|
|
|
| Radical cystoprostatectomy with orthotopic neobladder for a case of treatment emergent neuroendocrine prostate cancer presenting as bladder mass with hematuria-a rare instance of tumor remission after local control |
Rahul Jena*( ),Hira Lal,Nandita Chaudhary ),Hira Lal,Nandita Chaudhary
|
Uday Pratap Singh Department of Urology and Renal Transplant, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India
Department of Radiodiagnosis, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India
Department of Pathology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India |
|
|
|
|
Abstract Treatment emergent neuroendocrine prostate cancer (t-NEPC) is most commonly observed after development of resistance to androgen deprivation therapy (ADT) and is associated with rapid progression and widespread metastases with survival less than 1 year from diagnosis [1]. Management of this disease is mainly through cytotoxic chemotherapy and there is no published evidence of treating the primary prostatic lesion in this stage of the disease, unlike that of localized prostate cancer or castrate sensitive metastatic prostate cancer [2]. In this letter, we report the only known case of t-NEPC who presented with an initial diagnosis of bladder urothelial carcinoma and was treated by early radical surgery and chemotherapy, which led to long-term disease control and preservation of quality of life.
|
|
Available online: 20 October 2021
|
|
Corresponding Authors:
Rahul Jena
E-mail: jena.rahul@gmail.com
|
|
|
|
|
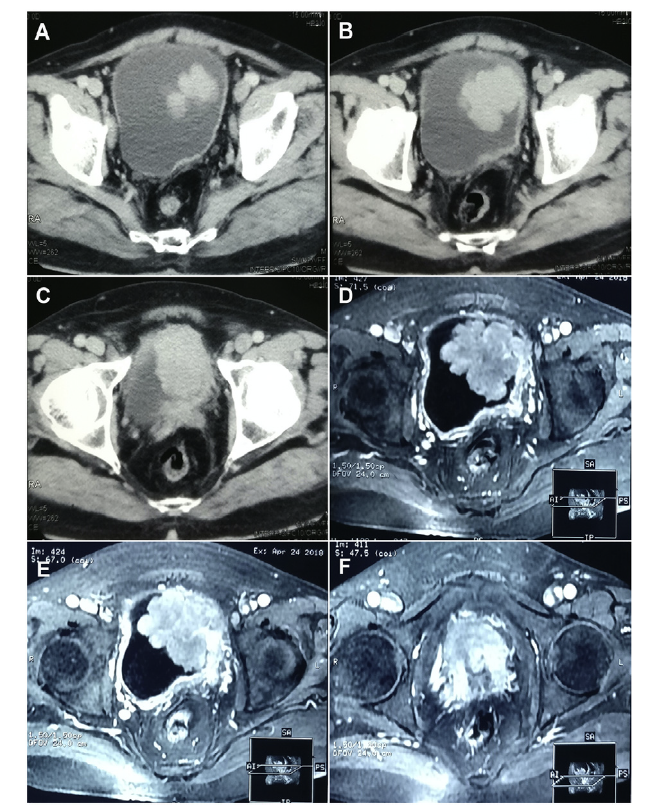
Cross sectional imaging showing locally advanced bladder tumour involving the prostate also. (A-C) Serial sections of contrast enhanced computed tomography images showing enhancing polypoidal intraluminal mass arising from the left lateral wall of the urinary bladder; (D-F) Magnetic resonance images showing the polypoidal mass arising from the urinary bladder wall and contiguous with the prostatic mass below. The seminal vesicles were involved bilaterally and bilateral pelvic lymph nodes are enlarged.
