|
|
|
| Description of a novel robotic early post-prostatectomy anastomotic repair technique and institutional outcomes |
David Strauss,Eric Cho,Matthew Loecher,Matthew Lee,Daniel Eun*( ) )
|
| Department of Urology, Lewis Katz School of Medicine, Temple University, Philadelphia, PA, USA |
|
|
|
|
Abstract Objective: A vesicourethral anastomotic leak (VUAL) is a known complication following robotic-assisted radical prostatectomy. The natural history of a VUAL has been well described and is frequently managed with prolonged catheterization. With increasing emphasis on patient reported outcomes, catheter duration and VUAL are associated with significant short-term quality of life impairment. We aimed to present a case series of our robotic early post-prostatectomy anastomotic repair technique, defined as revision within 6 weeks from index surgery. Methods: A single institution prospective database identified eleven patients with a VUAL from July 2016 to October 2022 who underwent robotic early post-prostatectomy anastomotic repair by a single surgeon. Patients were diagnosed with a VUAL on pre-operative CT urogram or CT/fluoroscopic cystogram. The primary outcome was resolution of the anastomotic leak, defined as no contrast extravasation on post-operative cystography. Secondary outcomes included post-repair catheter duration and continence on the last follow-up defined as pad(s) per day. Results: The mean time to intervention after robotic-assisted radical prostatectomy was 21 days. Eight of the eleven (72.7%) patients had no evidence of extravasation on post-repair cystogram. The range from intervention to first cystogram was 7-20 days. The median catheter duration for those with successful intervention was 10 days. The median catheter duration for those with the leak on initial post-operative cystogram was 20 days. At a mean follow-up time of 25 months, eight (72.7%) patients reported using no pads per day, and three (27.3%) patients reported one pad per day. Conclusion: Management of a VUAL has traditionally relied on prolonged catheter drainage and the tincture of time. As the role of robotic reconstruction has been shown to be a viable modality for management of bladder neck contracture, it is important to reconsider prior dogmas of urologic care. Our case series suggests that an early repair is safe and has a high success rate. Early robotic intervention gives providers an additional tool in aiding patient recovery.
|
|
Received: 24 June 2023
Available online: 20 July 2024
|
|
Corresponding Authors:
*E-mail address: Daniel.Eun@tuhs.temple.edu (D. Eun).
|
|
|

|
|
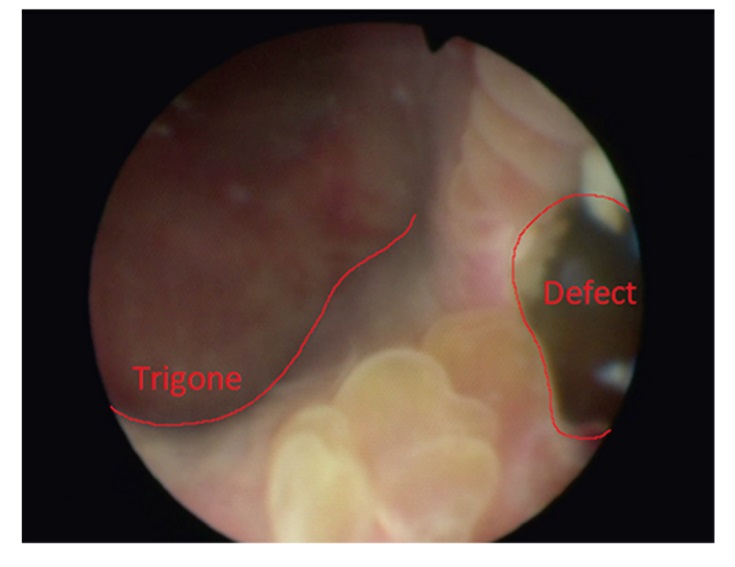
Cystoscopy demonstrating a partial view of the anastomotic disruption (labeled as “Defect”) at the 5 o'clock position of the bladder neck.
