|
|
|
| Effectiveness and economic outcomes in patients undergoing laparoscopic radical prostatectomy with a new surgical shear with an integrated energy system: A retrospective study based on a tertiary hospital database in China |
Yi Gaoa,Yu Zhua,Fukang Suna,Yuan Shaoa,Tao Huanga,Wei Hea,Xin Xiea,Lu Chena,Debra Winbergb,Danfeng Xua,*( ) )
|
aRuijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China
bTulane School of Public Health and Tropical Medicine, Department of Health Policy and Management, New Orleans, LA, USA |
|
|
|
|
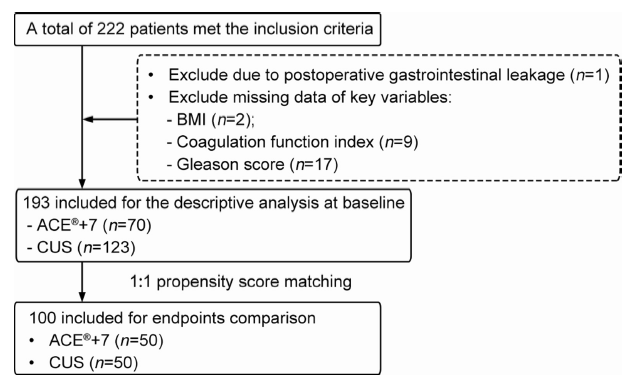
Abstract Objective: This study aimed to demonstrate a new surgical shear with an integrated energy system (Harmonic ACE®+7) value by determining its effectiveness and economic outcomes compared with conventional ultrasonic shears (CUSs) in a real-world setting. Methods: This was a retrospective study of adults with prostate cancer undergoing laparoscopic radical prostatectomy with the ACE®+7 shear or CUSs between August 2019 and April 2021 at Shanghai Ruijin Hospital (the headquarters and Luwan Center in China). Demographic and diagnosis information, intraoperative and postoperative clinical outcomes, and total and categorical costs were collected. Propensity score matching was performed to form the study population for each clinical group. Data were compared between the two groups using t-test and Chi-squared test. Results: The ACE®+7 was associated with a lower mean number of hemostatic clips used per surgery compared with CUSs (12.8 vs. 19.8, p<0.001), a moderate but not significant difference in mean postoperative drainage duration (6.6 [standard deviation, SD 2.2] days vs. 7.9 [SD 4.1] days, p=0.082), a reduction on mean total drainage volume (275.5 [SD 374.3 mL vs. 492.9 [SD 1495.0] mL, p=0.321), and a lower mean rate of postoperative hemostatic drug usage (16.0% vs. 52.0%, p<0.001). There was no significant difference in total costs between the ACE®+7 and CUS groups. Conclusion: This study provides real-world data demonstrating that the ACE®+7 shear with an integrated energy system improves clinical outcomes compared with CUSs and can offer cost savings for hospitals and health systems. Using the ACE®+7 during laparoscopic radical prostatectomy allows physicians to help their patients achieve better outcomes and not spend additional money.
|
|
Received: 07 March 2023
Available online: 20 October 2024
|
|
Corresponding Authors:
*E-mail address: xdf12036@rjh.com.cn (D. Xu).
|
|
|
|
|
Patient population selection. BMI, body mass index; CUS, conventional ultrasonic shear.
|

| Baseline characteristic | ACE®+7 groupa (n=70) | CUS groupa (n=123) | p-Value | | Age, year | 68.6±6.6 | 68.9±6.5 | 0.736 | | Study site | | | 0.005 | | Headquarters | 35 (50.0) | 88 (71.5) | | | Ruijin Luwan center | 35 (50.0) | 35 (28.5) | | | BMI, kg/m2 | 24.5±2.4 | 23.9±2.7 | 0.156 | | Comorbidity of hypertension | 34 (48.6) | 61 (49.6) | 1.000 | | Comorbidity of diabetes | 13 (18.6) | 18 (14.6) | 0.608 | | Preoperative abnormal coagulation function | 36 (51.4) | 42 (34.1) | 0.028 | | Gleason score | 7.5±1.0 | 7.3±0.9 | 0.115 | | Lymph node dissection during surgery | 57 (81.4) | 63 (51.2) | <0.001 | | Pelvic adhesiolysis during surgery | 35 (50.0) | 58 (47.2) | 0.818 |
|
|
Comparisons of baseline characteristics between the ACE®+7 group and CUS group.
