|
|
|
| Prospective randomized study to evaluate and compare the post-procedural sexual function in patients undergoing semi-rigid ureterorenoscopy for distal ureteric stones in three different operating room settings |
Gajanan S. Bhata,*( ),Anuradha Shastryb ),Anuradha Shastryb
|
aSexual Medicine, TSS Shripad Hegde Kadave Institute of Medical Sciences, Sirsi, Karnataka, India
bDepartment of Urology, Andrology and Sexual Medicine, TSS Shripad Hegde Kadave Institute of Medical Sciences, Sirsi, Karnataka, India |
|
|
|
|
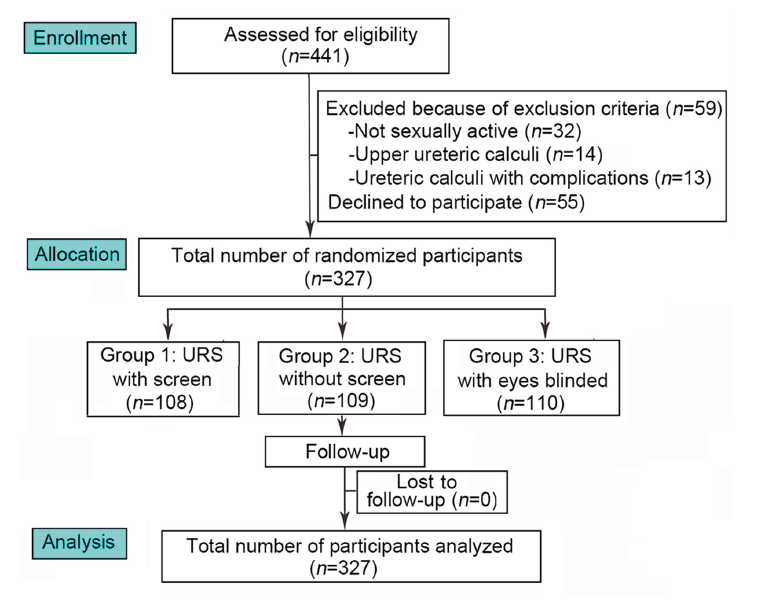
Abstract Objective: To evaluate and compare the effect of semi-rigid ureterorenoscopy on post-procedural sexual function with three different operating room settings. Methods: In this prospective randomized study, consecutive sexually active patients with normal pre-operative sexual function undergoing uncomplicated semi-rigid ureterorenoscopy for distal ureteric stones were randomized into three groups, with three different operating room settings. Procedure-related anxiety and sexual function were assessed pre-operatively using Amsterdam Preoperative Anxiety and Information Scale and Brief Sexual Function Inventory (in males) and Female Sexual Function Index-6 (in females), respectively. All the participants were stented following the procedure, and the stent was removed after 3 weeks. Post-procedural sexual function and general discomfort were assessed and compared between three groups at 1 week, 3 weeks, and 12 weeks. The effect of surgery-related anxiety, preoperative sexual function, age, and general discomfort (including stent-related discomfort) on post-procedural sexual function were analyzed using multiple regression analysis. A p-value of less than 0.05 was considered statistically significant. Results: Totally, 327 eligible patients were randomized into three groups. The group of patients who underwent the procedural with a screen separating the operating area from the patient vision, while the patient could watch the endoscopy through a separate monitor, had better post-procedural sexual function compared to those who had total vision of the operating area as well as to those whose eyes were blocked. This difference was statistically significant. This post-procedural reduction in sexual function could not be attributed to in situ stent alone. Conclusions: Our study showed that semi-rigid ureterorenoscopy can have significant negative effect on sexual function, which can be reduced with proper preoperative counseling and an ideal operating room settings.
|
|
Received: 23 March 2022
Available online: 20 April 2024
|
|
Corresponding Authors:
* E-mail address: gajubhatru@gmail.com (G.S. Bhat).
|
|
|

|
|
Participant flow diagram. URS, ureterorenoscopy.