|
|
|
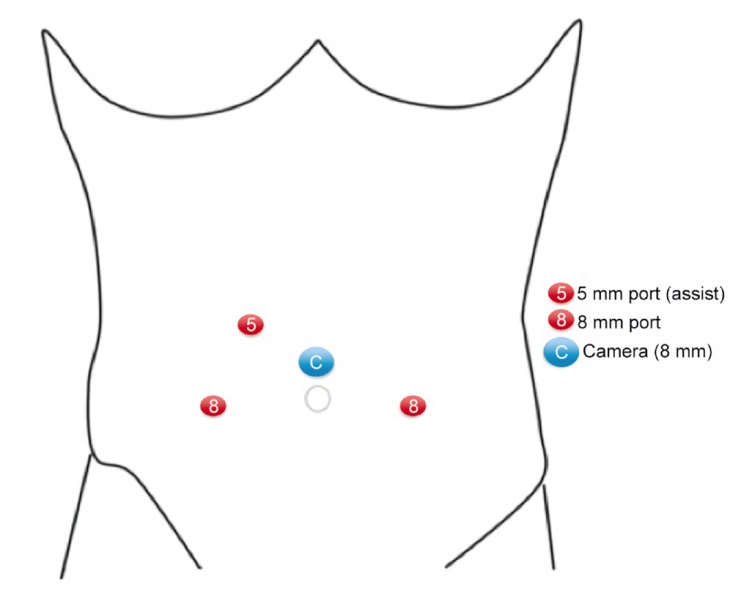
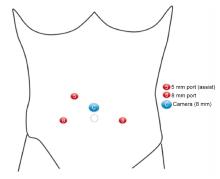
Port placement for surgical approach. When possible, prior robotic-assisted radical prostatectomy port sites were used.
|

|
|
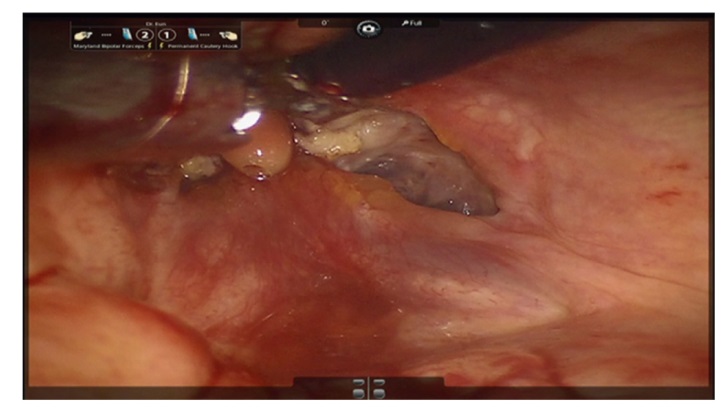
A vertical midline cystotomy was created for transvesical access to the anastomotic disruption.
|

|
|
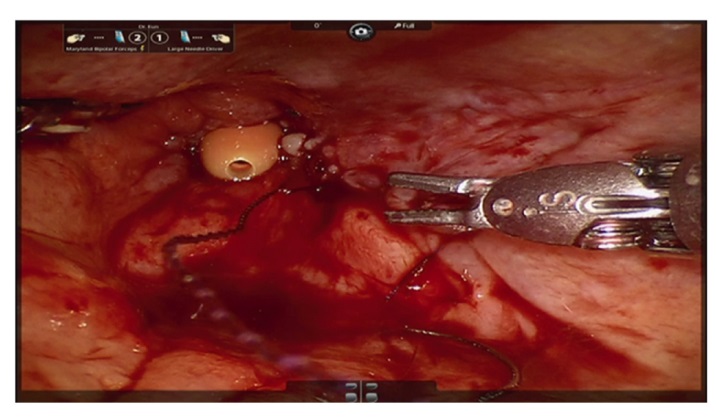
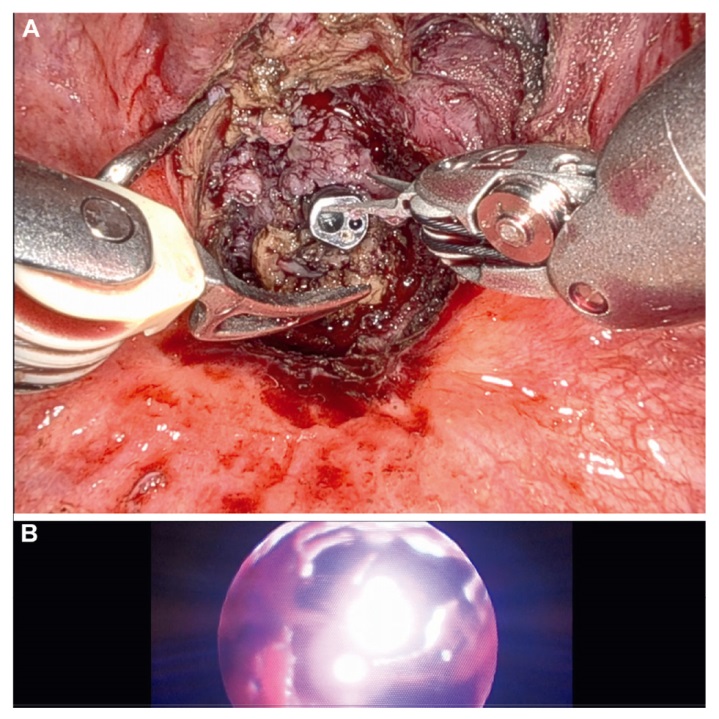
A vesicourethral anastomotic leak was inspected and an anastomotic repair was performed by re-approximating the urethral mucosa with the bladder mucosa. The urethral catheter, or bedside assistant via cystoscopy, can facilitate locating the urethral lumen. Fibrinous or necrotic tissue can be excised to aid in a tension-free mucosa to mucosa anastomosis.