|
|
|
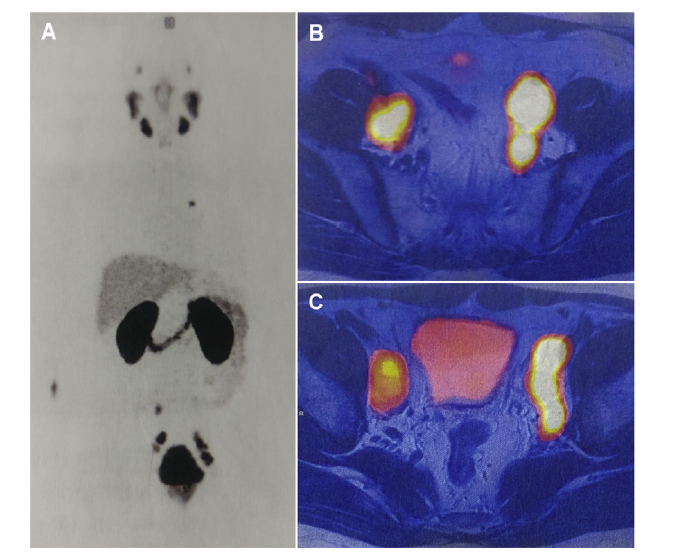
PSMA PET scan images. (A) Maximum intensity projection images showing a single area of uptake in the aortopulmonary node which was later shown to be inflammatory in nature based on its tracer avidity; (B and C) PSMA PET scan showing bilateral PSMA avid pelvic lymphadenopathy. PSMA PET, prostate-specific membrane antigen ositron emission tomography.
|
|
|
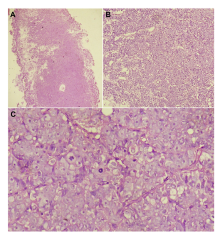
Sections of histopathological examination of the transurethral biopsy specimen. (A) HE stained sections 100×magnification, Low power view showing tumour infiltrating the prostate; (B) Tumour arranged in nests separated by thin fibrovascular septae (HE stain, 200×magnification); (C) Oil immersion view showing moderately pleomorphic tumour cells with prominent nucleoli and brisk mitotic activity (HE stain, 1000×magnification). HE, hematoxylin and eosin.
|
|
|
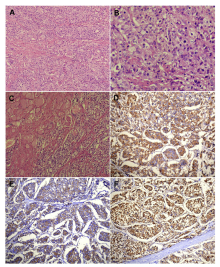
HE and immunohistochemistry stained sections of the tumour from the resected surgical specimen. Top row: Mildly pleomorphic to isomorphic tumour cells arranged in nested configuration (200×magnification) (A); Tumour cells showing moderate nuclear atypia (400×magnification) (B); Periprostatic skeletal muscle infiltration by the tumour (200×magnification) (C). Bottom row (200×magnification): Microphotographs showing positive immunostaining for synaptophysin (D), chromogranin (E), and prostate-specific antigen (F). HE, hematoxylin and eosin.
|
| [1] |
Wang HT, Yao YH, Li BG, Tang Y, Chang JW, Zhang J. Neuro-endocrine prostate cancer (NEPC) progressing from conven-tional prostatic adenocarcinoma: Factors associated with time to development of NEPC and survival from NEPC diagnosisda systematic review and pooled analysis. J Clin Oncol 2014; 32:3383e90.
|
| [2] |
Flechon A, Pouessel D, Ferlay C, Perol D, Beuzeboc P, Gravis G, et al. Phase II study of carboplatin and etoposide in patients with anaplastic progressive metastatic castration-resistant prostate cancer (mCRPC) with or without neuroen-docrine differentiation: Results of the French Genito-Urinary Tumor Group (GETUG) P01 trial. Ann Oncol 2011; 22:2476e81.
|
| [3] |
Ryan CJ, Smith MR, De Bono JS, Molina A, Logothetis CJ, De Souza P, et al. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med 2013; 368:138e48.
|
| [4] |
Beer TM, Armstrong AJ, Rathkopf DE, Loriot Y, Sternberg CN, Higano CS, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med 2014; 371:424e33.