|

| Characteristic | Group 1a (n=108) | Group 2a (n=109) | Group 3a (n=110) | p-Value | | Age, year | 37.9±9.6 | 39.5±8.5 | 39.2±9.6 | >0.05 | | Male:female | 3.5:1 | 3.5:1 | 3.4:1 | >0.05 | | Preoperative APAIS score | 8.9±2.1 | 8.7±1.7 | 8.8±2.0 | >0.05 | | BSFI score in males (highest possible 45) | | Pre-procedural | 39.7±2.0 | 39.4±2.2 | 39.6±2.2 | >0.05 | | 1 week postoperatively | 29.5±2.4 | 21.4±1.8 | 20.8±2.6 | >0.05 (between Groups 2 and 3);
<0.05 (between Groups 1 and 3, 1 and 3) | | 3 weeks postoperatively | 31.3±3.4 | 24.9±2.9 | 27.3±2.8 | <0.05 (all inter groups) | | 12 weeks postoperatively | 37.6±1.4 | 36.9±0.9 | 36.3±1.5 | >0.05 | | FSFI-6 score in females (highest possible 30) | | Pre-procedural | 26.4±1.7 | 26.3±1.7 | 26.2±1.8 | >0.05 | | 1 week postoperatively | 13.8±2.3 | 11.3±2.4 | 9.9±1.9 | <0.05 (all inter groups) | | 3 weeks postoperatively | 16.5±1.9 | 14.0±2.4 | 14.4±1.9 | >0.05 (between Groups 2 and 3);
<0.05 (between Groups 1 and 3, 1 and 3) | | 12 weeks postoperatively | 23.8±1.7 | 21.5±1.9 | 20.7±1.8 | >0.05 (between Groups 2 and 3);
<0.05 (between Groups 1 and 3, 1 and 3) | | VNRS | | 1 week postoperatively | 2.6±0.6 | 2.7±0.6 | 2.7±.5 | >0.05 | | 3 weeks postoperatively | 3.6±1.2 | 3.8±1.4 | 4.3±1.2 | >0.05 (between Groups 1 and 2);
<0.05 (between Groups 1 and 3, 1 and 3) | | 12 weeks postoperatively | 7.9±0.8 | 8.2±0.8 | 8.2±0.7 | >0.05 |
|
|
Patient characteristics.
|
| Sexual domain | Group 1 (n=108) | Group 2 (n=109) | Group 3 (n=110) | | Males (n=84) | Females (n=24) | Males (n=85) | Females (n=24) | Males (n=85) | Females (n=25) | | 1 week | 3 weeks | 12 weeks | 1 week | 3 weeks | 12 weeks | 1 week | 3 weeks | 12 weeks | 1 week | 3 weeks | 12 weeks | 1 week | 3 weeks | 12 weeks | 1 week | 3 weeks | 12 weeks | | Sexual drive | 57 (67.9) | 46 (54.8) | 3 (3.6) | NA | NA | NA | 64 (75.3) | 55 (64.7) | 11 (12.9) | NA | NA | NA | 75 (88.2) | 68 (80.0) | 7 (8.2) | NA | NA | NA | | Erectile function | 39 (46.4) | 26 (31.0) | 4 (4.8) | NA | NA | NA | 52 (61.2) | 35 (41.2) | 8 (9.4) | NA | NA | NA | 43 (50.6) | 38 (44.7) | 8 (9.4) | NA | NA | NA | | Ejaculatory function | 55 (65.5) | 27 (32.1) | 0 (0) | NA | NA | NA | 60 (70.6) | 38 (44.7) | 4 (4.7) | NA | NA | NA | 71 (83.5) | 42 (49.4) | 7 (8.2) | NA | NA | NA | | Sexual satisfaction | 62 (73.8) | 44 (52.4) | 4 (4.8) | 18 (75.0) | 15 (62.5) | 6 (25.0) | 60 (70.6) | 50 (58.8) | 10 (11.8) | 22 (91.7) | 15 (62.5) | 8 (33.3) | 70 (82.4) | 62 (72.9) | 6 (7.1) | 23 (92.0) | 15 (60.0) | 9 (36.0) | | Sexual desire | NA | NA | NA | 17 (70.8) | 13 (54.2) | 5 (20.8) | NA | NA | NA | 20 (83.3) | 16 (66.7) | 9 (37.5) | NA | NA | NA | 22 (88.0) | 17 (68.0) | 8 (32.0) | | Sexual arousal | NA | NA | NA | 18 (75.0) | 12 (50.0) | 4 (16.7) | NA | NA | NA | 21 (87.5) | 12 (50.0) | 8 (33.3) | NA | NA | NA | 22 (88.0) | 15 (60.0) | 6 (24.0) | | Vaginal lubrication | NA | NA | NA | 13 (54.2) | 10 (41.7) | 4 (16.7) | NA | NA | NA | 18 (75.0) | 11 (45.8) | 6 (25.0) | NA | NA | NA | 17 (68.0) | 15 (60.0) | 8 (32.0) | | Orgasm | NA | NA | NA | 14 (58.3) | 9 (37.5) | 4 (16.7) | NA | NA | NA | 16 (66.7) | 13 (54.2) | 6 (25.0) | NA | NA | NA | 18 (72.0) | 15 (60.0) | 6 (24.0) | | Pain | NA | NA | NA | 11 (45.8) | 7 (29.2) | 2 (8.3) | NA | NA | NA | 13 (54.2) | 11 (45.8) | 3 (12.5) | NA | NA | NA | 15 (60.0) | 10 (40.0) | 3 (12.0) |
|
|
Summary of post-procedural negative effect on various domains of sexual function as assessed by BSFI (in males) and FSFI-6 (in females).