|

|
|
The anastomosis was completed and an 18 Fr urethral catheter was inserted.
|

| Patient | Age, year | BMI, kg/m2 | Diagnostic modality | Location of defect | Days from index surgery to intervention | | 1 | 63 | 28.3 | CT urogram | Posterior | 49 | | 2 | 75 | 28.3 | CT urogram | Posterior | 25 | | 3 | 58 | 24.3 | Fluoroscopic cystogram | Posterior | 14 | | 4 | 68 | 26.8 | CT cystogram | Right posterior | 11 | | 5 | 50 | 26.4 | CT urogram | Left posterior | 19 | | 6 | 65 | 33.8 | CT urogram | Right and left posterior | 14 | | 7 | 57 | 32.3 | CT cystogram | Circumferential | 32 | | 8 | 59 | 27.0 | CT cystogram | Right | 1 | | 9 | 60 | 32.5 | CT cystogram | Posterior | 14 | | 10 | 58 | 26.4 | CT cystogram | Circumferential | 22 | | 11 | 55 | 27.4 | CT cystogram | Posterior | 35 | | Totala | 61±7 | 28.5±3.1 | - | - | 21±13 |
|
|
Patient demographics and leak characteristics.
|
| Patient | Hospital length, day | EBL, mL | Console time, min | Successful intervention | Catheter duration, day | Length of follow-up, month | Continence, pad per day | | 1 | 2 | 50 | 60 | Yes | 5 | 78 | 0 | | 2 | 3 | 50 | 89 | Yes | 8 | 37 | 0 | | 3 | 1 | 50 | 120 | Yes | 9 | 52 | 0 | | 4 | 3 | 100 | 144 | No | 35 | 12 | 0 | | 5 | 3 | 25 | 114 | Yes | 11 | 10 | 0 | | 6 | 1 | 50 | 138 | Yes | 20 | 5 | 1 | | 7 | 2 | 25 | 122 | Yes | 21 | 38 | 0 | | 8 | 1 | 30 | 80 | Yes | 14 | 16 | 1 | | 9 | 2 | 50 | 112 | No | 56 | 20 | 0 | | 10 | 5 | 50 | 115 | No | 40 | 4 | 1 | | 11 | 0 | 75 | 91 | Yes | 8 | 1 | 0 | | Totala | 2±1 | 50±22 | 107±25 | - | 20±16 | 25±24 | 0.3±0.5 |
|
|
Results and outcomes.
|
|
|
A vesicourethral anastomotic stricture approximately 1 year after robotic-assisted radical prostatectomy and several endoscopic procedures. (A) Transvesical view; (B) Cystoscopic view.
|
| [1] |
Hakimi AA, Faleck DM, Sobey S, Ioffe E, Rabbani F, Donat SM, et al. Assessment of complication and functional outcome reporting in the minimally invasive prostatectomy literature from 2006 to the present. BJU Int 2012; 109:26-30.
|
| [2] |
Tyritzis S, Katafigiotis I, Constantinides CA. All you need to know about urethrovesical anastomotic urinary leakage following radical prostatectomy. J Urol 2012; 188:369-76.
|
| [3] |
Herman MP, Raman JD, Dong S, Samadi D, Scherr DS. Increasing body mass index negatively impacts outcomes following robotic radical prostatectomy. J Soc Laparoendosc Surg 2007; 11:438-42.
|
| [4] |
Ye H, Wu YS, Liu ZW, Guo LH, Zhang JY, Wang XL. Comparison of outcomes between two vesicourethral anastomotic reconstruction techniques after robot-assisted laparoscopic radical prostatectomy. J Endourol 2020; 34:47-53.
|
| [5] |
Tan G, Srivastava A, Grover S, Peters D, Dorsey Jr P, Scott A, et al. Optimizing vesicourethral anastomosis healing after robot-assisted laparoscopic radical prostatectomy: lessons learned from three techniques in 1900 patients. J Endourol 2010; 24:1975-83.
|
| [6] |
bAhlering TE, Eichel L, Edwards R, Skarecky DW. Impact of obesity on clinical outcomes in robotic prostatectomy. Urology 2005; 65:740-4.
|
| [7] |
Sandhu JS, Gotto GT, Herran LA, Scardino PT, Eastham JA, Rabbani F. Age, obesity,medical comorbidities and surgical technique are predictive of symptomatic anastomotic strictures after contemporary radical prostatectomy. J Urol 2011; 185:2148-52.