|
| [5] |
Bishop JL, Davies A, Ketola K, Zoubeidi A. Regulation of tumor cell plasticity by the androgen receptor in prostate cancer. Endocr Relat Canc 2015;22:R165e82. https://doi.org/10.1530/ERC-15-0137.
|
| [6] |
Nouri M, Caradec J, Lubik AA, Li N, Hollier BG, Takhar M, et al. Therapy-induced developmental reprogramming of prostate cancer cells and acquired therapy resistance. Oncotarget 2017;8:18949. https://doi.org/10.18632/oncotarget.14850.
|
| [7] |
Small EJ, Aggarwal RR, Huang J, Sokolov A, Zhang L, Alumkal JJ, et al. Clinical and genomic characterization of metastatic small cell/neuroendocrine prostate cancer (SCNC) and intermediate atypical prostate cancer (IAC): Results from the SU2C/PCF/AACRWest Coast Prostate Cancer Dream Team (WCDT). J Clin Oncol 2016;34:5019. https://doi.org/10.1200/JCO.2016.34.15_suppl.5019.
|
| [8] |
Nadal R, Schweizer M, Kryvenko ON, Epstein JI, Eisenberger MA. Small cell carcinoma of the prostate. Nat Rev Urol 2014;11:213. https://doi.org/10.1038/nrurol.2014.21.
|
| [9] |
Aggarwal R, Huang J, Alumkal JJ, Zhang L, Feng FY, Thomas GV, et al. Clinical and genomic characterization of treatment-emergent small-cell neuroendocrine prostate can-cer: A multi-institutional prospective study. J Clin Oncol 2018; 36:2492. https://doi.org/10.1200/JCO.2017.77.6880.
|
| [10] |
Aparicio AM, Harzstark AL, Corn PG, Wen S, Araujo JC, Tu SM, et al. Platinum-based chemotherapy for variant castrate-resistant prostate cancer. Clin Cancer Res 2013; 19:3621e30.
|
| [11] |
Turina CB, Coleman DJ, Thomas GV, Fung AW, Alumkal JJ. Molecular testing identifies determinants of exceptional response and guides precision therapy in a patient with lethal, treatment-emergent neuroendocrine prostate cancer. Cureus 2019;11. https://doi.org/10.7759/cureus.5197.
|
| [12] |
Culine S, El Demery M, Lamy PJ, Iborra F, Avances C, Pinguet F. Docetaxel and cisplatin in patients with metastatic androgen independent prostate cancer and circulating neuroendocrine markers. J Urol 2007; 178:844e8.
|
| [13] |
Papandreou CN, Daliani DD, Thall PF, Tu SM, Wang X, Reyes A, et al. Results of a phase II study with doxorubicin, etoposide, and cisplatin in patients with fully characterized small-cell carcinoma of the prostate. J Clin Oncol 2002; 20:3072e80.
|
| [14] |
Singh UP, Jena R, Madhavan Kumar, Kumar N, Sureka SK, Srivastava A. Radical cystectomy and W-shaped ileal ortho-topic neobladder reconstruction with serosa-lined tunneled ureteroileal anastomoses: A critical analysis of the short-term voiding patterns and urodynamic and functional outcomes. Indian J Urol 2019;35:121. https://doi.org/10.4103/iju.IJU_356_18.
|
| [15] |
Boevé LM, Hulshof MC, Vis AN, Zwinderman AH, Twisk JW, Witjes WP, et al. Effect on survival of androgen deprivation therapy alone compared to androgen deprivation therapy combined with concurrent radiation therapy to the prostate in patients with primary bone metastatic prostate cancer in a prospective randomised clinical trial: Data from the HORRAD trial. Eur Urol 2019; 75:410e8.
|
| [16] |
Sooriakumaran P. Testing radical prostatectomy in men with prostate cancer and oligometastases to the bone: A random-ized controlled feasibility trial. BJU Int 2017;120:E8e20. https://doi.org/10.1111/bju.13925.
|
| No related articles found! |
|
|
|
|