42: 190-6.
[10]
Noegroho BS, Siregar S, Mustafa A, Rivaldi MA. Validation of FGSI scores in predicting Fournier gangrene in tertiary hospi-tal. Res Rep Urol 2021; 13:341-6.
[11]
Shukla PK, Ghanghoria A, Yedalwar V. Fournier’s gangrene: a prospective study of 57 patients with special reference to validity of Fournier’s gangrene severity index in predicting the outcome and mortality. Int Surg J 2016; 3:1256-61.
[12]
Benjelloun EB, Souiki T, Yakla N, Ousadden A, Mazaz K, Louchi A, et al. Fournier’s gangrene: our experience with 50 patients and analysis of factors affecting mortality. World J Emerg Surg 2013; 8:13. https://doi.org/10.1186/1749-7922-8-13.
[13]
Yeniyol CO, Suelozgen T, Arslan M, Ayder AR. Fournier’s gangrene: experience with 25 patients and use of Fournier’s gangrene severity index score. Urology 2004; 64:218-22.
doi: 10.1016/j.urology.2004.03.049
pmid: 15302463
Tahmaz L, Erdemir F, Kibar Y, Cosar A, Yalcy ′n O. Fournier’s gangrene: report of thirty-three cases and a review of the literature. Int J Urol 2006; 13:960-7.
[16]
Pandey S, Narayan Sankhwar S, Goel A, Kumar M, Aggarwal A, Sharma D, et al. Quick Sequential (Sepsis related) Organ Failure Assessment: a high performance rapid prognostication tool in patients having acute pyelonephritis with upper urinary tract calculi. Investig Clin Urol 2019; 60:120-6.
doi: 10.4111/icu.2019.60.2.120
pmid: 30838345
[17]
Fukushima H, Kobayashi M, Kawano K, Morimoto S. Performance of Quick Sequential (Sepsis related) and Sequential (Sepsis related) Organ Failure Assessment to predict mortality in patients with acute pyelonephritis associated with upper urinary tract calculi. J Urol 2018; 199:1526-33.
doi: S0022-5347(17)78189-X
pmid: 29291417
[18]
Roghmann F, Von Bodman C, Loppenberg B, Hinkel A, Palisaar J, Noldus J. Is there a need for Fournier’s gangrene severity index? Comparison of scoring systems for outcome prediction in patients with Fournier’s gangrene. BJU Int 2012; 110:1359-65.
doi: 10.1111/j.1464-410X.2012.11082.x
pmid: 22494217
[19]
Martinschek A, Evers B, Lampl L, Gernros H, Schmidt R, Sparwasser C. Prognostic aspects, survival rate, and predisposing risk factors in patients with Fournier’s gangrene and necrotizing soft tissue infections: evaluation of clinical outcome of 55 patients. Urol Int 2012; 89:173-9.
doi: 10.1159/000339161
pmid: 22759538
[20]
Erol B, Tuncel A, Hanci V, Tokgoz H, Yildiz A, Akduman B, et al. Fournier’s gangrene: overview of prognostic factors and definition of new prognostic parameter. Urology 2010; 75: 1193-8.
doi: 10.1016/j.urology.2009.08.090
[21]
Corcoran AT, Smaldone MC, Gibbons EP, Walsh TJ, Davies BJ. Validation of the Fournier’s gangrene severity index in a large contemporary series. J Urol 2008; 180:944-8.
[22]
Altarac S, Katusin D, Crnica S, Papes D, Rajkovic Z, Arslani N. Fournier’s gangrene: etiology and outcome analysis of 41 patients. Urol Int 2012; 88:289-93.
doi: 10.1159/000335507
pmid: 22433163
[23]
Sonneville R, Verdonk F, Rauturier C, Klein IF, Wolff M, Annane D, et al. Understanding brain dysfunction in sepsis. Ann Intensive Care 2013; 3:15. https://doi.org/10.1186/2110-5820-3-15.
doi: 10.1186/2110-5820-3-15
pmid: 23718252
[24]
Vincent JL, Moreno R, Takala J, Willatts S, De Mendonca A, Bruining H, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive Care Med 1996; 22:707-10.
doi: 10.1007/BF01709751
[25]
Dolan R, Polito C, Isakov A, Yancey A, Bloom I, Martin GS, et al. Utility of pre-hospital Glasgow Coma Scale in predicting in- hospital mortality in patients with sepsis. Am J Respir Crit Care Med 2016; 193:A7619. https://www.atsjournals.org/doi/pdf/10.1164/ajrccm-conference.2016.193.1_MeetingAbstracts.A7619.
[26]
Dewitte A, Lepreux S, Villeneuve J, Rigothier C, Combe C, Ouattara A, et al. Blood platelets and sepsis pathophysiology: a new therapeutic prospect in critically ill patients? Ann Intensive Care 2017; 7:115. https://doi.org/10.1186/s13613-017-0337-7.
doi: 10.1186/s13613-017-0337-7
[27]
Venkata C, Kashyap R, Farmer JC, Afessa B. Thrombocyto- penia in adult patients with sepsis: incidence, risk factors, and its association with clinical outcome. J Intensive Care 2013; 1:9. https://doi.org/10.1186/2052-0492-1-9.
doi: 10.1186/2052-0492-1-9
[28]
Sun JK, Sun F, Wang X, Yuan ST, Zheng SY, Mu XW. Risk factors and prognosis of hypoalbuminemia in surgical septic patients. PeerJ 2015; 3:e1267. https://doi.org/10.7717/peerj.1267.
doi: 10.7717/peerj.1267
[29]
Jiang J, Yang J, Mei J, Jin Y, Lu Y. Head-to-head comparison of qSOFA and SIRS criteria in predicting the mortality of infected patients in the emergency department: a meta-analysis. Scand J Trauma Resusc Emerg Med 2018; 26:56. https://doi.org/10.1186/s13049-018-0527-9.
doi: 10.1186/s13049-018-0527-9
[30]
Liu YC, Luo YY, Zhang X, Shou ST, Gao YL, Lu B, et al. Quick Sequential Organ Failure Assessment as a prognostic factor for infected patients outside the intensive care unit: a systematic review and meta-analysis. Intern Emerg Med 2019; 14:603-15.
doi: 10.1007/s11739-019-02036-0
[31]
Sallami S, Maalla R, Gammoudi A, Jdidia B, Tarhouni L, Horchani A. Fournier’s gangrene: what are the prognostic factors? Our experience with 40 patients. Tunis Med 2012; 90: 708-14.
[32]
McCormack M, Valiquette AS, Ismail S. Fournier’s gangrene: a retrospective analysis of 26 cases in a Canadian hospital and literature review. Can Urol Assoc J 2015; 9:E407-10. https://doi.org/10.5489/cuaj.2445.
[33]
Sánchez Mazzaferri F, Fadil Iturralde JL, Provenzal O, Damiani H, Milman A, Bragagnolo J, et al. [Fournier’s gangrene. Our experience over 10 years. A review of the literature]. Arch Esp Urol 1999; 52:721-7. [Article in Spanish].
pmid: 10540762