|
| [8] |
Sukkarieh T, Harmon J, Penna F, Parra R. Incidence and management of anastomotic leakage following laparoscopic prostatectomy with implementation of a new anastamotic technique incorporating posterior bladder neck tailoring. J Robot Surg 2007; 1:213-5.
|
| [9] |
Mochtar CA, Kauer PC, Laguna MP, de la Rosette JJMCH. Urinary leakage after laparoscopic radical prostatectomy: a systematic review. J Endourol 2007; 21:1371-9.
|
| [10] |
Moinzadeh A, Abouassaly R, Gill IS, Libertino JA. Continuous needle vented Foley catheter suction for urinary leak after radical prostatectomy. J Urol 2004; 171:2366-7.
|
| [11] |
Shah G, Vogel F, Moinzadeh A. Nephroureteral stent on suction for urethrovesical anastomotic leakafter robot-assisted laparoscopic radical prostatectomy. Urology 2009; 73:1375-6.
|
| [12] |
Elmor T, Rubinstein M, Lima G, Cruz AC, Pereira CFT, Rubinstein I. Minimally invasive treatment of vesicourethral leak after laparoscopic radical prostatectomy. Rev Col Bras Cir 2016; 43:185-8.
|
| [13] |
Yossepowitch O, Baniel J. Persistent vesicourethral anastomotic leak after radical prostatectomy: a novel endoscopic solution. J Urol 2010; 184:2452-5.
|
| [14] |
Diamand R, Hajj Obeid WAl, Accarain A, Limani K, Hawaux E, van Velthoven R, et al. Management of anastomosis leakage post-RALP: a simple trick for a complex situation. Urol Case Rep 2017; 12:28-30.
|
| [15] |
Castillo OA, Alston C, Sanchez-Salas R. Persistent vesicourethral anastomotic leak after laparoscopic radical prostatectomy: laparoscopic solution. Urology 2009; 73:124-6.
|
| [16] |
Kim S, Buckley JC. Robotic lower urinary tract reconstruction. Urol Clin 2021; 48:103-12.
|
| [17] |
Tewari A, Sooriakumaran P, Bloch D, Seshadri-Kreaden U, Hebert AE, Wiklund P, et al. Positive surgical margin and perioperative complication rates of primary surgical treatments for prostate cancer: a systematic review and metaanalysis comparing retropubic, laparoscopic, and robotic prostatectomy. Eur Urol 2012; 62:1-15.
|
| [1] |
Simone Sforza,Valeria Emma Palmieri,Maria Rosaria Raspollini,Giandomenico Roviello,Alberto Mantovani,Umberto Basso,Maria Carmen Affinita,Alberto D’Angelo,Lorenzo Antonuzzo,Marco Carini,Andrea Minervini,Lorenzo Masieri. Robotic approach with neoadjuvant chemotherapy in adult Wilms’ tumor: A feasibility study report and a systematic review of the literature[J]. Asian Journal of Urology, 2023, 10(2): 128-136. |
| [2] |
Gilberto José Rodrigues,Giuliano Betoni Guglielmetti,Marcelo Orvieto,Kulthe Ramesh Seetharam Bhat,Vipul R. Patel,Rafael Ferreira Coelho. Robot-assisted endoscopic inguinal lymphadenectomy: A review of current outcomes[J]. Asian Journal of Urology, 2021, 8(1): 20-26. |
| [3] |
Weibin Xie,Junming Bi,Qiang Wei,Ping Han,Dongkui Song,Lei Shi,Dingwei Ye,Yijun Shen,Xin Gou,Weiyang He,Shaogang Wang,Zheng Liu,Jinhai Fan,Kaijie Wu,Zhiwen Chen,Xiaozhou Zhou,Chuize Kong,Yang Liu,Chunxiao Liu,Abai Xu,Baiye Jin,Guanghou Fu,Wei Xue,Haige Chen,Tiejun Pan,Zhong Tu,Tianxin Lin,Jian Huang. Survival after radical cystectomy for bladder cancer: Multicenter comparison between minimally invasive and open approaches[J]. Asian Journal of Urology, 2020, 7(3): 291-300. |
| [4] |
Xiaofeng Zou,Guoxi Zhang,Tianpeng Xie,Yuanhu Yuan,Rihai Xiao,Gengqing Wu,Xiaoning Wang,Hui Xu,Folin Liu,Yuting Wu,Yunfeng Liao,Quanliang Liu,Yinghao Sun,Bo Yang,Linhui Wang,Chuanliang Xu,Xiaofeng Gao. Natural orifice transluminal endoscopic surgery in urology: The Chinese experience[J]. Asian Journal of Urology, 2020, 7(1): 1-9. |
|
|
|
|