|
|
|
| Necrosis zone depth after bipolar plasma vaporization and resection in the human prostate |
Clara Breitlinga,Hans Nenningb,Jörg Rasslera,*( ) )
|
aDepartment of Urology, St. Elisabeth Hospital, Leipzig, Germany
bInstitute for Pathology “Am Elsapark”, Leipzig, Germany |
|
|
|
|
Abstract Objectives: To compare the depth of thermal necrosis after use of bipolar resection and vaporization technique comparing intra-individually bipolar loop and bipolar button electrodes.
Methods: Transurethral resection and vaporization of the prostate was performed in 55 male patients (260 specimens in total). In a standardized procedure, a bipolar resection loop was used for resection, and a bipolar button electrode was used for vaporization. Both electrodes were applied in each patient, either in the left or in the right lateral lobe. The depth of necrotic zones in the resected or vaporized tissue of each patient was measured in a standardized way by light microscopy.
Results: The mean depth with standard deviation of thermal injury caused by the loop electrode was 0.0495±0.0274 mm. The vaporization electrode caused a mean thermal depth with standard deviation of 0.0477±0.0276 mm. The mean difference of necrosis zone depths between the two types of electrodes (PlasmaButton-resection loop) was −0.0018 mm (p=0.691).
Conclusion: For the first time, we present directly measured values of the absolute necrosis zone depth after application of plasma in the transurethral treatment of benign prostatic hyperplasia. The measured values were lower than in all other transurethral procedures. Standardized procedures of measurement and evaluation allow a statistically significant statement that the low necrosis depth in bipolar procedures is independent of the applied electrodes.
|
|
Received: 21 December 2020
Available online: 20 April 2023
|
|
Corresponding Authors:
Jörg Rassler
E-mail: Joerg_Rassler@t-online.de
|
|
|

| Parameter | Value | | Agea, year | 71.7±7.1 | | Group 1b,c | 29 (52.7) | | Group 2b,c | 26 (47.3) | | BMIa, kg/m2 | 26.47±3.99 | | PSAa, ng/mL | 4.69±3.62 | | Prostate volumea, cm3 | 70.42±33.76 | | Intake of 5alpha-reductase inhibitor (dutasteride or finasteride)b | 11 (20.0) | | Intake of alpha1-inhibitor (tamsulosin)b | 13 (23.6) | | Intake of combined 5alpha-reductase-inhibitor and alpha1-inhibitorb | 5 (9.1) | | No prostate-specific medicationb | 26 (47.3) | | Blood clotting inhibitor (acetylsalicylic acid)b | 16 (29.1) | | Positive family history for PCab | 1 (1.8) |
|
|
Patients' data (n=55).
|

|
|
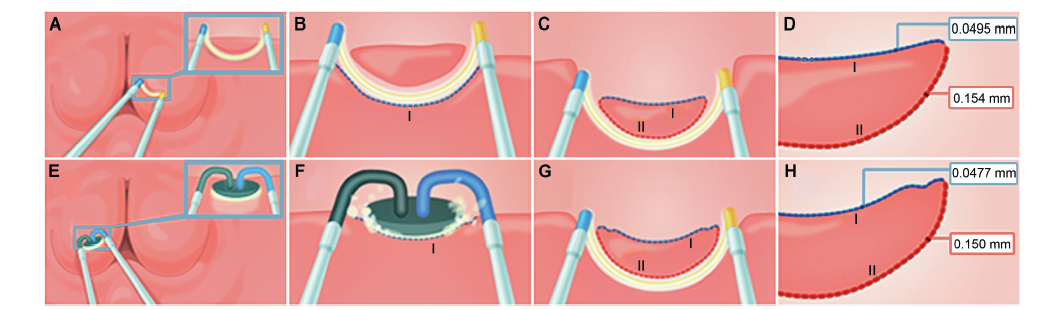
Schematic explanation of the two procedures. Resection (top; A-D): a mucosa-free layer of one lateral lobe was resected with the loop (A) forming a standardized resection area (side Ⅰ; B); those specimens were not used for the study and were rinsed out; from the standardized resection area (side Ⅰ) the study specimens were taken with the resection loop (C). Vaporization (bottom; E-H): the other lateral lobe was vaporized with the PlasmaButton on the mucosa-free area (side Ⅰ; F); from this vaporization area study specimens were taken using the resection loop (G); the specimen surface (side Ⅰ) represents the area, which would remain inside the patient. The specimens were collected for histopathological examination and measurement of necrosis depth on sides Ⅰ and Ⅱ. The numbers in the red and blue boxes represent the mean necrosis zone depths (D and H).