|
| Baseline characteristic | ACE®+7 groupa (n=50) | CUS groupa (n=50) | p-Value | | Age, year | 68.2±6.2 | 68.4±7.1 | 0.858 | | Study site | | | 0.682 | | Headquarters | 32 (64.0) | 29 (58.0) | | | Ruijin Luwan center | 18 (36.0) | 21 (42.0) | | | BMI, kg/m2 | 24.3±2.6 | 23.6±3.2 | 0.224 | | Comorbidity of hypertension | 26 (52.0) | 25 (50.0) | 1.000 | | Comorbidity of diabetes | 9 (18.0) | 7 (14.0) | 0.785 | | Preoperative abnormal coagulation function | 20 (40.0) | 21 (42.0) | 1.000 | | Gleason score | 7.6±1.0 | 7.7±1.0 | 0.477 | | Lymph node dissection during surgery | 39 (78.0) | 37 (74.0) | 0.815 | | Pelvic adhesiolysis during surgery | 32 (64.0) | 25 (50.0) | 0.226 |
|
|
Comparisons of baseline characteristics between the ACE®+7 group and CUS group after 1:1 prop-nsity score matching.
|
| Clinical outcome | ACE®+7 groupa (n=50) | CUS groupa (n=50) | p-Value | | Intraoperative hemostatic clip usage, n | 12.8±5.8 | 19.8±6.6 | <0.001 | | Intraoperative blood loss, mL | 191.1±152.8 | 204.2±181.6 | 0.782 | | Transfusion | 1 (2.0) | 3 (6.0) | 0.610 | | Operation time, min | 162.6±44.8 | 158.0±37.4 | 0.586 | | Postoperative hemostatic drug usage | 8 (16.0) | 26 (52.0) | <0.001 | | Postoperative length of drainage, day | 6.6±2.2 | 7.9±4.1 | 0.082 | | Postoperative drainage volume within 24 h, mL | 72.0±59.1 | 133.4±282.0 | 0.135 | | Postoperative drainage volume within 48 h, mL | 143.4±135.5 | 239.6±495.9 | 0.189 | | Postoperative total drainage volume, mL | 275.5±374.3 | 492.9±1495.0 | 0.321 | | Length of stay, dayb | 10.7±3.4 | 11.3±4.8 | 0.413 | | Postoperative length of stay, dayc | 7.9±3.0 | 8.6±4.2 | 0.337 | | Re-operation during the LRP procedure hospitalization | 0 | 0 | NA | | Postoperative readmission within 30 days | 0 | 0 | NA |
|
|
Comparisons of clinical outcomes between the ACE®+7 group and CUS group after 1:1 prop-nsity score matching.
|
| Cost, RMB | ACE®+7 groupa (n=50) | CUS groupa (n=50) | Differenceb | p-Value | | Total cost | 42 675.0±5134.5 | 41 426.3±7623.7 | 1248.7 | 0.349 | | Device cost | 23 308.4±5702.0 | 19 467.5±5946.7 | 3840.9 | 0.002 | | Treatment cost | 3287.0±3902.9 | 4412.4±4097.2 | -1125.4 | 0.176 | | Pharmaceutical cost | 6800.3±4169.0 | 7436.4±4481.4 | -636.1 | 0.478 | | Nursing cost | 555.6±275.8 | 649.9±352.1 | -94.3 | 0.149 | | Board and room cost | 723.0±636.0 | 858.7±694.4 | -135.7 | 0.325 | | Lab test cost | 2636.8±805.9 | 3132.3±1280.2 | -495.5 | 0.025 | | Examination cost | 3591.3±763.4 | 3792.1±1178.1 | -200.8 | 0.324 | | Transfusion cost | 20.0±141.4 | 49.2±192.0 | -29.2 | 0.400 | | Oxygen therapy cost | 44.3±8.4 | 62.9±50.8 | -18.6 | 0.012 | | TCM cost | 996.5±1034.8 | 765.4±999.0 | 231.1 | 0.275 | | Diagnosis cost | 376.0±88.7 | 384.4±106.0 | -8.4 | 0.677 | | Other cost | 335.8±355.5 | 415.1±426.8 | -79.3 | 0.328 | | Total cost excluding intervention costc | 38 357.8±5127.1 | 39 983.1±7618.3 | -1625.3 | 0.223 |
|
|
Direct hospitalization cost comparisons between the ACE®+7 group and CUS group after 1:1 prop-nsity score matching.