|
| Independent variables | Group 1 (n=108) | Group 2 (n=109) | Group 3 (n=110) | | Males (n=84) | Females (n=24) | Males (n=85) | Females (n=24) | Males (n=85) | Females (n=25) | | 1 week | 3 weeks | 12 weeks | 1 week | 3 weeks | 12 weeks | 1 week | 3 weeks | 12 weeks | 1 week | 3 weeks | 12 weeks | 1 week | 3 weeks | 12 weeks | 1 week | 3 weeks | 12 weeks | | Age | 0.855 | 0.222 | 0.093 | 0.957 | 0.454 | 0.029 | 0.564 | 0.137 | 0.681 | 0.393 | 0.941 | 0.014 | 0.210 | 0.335 | 0.232 | 0.398 | 0.653 | 0.909 | | APAIS score | 0.004 | 0.002 | 0.001 | 0.105 | 0.592 | 0.930 | 0.021 | 0.278 | 0.693 | 0.088 | 0.348 | 0.039 | 0.001 | 0.361 | 0.023 | 0.601 | 0.060 | 0.225 | | Pre-procedural sexual function score | 0.227 | 0.407 | 0.002 | 0.872 | 0.787 | 0.442 | 0.622 | 0.084 | 0.001 | 0.424 | 0.078 | 0.010 | 0.806 | 0.671 | 0.006 | 0.472 | 0.668 | 0.607 | | VNRS | 0.477 | 0.520 | 0.862 | 0.951 | 0.568 | 0.846 | 0.698 | 0.012 | 0.269 | 0.633 | 0.770 | 0.502 | 0.747 | 0.685 | 0.706 | 0.632 | 0.934 | 0.157 |
|
|
Summary of p-values obtained during regression analysis.
|
| [1] |
Agrawal MS. Controversies in endourology. Indian J Urol 2013; 29:193e4.
doi: 10.4103/0970-1591.117289
|
| [2] |
Giannarini G, Keeley FX Jr, Valent F, Manassero F, Mogorovich A, Autorino R, et al. Predictors of morbidity inpatients with indwelling ureteric stents: results of a prospective study using the validated Ureteric Stent Symptoms Questionnaire. BJU Int 2011; 107:648e54.
doi: 10.1111/j.1464-410X.2010.09482.x
pmid: 20590539
|
| [3] |
Sofer M, Yehiely R, Greenstein A, Bar-Yosef Y, Matzkin H, Chen J. Endourological procedures and sexual dysfunction: a prospective multivariate analysis. BJU Int 2012; 109:250e3.
doi: 10.1111/j.1464-410X.2011.10232.x
pmid: 21507192
|
| [4] |
Mosharafa A, Hamid MAE, Tawfik M, El Rzzak OA. Effect of endourological procedures on erectile function: a prospective cohort study. Int Urol Nephrol 2016; 48:1055e9.
doi: 10.1007/s11255-016-1274-3
pmid: 27023476
|
| [5] |
O’Leary MP, Fowler FJ, Lenderking WR, Barber B, Sagnier PP, Guess HA, et al. A brief male sexual function inventory for urology. Urology 1995; 46:697e706.