|
|
|
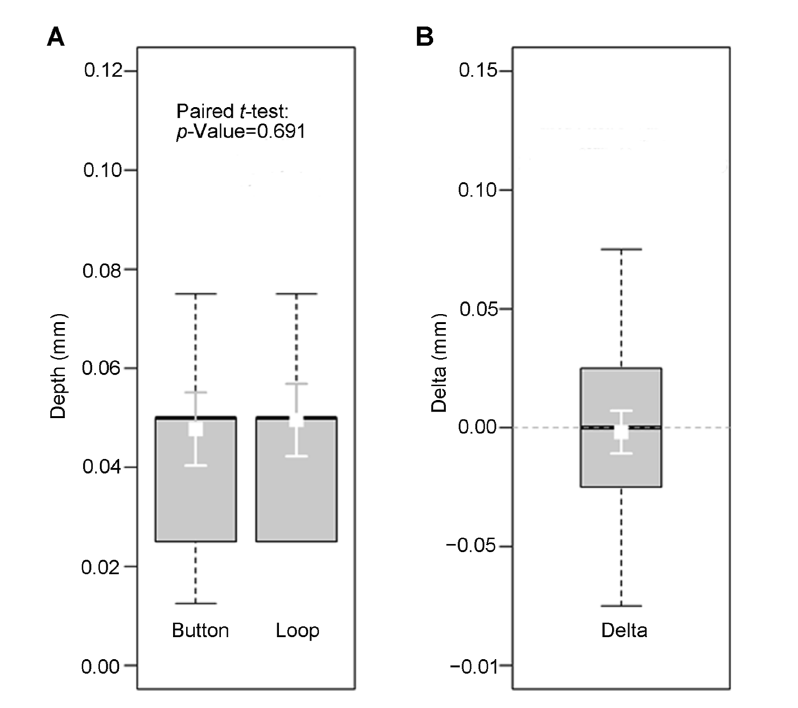
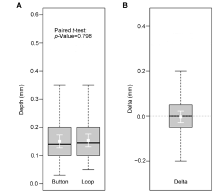
Necrotic zone depths at the concave side (side Ⅰ). (A) Absolute depth values in both methods (Button and Loop, respectively; in millimeter). (B) Difference (Delta) of the necrotic zone depths at side Ⅰ between PlasmaButton and resection loop (in millimeter). Boxes represent the interquartile range with the bold lines representing the medians and the whiskers the 10th/90th percentiles. The white squares and error bars in the boxes show the mean values ± 95% confidence intervals. The mean difference (PlasmaButton-resection loop; in millimeter) was with ?0.0018 mm not significant (paired t-test: p=0.691).
|
|
|
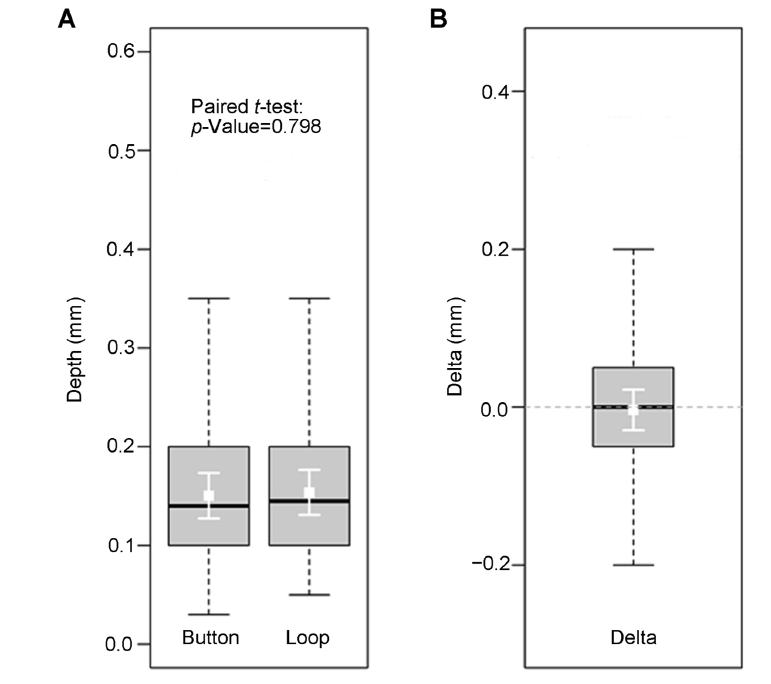
Necrotic zone depths at the convex side (side Ⅱ). (A) Absolute depth values in both methods (Button and Loop, respectively; in millimeter). (B) Difference (Delta) of the necrotic zone depths at side Ⅱ between PlasmaButton and resection loop (in millimeter). Boxes represent the interquartile range with the bold lines representing the medians and the whiskers the 10th/90th percentiles. The white squares and error bars in the boxes show the mean values ± 95% confidence intervals. The mean difference (PlasmaButton-resection loop; in millimeter) was with ?0.003 mm not significant (paired t-test: p=0.798).