|
| [1] |
Speight J, Holmes-Truscott E, Hendrieckx C, Skovlund S, Cooke D. Assessing the impact of diabetes on quality of life: what have the past 25 years taught us? Diabet Med 2020; 37:483-92.
|
| [2] |
Schatten H. Brief overview of prostate cancer statistics, grading, diagnosis and treatment strategies. Adv Exp Med Biol 2018; 1095:1-14.
doi: 10.1007/978-3-319-95693-0_1
pmid: 30229546
|
| [3] |
Chaussy CG, Thüroff S. High-intensity focused ultrasound for the treatment of prostate cancer: a review. J Endourol 2017; 31:S30-7. https://doi.org/10.1089/end.2016.0548.
|
| [4] |
Yu W, Zhou L. Early diagnosis of prostate cancer from the perspective of Chinese physicians. J Cancer 2020; 11:3264-73.
doi: 10.7150/jca.36697
pmid: 32231732
|
| [5] |
Chinese guidelines for diagnosis and treatment of prostate cancer 2018 (English version). Chin J Cancer Res 2019; 31:67-83.
|
| [6] |
Kondrup JD, Anderson F, Sylvester B, Branning M. The new HARMONIC ACE®+7 shears: a game changer in ultrasonic hemostasis. Surg Technol Int 2014; 25:24-7.
pmid: 25419951
|
| [7] |
Timm RW, Asher RM, Tellio KR, Welling AL, Clymer JW, Amaral JF. Sealing vessels up to 7 mm in diameter solely with ultrasonic technology. Med Devices (Auckl) 2014; 7:263-71.
|
| [8] |
Church JT, McLeod JS, Coughlin MA, Bergin IL, Perkins EM, Hoffman HR, et al. An early investigation into possible alternatives to stapled hysterotomy in open fetal surgery. Am J Perinatol 2019; 36:742-50.
doi: 10.1055/s-0038-1673664
pmid: 30372770
|
| [9] |
Singleton D, Juncosa-Melvin N, Scoggins P, Paulin-Curlee G, Cummings J, Ricketts C. Intelligent ultrasonic energy: new adaptive tissue technology in HARMONIC shears. J Surg 2020; 8:178-83.
|
| [10] |
Zurawin R, Pickron T, Blackstone R. Intelligent ultrasonic energy delivered by HARMONIC® devices with adaptive tissue technology. https://www.academia.edu/32143407/Intelligent_Ultrasonic_Energy_Delivered_by_HARMONIC_devices_with_Adaptive_Tissue_Technology. [Accessed November 1, 2021].
|
| [11] |
Benedetto U, Head SJ, Angelini GD, Blackstone EH. Statistical primer: propensity score matching and its alternatives. Eur J Cardio Thorac Surg 2018; 53:1112-7.
|
| [12] |
Dokmak S, Ftériche FS, Aussilhou B, Lévy P, Ruszniewski P, Cros J, et al. The largest European single-center experience: 300 laparoscopic pancreatic resections. J Am Coll Surg 2017; 225:226-34.e2. https://doi.org/10.1016/j.jamcollsurg.2017.04.004.
|
| [13] |
Curnow J, Pasalic L, Favaloro EJ. Why do patients bleed? Surg J 2016; 2:e29-43. https://doi.org/10.1055/s-0036-1579657.
|
| [14] |
Marietta M, Facchini L, Pedrazzi P, Busani S, Torelli G. Pathophysiology of bleeding in surgery. Transplant Proc 2006; 38:812-4.
|
| [15] |
Franco Moreno AI, Martín Díaz RM, García Navarro MJ. Direct oral anticoagulants: an update. Med Clin 2018; 151:198-206.
|
| [16] |
Yip W, Fu H, Chen AT, Zhai T, Jian W, Xu R, et al. 10 years of health-care reform in China: progress and gaps in Universal Health Coverage. Lancet 2019; 394:1192-204.
doi: S0140-6736(19)32136-1
pmid: 31571602
|
| [17] |
Zhang J, Xian TZ, Wu MX, Li C, Pan Q, Guo LX. Comparison of the effects of twice-daily exenatide and insulin on carotid intima-media thickness in type 2 diabetes mellitus patients: a 52-week randomized, open-label, controlled trial. Cardiovasc Diabetol 2020; 19:48. https://doi.org/10.1186/s12933-020-01014-7.
doi: 10.1186/s12933-020-01014-7
pmid: 32334592
|
| No related articles found! |
|
|
|
|