doi: 10.1016/S0090-4295(99)80304-5
pmid: 7495124
|
| [6] |
Isidori AM, Pozza C, Esposito K, Giugliano D, Morano S, Vignozzi L, et al. Development and validation of a 6-item version of the female sexual function index (FSFI) as a diagnostic tool for female sexual dysfunction. J Sex Med 2010; 7: 1139e46.
doi: 10.1111/j.1743-6109.2009.01635.x
|
| [7] |
Moerman N, van Dam FS, Muller MJ, Oosting H. The Amsterdam preoperative anxiety and information scale (APAIS). Anesth Analg 1996; 82:445e51.
doi: 10.1097/00000539-199603000-00002
pmid: 8623940
|
| [8] |
Miu MW, Martin A, Cyna AM. Postoperative pain and comfort scores: do they correlate? Anaesth Intensive Care 2019; 47: 435e41.
doi: 10.1177/0310057X19861985
|
| [9] |
Guha M, Banerjee H, Mitra P, Das M. The demographic diversity of food intake and prevalence of kidney stone diseases in the Indian continent. Foods 2019; 8:37. https://doi.org/10.3390/foods8010037.
doi: 10.3390/foods8010037
|
| [10] |
Agresti A, Finlay B. Statistical methods for the social sciences. New Jersey: Pearson Prentice Hall, Inc; 2009. p.609.
|
| [11] |
Das K, Rao TSS. A chronicle of sexuality in the Indian subcontinent. J Psychosexual Health 2019; 1:20e5.
doi: 10.1177/2631831818822017
|
| [12] |
Prakash O, Rao TS. Sexuality research in India: an update. Indian J Psychiatr 2010; 52(Suppl 1):S260e3. https://doi.org/10.4103/0019-5545.69243.
|
| [13] |
Jejeebhoy S, Santhya K, Zavier A. Sexual and reproductive health in India. Oxford Research Encyclopedia of Global Public Health. https://doi.org/10.1093/acrefore/9780190632366.013.225. [Accessed17Jun.2021].
|
| [14] |
Lu J, Lu Y, Xun Y, Chen F, Wang S, Cao S. Impact of endourological procedures with or without double-J stent on sexual function: a systematic review and meta-analysis. BMC Urol 2020; 20:13. https://doi.org/10.1186/s12894-020-0582-1.
doi: 10.1186/s12894-020-0582-1
pmid: 32059655
|
| [15] |
Kazmi Z, Umer D, Ather MH. The effect of ureteric stenting on female sexual function: a prospective cohort study. Cureus 2020; 12:e11075. https://doi.org/10.7759/cureus.11075.
|
| [16] |
Fawzi R, Ali Z. Association of JJ stent insertion and sexual function: a cohort study [version 1; peer review: 1 approved with reservations]. F1000Research 2018;7:1978. https://doi.org/10.12688/f1000research.16608.1.
|
| [17] |
Akdeniz E, Bolat MS. Ureterorenoscopy with stenting and its effect on female sexual function. Urol J 2017; 14:3059e63.
pmid: 28537043
|
| [18] |
Eryildirim B, Tuncer M, Kuyumcuoglu U, Faydaci G, Tarhan F, Ozgül A. Do ureteral catheterisation procedures affect sexual functions? A controlled prospective study. Andrologia 2012; 44: S419e23. https://doi.org/10.1111/j.1439-0272.2011.01199.x.
|
| [19] |
Sofer M, Yehiely R, Greenstein A, Bar-Yosef Y, Matzkin H, Chen J. Endourological procedures and sexual dysfunction: a prospective multivariate analysis. BJU Int 2012; 109: 250e3.
doi: 10.1111/j.1464-410X.2011.10232.x
pmid: 21507192
|
| [20] |
Shah B, Juwono T, Uichanco L, Fisher J, Patel T. MP36-11 Ureteroscopydis the risk of erectile dysfunction a consideration? J Endourol 2016; 30:S2. https://liebertpub.com/doi/full/10.1089/end.2016.29020.abstracts.
doi: 10.1089/end.2015.0705
|
| [21] |
Eryildirim B, Tuncer M, Sahin C, Yucetas U, Sarica K. Evaluation of sexual function in patients submitted to ureteroscopic procedures. Int Braz J Urol 2015; 41:791e5.
doi: 10.1590/S1677-5538.IBJU.2014.0353
pmid: 26401873
|
| No related articles found! |
|
|
|
|