|
| [1] |
Bschleipfer T, Bach T, Berges R, Dreikorn K, Gratzke C, Madersbacher S, et al. [S2e-Leitlinie der Deutschen Urologen. Instrumentelle Therapie des benignen Prostatasyndroms]. Urologe 2016; 55:195-207. [Article in German].
doi: 10.1007/s00120-015-3983-0
|
| [2] |
Lokeshwar SD, Harper BT, Webb E, Jordan A, Dykes TA, Neal Jr DE, et al. Epidemiology and treatment modalities for the management of benign prostatic hyperplasia. Transl Androl Urol 2019; 8:529-39.
doi: 10.21037/tau.2019.10.01
pmid: 31807429
|
| [3] |
Alexander CE, Scullion MM, Omar MI, Yuan Y, Mamoulakis C, N’Dow JM, et al. Bipolar versus monopolar transurethral resection of the prostate for lower urinary tract symptoms secondary to benign prostatic obstruction. Cochrane Database Syst Rev 2019; 12:CD009629. https://doi.org/10.1002/14651858.CD009629.pub4.
|
| [4] |
Rieken M, Herrmann TRW, Füllhase C. [Surgical treatment of benign prostatic hyperplasiadresection, vaporization or enucleation?]. Urologe 2019; 58:263-70. [Article in German].
doi: 10.1007/s00120-019-0891-8
|
| [5] |
Singh H, Desai MR, Shrivastav P, Vani K. Bipolar versus monopolar transurethral resection of prostate: randomized controlled study. J Endourol 2005; 19:333-8.
doi: 10.1089/end.2005.19.333
pmid: 15865523
|
| [6] |
Maddox M, Pareek G, Al Ekish S, Thavaseelan S, Mehta A, Mangray S, et al. Histopathologic changes after bipolar resection of the prostate: depth of penetration of bipolar thermal injury. J Endourol 2012; 26:1367-71.
doi: 10.1089/end.2012.0202
pmid: 22577984
|
| [7] |
Akgül T, Nuho?lu B, Polat O, Ayyildiz A, Astarci M, Germiyano?lu C, et al.An in vitro study comparing the coagulation and cautery effects of bipolar and unipolar cutting modalities on prostatic tissue. Urol Int 2009; 83:458-62.
doi: 10.1159/000251188
pmid: 19996655
|
| [8] |
Ko R, Tan AHH, Chew BH, Rowe PE, Razvi H. Comparison of the thermal and histopathological effects of bipolar and monopolar electrosurgical resection of the prostate in a canine model. BJU Int 2010; 105:1314-7.
doi: 10.1111/j.1464-410X.2009.08907.x
pmid: 19817746
|
| [9] |
Kan CF, Chan ACL, Pun CT, Ho LY, Chan SW, Au WH. Heat damage zones created by different energy sources used in the treatment of benign prostatic hyperplasia in a pig liver model. J Endourol 2015; 29:714-7.
doi: 10.1089/end.2014.0665
pmid: 25353613
|
| [10] |
Huang X, Wang XH, Wang HP, Shi HB, Zhang XJ, Zhou J, et al. Bipolar transurethral resection of the prostate versus monopolar transurethral prostatectomy: a pathological study in a canine model. Zhonghua Nan ke Xue 2010; 16:712-5.
|
| [11] |
Huang X, Wang L, Wang XH, Shi HB, Zhang XJ, Yu ZY. Bipolar transurethral resection of the prostate causes deeper coagulation depth and less bleeding than monopolar transurethral prostatectomy. Urology 2012; 80:1116-20.
doi: 10.1016/j.urology.2012.07.024
pmid: 22990062
|
| [12] |
Qu L, Wang X, Huang X, Zhang Y, Zeng X. Use of a novel ex-vivo model to compare the hemostatic properties of plasmakinetic resection, transurethral vaporization resection and conventional transurethral resection of the prostate. Urology 2007; 70:1034-8.
pmid: 18068481
|
| [13] |
Rassler J, Berthold KL, Kempter JU. V66 Transurethral mechanical enucleation and bipolar resection of the prostate (TUER-P). Eur Urol Suppl 2014; 13:eV66. https://doi.org/10.1016/S1569-9056(14)61195-7.
doi: 10.1016/S1569-9056(14)61195-7
|
| [14] |
Huang X, Wang XH, Wang HP, Qu LJ. Comparison of the microvessel diameter of hyperplastic prostate and the coagulation depth achieved with mono- and bipolar transurethral resection of the prostate. A pilot study on hemostatic capability. Scand J Urol Nephrol 2008; 42:265-8.
doi: 10.1080/00365590701702168
pmid: 17934987
|
| [15] |
Bach T, Herrmann TR, Cellarius C, Geavlete B, Gross AJ, Jecu M. Bipolar resection of the bladder and prostatedinitial experience with a newly developed regular sized loop resectoscope. J Med Life 2009; 2:443-6.
|
| [16] |
Akgül KT, Ayyildiz A, Nuho?lu B, Caydere M, Ustün H, Germiyano?lu C. Comparison of transurethral prostate resection and plasmakinetic prostate resection according to cautery artefacts in tissue specimens. Int Urol Nephrol 2007; 39: 1091-6.
doi: 10.1007/s11255-007-9174-1
pmid: 17431812
|
| [17] |
Kwon JS, Lee JW, Lee SW, Choi HY, Moon HS. Comparison of effectiveness of monopolar and bipolar transurethral resection of the prostate and open prostatectomy in large benign prostatic hyperplasia. Korean J Urol 2011; 52:269-73.
doi: 10.4111/kju.2011.52.4.269
pmid: 21556214
|
| [18] |
Hirik E, Bozkurt A, Karabakan M, Aydemir H, Aktas BK, Nuho?lu B. Safety and efficacy of bipolar versus monopolar transurethral resection of the prostate: a comparative study. Urol J 2015; 12:2452-6.
pmid: 26706745
|
| [19] |
Bhansali M, Patankar S, Dobhada S, Khaladkar S. Management of large (>60 g) prostate gland: plasma kinetic superpulse (bipolar) versus conventional (monopolar) transurethral resection of the prostate. J Endourol 2009; 23:141-5.
doi: 10.1089/end.2007.0005
pmid: 19178175
|
| [20] |
Alkatout I, Schollmeyer T, Hawaldar NA, Sharma N, Mettler L. Principles and safety measures of electrosurgery in laparoscopy. J Soc Laparoendosc Surg 2012; 16:130-9.
doi: 10.4293/108680812X13291597716348
|
| [21] |
Bach T, Muschter R, Sroka R, Gravas S, Skolarikos A, Herrmann TR, et al. Laser treatment of benign prostatic obstruction: basics and physical differences. Eur Urol 2012; 61: 317-25.
doi: 10.1016/j.eururo.2011.10.009
pmid: 22033173
|
| [1] |
Rajiv N. Kore. Management of urethral strictures and stenosis caused by the endo-urological treatment of benign prostatic hyperplasia—a single-center experience[J]. Asian Journal of Urology, 2023, 10(2): 137-143. |
| [2] |
Kalpesh Parmar,Ashish Khanna,Shrawan Kumar Singh,Manjeet Sharma. A rare cause of acute urinary retention— Primary malignant melanoma of prostate[J]. Asian Journal of Urology, 2019, 6(4): 380-382. |
| [3] |
S.J.Chung Amanda,H.Woo Henry. Update on minimally invasive surgery and benign prostatic hyperplasia[J]. Asian Journal of Urology, 2018, 5(1): 22-27. |
| [4] |
Jonathan Shunming Teo, Yee Mun Lee, Henry Sun Sien Ho. An update on transurethral surgery for benign prostatic obstruction[J]. Asian Journal of Urology, 2017, 4(3): 195-198. |
|
|
|
|